

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The Guideline Working Group of Korean Society for Neuro-Oncology (KSNO) conducted a nationwide questionnaire survey on the clinical practice about several topics of brain tumor. The intent of this survey study is described in the previous article of the series in this issue. As part II of the survey, this study deals with practical decisions of specific brain tumors, such as diffuse midline glioma and meningioma.
Diffuse midline glioma is known to be one of dismal highgrade pediatric and adult brain tumors involving midline structures of the central nervous system. In general, most of these tumors are inoperable because of challenging anatomic location, which makes the prognosis even worse to the overall survival no more than 12 months [123]. There were few randomized controlled clinical trials to establish the evidence-based standard treatment protocol. Despite several therapeutic options including radiotherapy, chemotherapy and/or surgery, no superior treatment modalities could be recommended alone or in combination [456]. In addition, 2016 revised World Health Organization (WHO) classification recently redefined this type of tumors as diffuse midline glioma, H3K27M mutant, a new diagnostic entity based on its unique genetic signature [7]. So, evidence-based and consensus guideline from diagnosis to treatment for this entity is required.
Meningiomas are the most common primary brain tumors. The data from Korean Cancer Registration Statistics Program in 2013 shows that the incidence of meningioma was 37.3% of newly diagnosed brain tumors with median age at diagnosis of 61 years in Korea [8]. Recently, the incidence of meningioma is continuously increasing due to the discovery of incidental meningiomas from expanded inclusion of neuroimaging in routine health check-ups [91011]. However, the management strategy for incidental meningiomas is controversial among neurosurgeons [1213141516]. Meningiomas were histologically classified into three grades by WHO definition from grade I to III. The definition of atypical meningioma (WHO grade II) from 2016 revised WHO classification includes histologically confirmed brain invasion [7]. Contrast to grade I and grade III meningiomas, the adjuvant treatment after surgical resection for grade II meningiomas remains debating issue among physicians. Some studies reported that adjuvant radiotherapy after neurosurgical resection decreased the recurrence rates and improved overall survival [1718]. However, there are also other studies describing no benefit in recurrence and survival of adjuvant radiotherapy at the cost of its risk of radiation-induced toxicity [1920].
The aim of this study is to evaluate the tendencies of clinical practice for patients with diffuse midline glioma and meningioma from the nationwide survey in Korea.
Go to : 
MATERIALS AND METHODS
The details of the study design, outline, and implementation are described in the previous article of the series in this issue. Here, the questionnaires about diffuse midline glioma (4 questions) and meningioma (6 questions) were structured around existing controversies regarding real clinical management in patients (Appendix).
Regarding the diffuse midline glioma, the questionnaires were focused on the diagnosis and treatment options in clinical practices. The dose and target of radiotherapy that considered as the significant treatment option were also investigated.
The questionnaires of meningioma included 2 case scenarios asking the management options for the patients with asymptomatic meningioma with different age and radiological finding of the tumor. Other questionnaire consisted of follow-up MRI schedules for asymptomatic meningioma, adjuvant treatment of WHO grade II meningioma according to the extent of surgical resection, adjuvant radiation dose of WHO grade II meningioma after surgical resection, and experience of medical treatment for patients with meningioma.
Go to :
RESULTS
Diffuse midline glioma
About three quarters of the respondents performed the diagnostic confirmation to identify the H3K27M mutation (n=36, 72%) by the immunohistochemical (IHC) staining or the pathognomonic K27M mutation (n=20, 40%) in the histone 3.3 (H3.3) gene H3F3A, histone 3.2 (H3.2) gene HIST2H3C, and histone 3.1 (H3.1) genes HIST1H3B/C using sequencing methods. Twelve respondents (24%) diagnosed the diffuse midline glioma by using only radiologic findings without detection of H3K27M mutation.
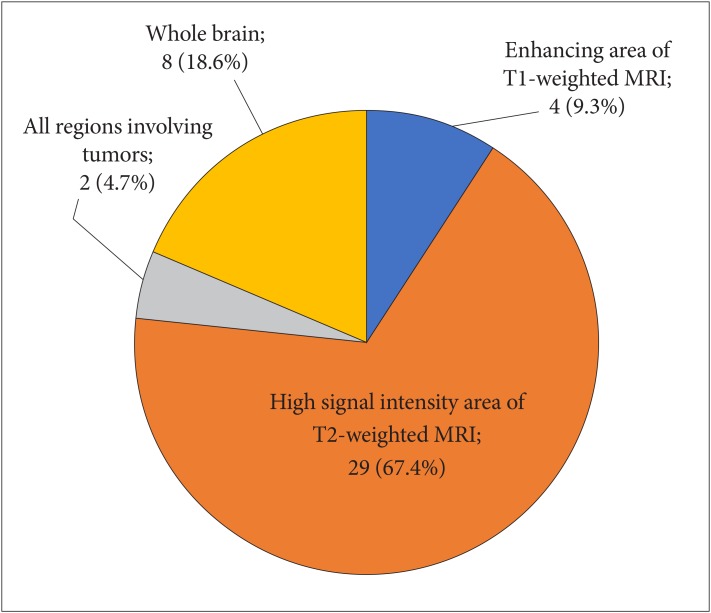
For treatment of diffuse midline glioma, 30 of 47 (63.8%) respondents performed the concurrent chemoradiotherapy with temozolomide (TMZ) and adjuvant TMZ, and 16 respondents (34.0%) treated the patient with radiotherapy alone. One respondent reported that if surgically total resection was performed, no further treatment was given. For radiation dose, 42 of 45 (93.4%) respondents mostly delivered 54–60 Gy in 27–30 fractions. Two (4.4%) respondents delivered 45 Gy in 25 fractions, and one (2.2%) respondent stated in free text response that the radiation dose was decided according to location of lesions (i.e., 54 Gy in 30 fractions for brainstem lesion and 60 Gy in 30 fractions for the others). The target coverage of radiotherapy showed that mainly focused on the high signal intensity lesion of T2-weighted MRI (Fig. 1).
Meningioma
We asked the decision on initial management plan for incidentally found asymptomatic meningiomas based on case scenarios. The preference of treatment modality for a 45-year-old woman with small (3 cm in diameter) meningioma was quite variable according to tumor location and presence of peritumoral edema (Fig. 2). For frontal convexity meningioma without peritumoral edema, respondents preferred observation with serial MRI follow-up, but for patients with peritumoral edema, surgical resection was preferred. For patients with parasagittal meningioma around the motor cortex, respondents preferred the surgical resection regardless of peritumoral edema. If the tumor was located at skull base, the decision was quite similar to that of frontal convexity tumor, but the role of radiosurgery was emphasized all the more. However, the majority of respondents opted for surgical resection for a 70-year-old woman with meningioma with larger tumor (6 cm in diameter) regardless of tumor location and peritumoral edema (Fig. 2). The responses of case scenarios showed that the radiologic findings, such as tumor location, tumor size, and peritumoral edema, were considered more important factors than age of patient in determining treatment strategies of asymptomatic meningioma.
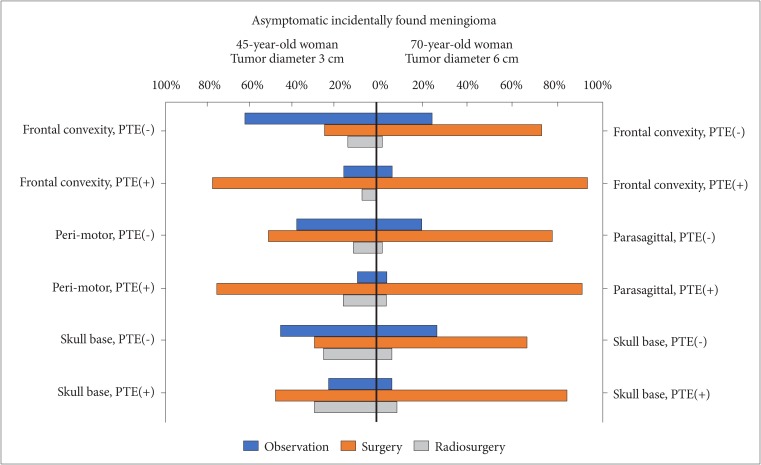
Fig. 3 shows responses about radiological follow-up plans for patients with asymptomatic meningioma by each respondent. Among 45 respondents who answered to have follow-up plans, 12 respondents (26.7%) had no long-term plans for radiological follow-up after a year if the tumor is stable. We could find that every respondent has different ideas on follow-up plans for the meningiomas with observation policy. There was no single opinion with major consensus on long-term follow-up plans.
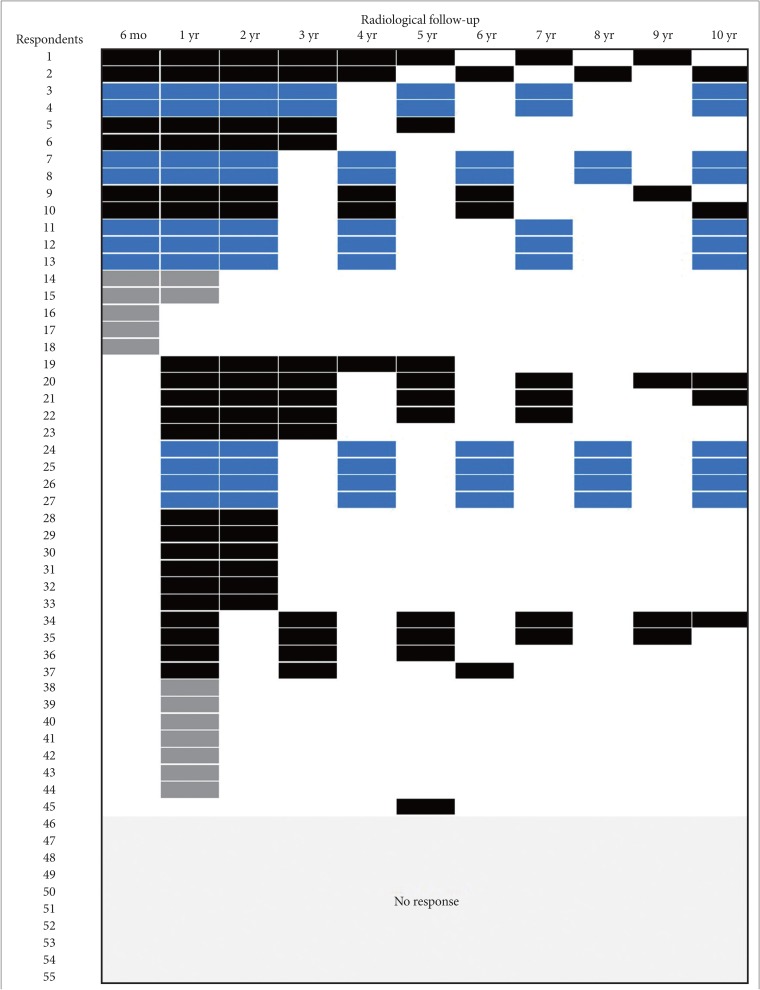 | Fig. 3Responses about radiological follow-up plans for patients with asymptomatic meningioma by each respondent. Colored cells are time points to study. Responses with blue cells are answers with any consensus for long-term follow-up plans, while those with grey cells are with no plan for long-term follow ups after a year.
|
Among 47 respondents, 32 (68.1%) respondents choose observation with serial MRI follow-up without adjuvant treatment for patient with WHO grade II meningioma receiving complete tumor resection with removal of affected dura, while 14 (29.8%) respondents performed the radiotherapy and one (2.1%) respondent performed the radiosurgery. For patients with WHO grade II meningioma receiving complete tumor resection without removal of affected dura, 31 of 47 (66.0%) respondents performed the radiotherapy, and four (8.5%) respondents performed the radiosurgery. Twelve (25.5%) respondents choose observation without adjuvant treatment in this setting. For patient with WHO grade II meningioma with residual tumor after surgery, respondents choose the next plan as following: radiotherapy (n=34, 72.4%), radiosurgery (n=12, 25.5%), and observation without adjuvant treatment (n=1, 2.1%). Regarding the radiation dose given after surgical resection, 28 of 42 (66.7%) respondents delivered 54.0 Gy after surgical resection for WHO grade II meningioma. Ten (23.8%) respondents delivered 60.0 Gy and three (7.0%) delivered 58.8 Gy. In free text responses, one respondent stated that the radiation dose was decided according to whether performing complete tumor resection or not. Twelve respondents described their experiences of a medical treatment trial for patients with meningioma. The prescribed medications were the following: hydroxyurea (n=11); nimustine plus cisplatin (n=1); nitrosourea (n=1).
Go to :
DISCUSSION
The characteristic findings of diffuse midline glioma are known as K27M mutations in the histone H3 gene H3F3A, or less commonly in the related HIST1H3B gene, a diffuse growth pattern, and a midline location of brain (e.g., thalamus, brain stem, and spinal cord) [72122]. Because surgical resection is often difficult due to the location of the tumor, proper imaging and biopsy are required for accurate differential diagnosis. In this survey report, three-quarters of respondents consider that histologic confirmation of the H3K27M mutation is more important for diagnosis, based on the 2016 revised WHO classification [7]. This is in line with the diagnosis of diffuse midline glioma in the European Assocation for Neuro-Oncology guideline that recommends IHC of histone H3K27M mutation which characterizes diffuse midline glioma, histone H3K27M-mutant [23]. Therefore, if possible, the histologic confirmation of the H3K27M mutation would be considered as a diagnostic criterion.
Current treatment strategy for diffuse midline glioma is that conventional radiotherapy is the important therapeutic option due to the limitation of radical resection [2324]. The role of chemotherapy remains unclear. Several types of chemotherapeutic regimens such as carboplatin, etoposide, vincristine and TMZ have shown no evidence of survival improvement [2526272829]. Some physicians have used chemotherapy with or after radiotherapy following the standards of care for gliomas of the same WHO grade in other anatomical locations. EANO guideline recommends radiotherapy alone or TMZ plus radiotherapy followed by TMZ as first line treatment [23]. Our results also seem to reflect this situation in the real world. The standard radiation dose is 54–60 Gy with a daily conventional fractionation of 1.8–2.0 Gy [24]. Some studies for the altered fractionation schemes including the hypofractionation with shorter treatment duration or hyperfractionation with dose-escalation have shown no distinct survival benefit [12353031]. To overcome the limitation of few therapeutic options, there is a continuing need for new clinical trials to find a new therapeutic strategy and basic research to increase insight to diffuse midline glioma.
This nationwide survey study reflects various opinions on the treatment of asymptomatic meningioma and postoperative treatment of WHO grade II meningioma. There have been many reports about the strategy for asymptomatic meningiomas. The prospective study dealing with the natural history of incidental meningioma reported that asymptomatic tumors can be safely managed by imaging follow-up, although 75% of meningioma had slowly increased on observation period. It was also reported that the growth rate was significantly correlated with the tumor size and the age of patients [32]. Kim et al. [33] reported the comparison result of Gamma Knife surgery (GKS) versus observation in 354 patients with asymptomatic meningiomas. The clinical and radiologic progression-free survival rates at 10 years were 92.9% and 88.5% in GKS group, while those were 42.7% and 7.9% in observation group. Clinical progression was correlated with young age, absence of calcification, peritumoral edema, and high T2 signal intensity in the observation group [33]. In another report, 603 patients with asymptomatic meningiomas were respectively analyzed about the natural course and surgical outcome [16]. A total of 63% of asymptomatic meningiomas did not grow in follow up for longer than 5 years, and only 6% of all patients with these lesions showed symptoms during the observation period. Among the 213 patients underwent the neurosurgical resection, the morbidity rate was 4.4% in patients younger than 70 years of age and 9.4% in those 70 years of age or older, and those were lower compared with those in symptomatic patients [16]. Zeng et al. [34] reported that Simpson I resection rate was significantly high in the cerebral hemispheric tumor compared with skull base lesion (95.2% vs. 66.7%) in the patient with asymptomatic meningiomas. The surgical-related complication rate was 13.6%, which was lower than the rate of 21.7% in the symptomatic patients, and younger patients less than 60 years showed better outcome at 1 year after the operation. In the current survey, the respondents rather choose an aggressive treatment of neurosurgical resection or radiosurgery except for the situations with middle-aged patients having 3-cm-sized frontal convexity without peritumoral edema. The size of tumors rather than age and the peritumoral edema tended to be the determining factors whether to treat or not. Additionally, the neurosurgical resection was more preferred compared to radiosurgery as the treatment strategy in patients with asymptomatic meningiomas.
There have been several controversies in management of WHO grade II meningiomas, including the significance of extent of surgical resection, the postoperative radiotherapy, and chemotherapy. In the conclusion of previous review on these issues in non-benign meningiomas, gross total resection could improve outcome and should be attempted in grade II meningiomas [35]. They also reported that postoperative radiotherapy following gross total resection did not improve patient outcome of grade II meningioma, but radiotherapy improves outcome following subtotal tumor resection of grade II meningioma. Additionally, no drug therapy was not effective to improve outcome in non-benign meningiomas [35]. Sun et al. [36] reported the treatment algorithm based on the investigation of previous studies in WHO grade II meningiomas. They recommended that adjuvant radiotherapy could be considered when tumors showed high risk features, such as brain invasion, mitotic index ≥8, and sheeting, although gross total resection was performed. And stereotactic radiosurgery as well as radiotherapy could be suitable in the patients after subtotal resection [36]. In this study, there was the opposite opinion about the necessity of postoperative radiotherapy according to the presence of affected dura even if gross total resection was performed. However, respondents concurred with the previous results about the management following subtotal resection.
As with any online survey, the major limitation of this study is response bias that respondents might be influenced by the pressure to follow the published guidelines, especially in the survey of diffuse midline glioma because of a rare disease entity. Additionally, the relatively low response rate may give rise to sampling bias interfering with the valuable interpretation of several questions.
In conclusion, the survey demonstrates the variation and similarity of clinical practice for patients with diffuse midline glioma and meningioma among members of the KSNO. It is important to reduce the variation for establishing the guideline based on the best available evidence.
Go to :
 XML Download
XML Download