

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The incidence of metastatic brain tumors is increasing because systemic cancers are maintained longer by using new developing chemotherapeutic agents. Two common metastases to the brain are from lung cancer and breast cancer [123].
The rate of brain metastasis from non-small cell lung cancer (NSCLC) varies according to its pathology [4]. Brain metastases are found in approximately 25–30% of patients with NSCLC and their overall survival (OS) is about 4 months after whole brain radiation therapy, which varies based on several factors [56].
The development of targeted agents with promising results in the treatment of NSCLC has led to prolongation of life expectancy. Among the molecular diagnosis, epidermal growth factor receptor (EGFR) mutations are associated with significant sensitivity to EGFR tyrosine kinase inhibitors (TKI) which can improve outcomes in NSCLC patients who are treated with the targeted agent [7]. The patients with a metastatic brain tumor from NSCLC have been reported to have a better prognosis when they were treated with EGFR TKI agents [89]. However, there is still controversy about how EGFR TKI agents act on brain metastases from NSCLC and which effects produce the better clinical outcome after treating intracranial disease [1011]. Determining which factors improve the prognosis of the metastatic brain tumor patients is very important. For this study, we analyzed factors associated with intracranial disease prognosis in NSCLC patients undergoing radiosurgery for brain metastasis, primarily focusing on the effects of EGFR TKI.
Go to : 
MATERIALS AND METHODS
We retrospectively reviewed 184 Gamma Knife Radiosurgery (GKRS) procedures for brain tumors that metastasized from lung cancer from August 2010 to July 2017. The patients whose medical records were insufficient for analysis or those lost to follow-up were excluded. In total, 98 NSCLC patients was analyzed in this study. Table 1 shows the demographics of the patients enrolled in this study. We defined intracranial disease progression when a new intracranial lesion was found in follow-up brain image. So, we only included the first radiosurgery for the metastatic brain tumor for analysis because the patients who underwent a second radiosurgery had intracranial disease progression.
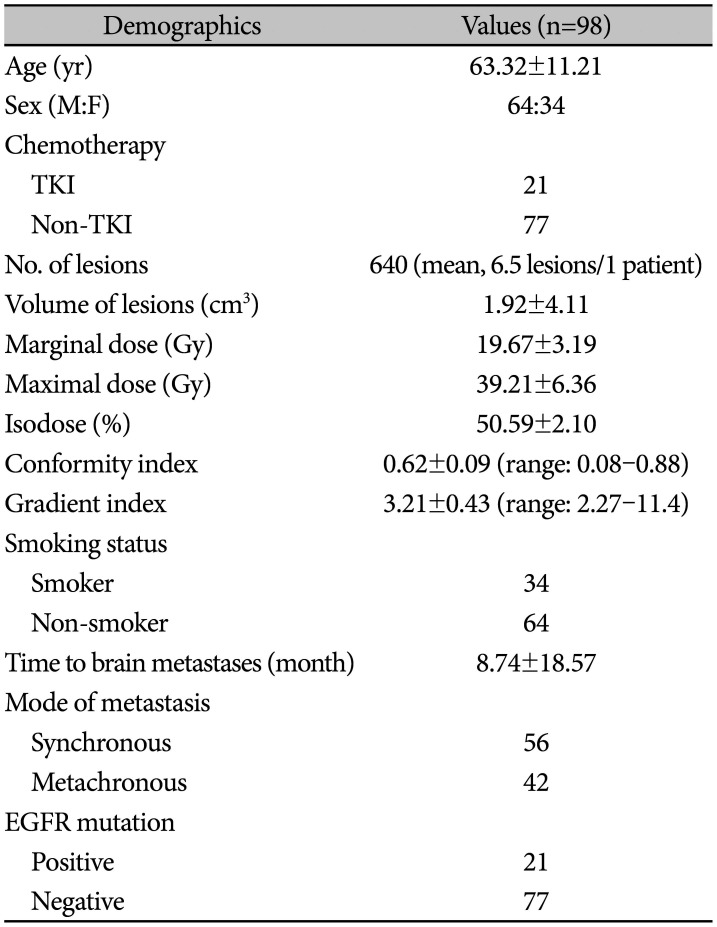
Table 1
Demographics of the patients with non-small cell lung cancer underwent Gamma Knife Radiosurgery
![]()
The mean age of the patients was 63.32±11.21 years. Male patients were 64 and females were 34. Thirty-four patients were smokers and 64 patients were non-smokers. There were 640 treated lesions and the mean lesion number for radiosurgery was 6.5. The median time to brain metastases after the diagnosis of systemic disease was 8.74±18.57 months. Intracranial diseases in 56 patients were diagnosed as synchronous with systemic disease and those in 42 patients were diagnosed as metachronous. Primary cancer pathologies were reported as adenocarcinoma (77 patients), squamous cell carcinoma (16 patients), sarcomatoid carcinoma (2 patients), and other types of carcinomas (3 patients). Primary disease pathologies and clinical status at initial diagnosis are shown in Table 2. EGFR studies were positive in 21 patients and negative in 77. Chemotherapy for the systemic disease was performed for all the patients enrolled in this study. EGFR TKI agents were selected primarily in EGFR positive patients.
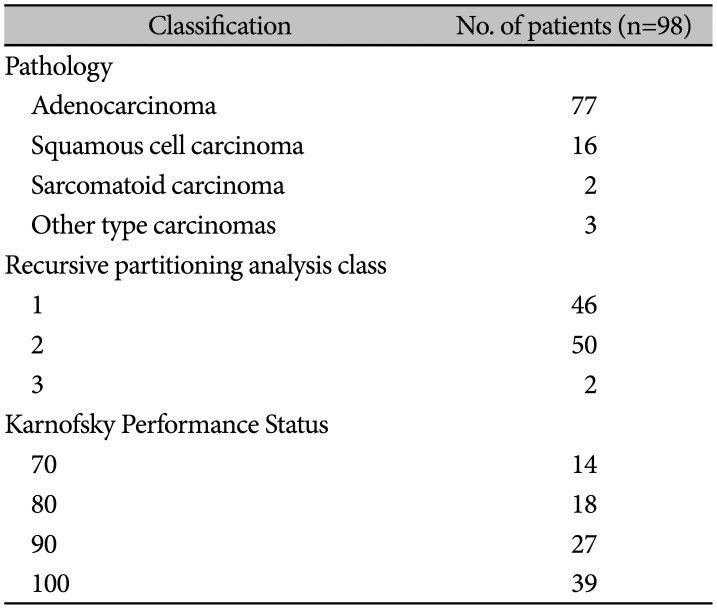
Table 2
Pathology and clinical status of the patients
![]()
Statistical analysis
All analyses were conducted using MedCalc (version 12, MedCalc Software bvba, Ostend, Belgium). Frequencies and descriptive statistics of demographic and clinical variables were obtained. OS of the patients was estimated using the Kaplan-Meier method. Progression-free survival (PFS) was defined as the time interval from the radiosurgery to documented disease progression in the intracranial disease or systemic disease. Significance was determined by a two-tailed p-value of less than 0.05.
Go to :
RESULTS
The median OS of the patients was 16 months [95% confidence interval (CI), 13–21 months]. One-, two-, and threeyear OS were 62.2%, 31.7%, and 21.0%, respectively. Median systemic disease PFS and intracranial disease PFS were 9 months (95% CI, 8–11 months) and 11 months (95% CI, 7–14 months), respectively.
The patients with EGFR mutations had longer intracranial PFS than those without EGFR mutation (median intracranial PFS: 19 vs. 10 months with p=0.01) and there were no benefits in OS and systemic PFS (Fig. 1). Additionally, the patients harboring adenocarcinoma had longer OS (p=0.01) and intracranial PFS (p=0.01) (Fig. 2), and the patients with lower recursive partitioning analysis (RPA) class had longer OS (p=0.02) and intracranial PFS (p=0.03) (Fig. 3).
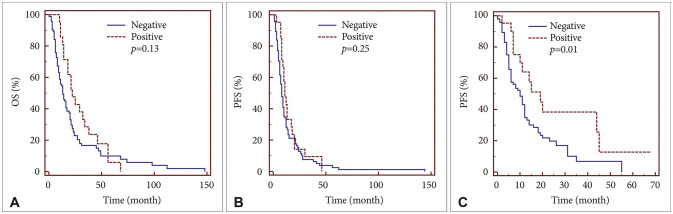 | Fig. 1Kaplan-Meier survival curve. OS (A), systemic disease PFS (B), and intracranial disease PFS (C) according to EGFR mutation are shown. Only intracranial disease PFS was statistically different. OS, overall survival; PFS, progression-free survival; EGFR, epidermal growth factor receptor.
|
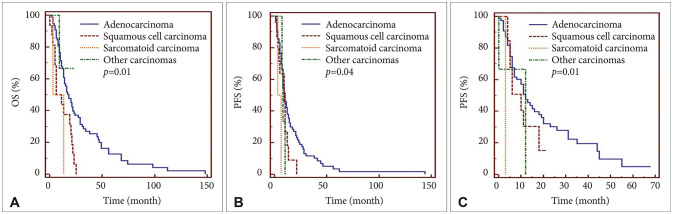 | Fig. 2Kaplan-Meier survival curve. OS (A), systemic disease PFS (B), and intracranial disease PFS (C) according to primary tumor pathology are shown. The patients with adenocarcinoma had longer overall survival, systemic disease PFS, and intracranial disease PFS over those with other pathologies. OS, overall survival; PFS, progression-free survival.
|
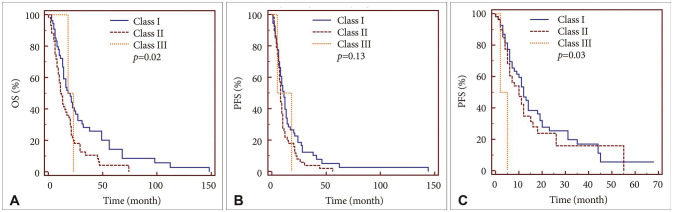 | Fig. 3Kaplan-Meier survival curve. OS (A), systemic disease PFS (B), and intracranial disease PFS (C) according to RPA class are shown. The patients classified as class I had longer OS and intracranial disease PFS over those with other classes. OS, overall survival; PFS, progression-free survival; RPA, recursive partitioning analysis.
|
Kaplan-Meier survival analysis revealed improved OS rate in younger patients (p<0.01), the patients with fewer intracranial lesions (p<0.01), and shorter time duration to brain metastasis (p<0.01) while it revealed no statistical differences in intracranial disease PFS according to those variables (Table 3). The patients with a shorter time to brain metastasis (p<0.01) or with small number of brain metastatic lesions (p<0.01) showed longer PFS in systemic disease. Other variables such as mode of brain metastasis, EGFR mutation, sex, and smoking status were not related to the OS.

Table 3
Variables related to OS, systemic PFS, and intracranial PFS
![]()
Go to :
DISCUSSION
EGFR mutation has shown to be better prognostic factor in NSCLC patients when TKI was selected as a first-line chemotherapy [12131415]. However, there has been controversy regarding EGFR mutation having an effect on the treatment results of intracranial disease in patients with brain metastasis from systemic cancer. In our study, the results showed that EGFR mutation had a positive effect on PFS of intracranial disease in the patients who underwent radiosurgery for metastatic brain lesions. Heon et al. [16] reported that brain metastatic lesion progresses differently according to EGFR mutation in the NSCLC patients treated with TKI. In the animal study, EGFR mutated brain metastasis has shown the efficacy of gefitinib [17]. Some human data have shown the effect on brain metastases when TKI was used even though EGFR mutation was not confirmed in most cases [181920]. Recent studies reported that TKI agents had a promising effect on brain metastasis from NSCLC with EGFR mutation [32122]. Radiation therapy and TKI treatment were reported even as the same efficacies in intracranial disease from NSCLC [23]. However, some authors reported that the effectiveness of EGFR-TKI is different in brain metastasis because there was a different expression of EGFR mutation between intracranial disease and systemic disease in NSCLC patients [924]. Other reports stressed additional efficacy of radiation therapy on TKI treatment from NSCLC patients with brain metastases rather than TKI treatment alone [25]. Furthermore, there was a report for which we needed to clarify the role of multimodality treatment such as cranial radiation and the optimal timing of TKI agents because resistance to these agents is common [26]. Shin et al. [27] concluded that EGFR mutations were not associated with improved intracranial disease control even though NSCLC patients with EGFR mutated brain metastasis had favorable survival.
Radiosurgery has a promising role on brain metastases from NSCLC [2829]. However, the results of radiosurgery on intracranial disease could be different according to primary cancer pathology [30]. In our study, adenocarcinoma showed the best results after radiosurgery among NSCLC pathologies. The additional effect of EGFR mutation on adenocarcinoma after radiosurgery could not be clarified in our study. There was controversy about the additional effect of EGFR TKI in the literature reviewed. Kim et al. [31] reported that radiosurgery and TKI treatment was not superior to radiosurgery alone, however, there was no additional side effect of TKI. There were a few reports on the resistance of TKI treatment in brain metastases [1132]. However, Eichler et al. [8] reported that EGFR mutation status had an association of improving survival in NSCLC patients with brain metastases. The additional effect of TKI treatment on radiotherapy was reported by Zhang, et al. [10]. Heon et al. [16] reported that the risk of central nervous system progression of advanced NSCLC patients was related to EGFR mutation status.
There are several reports about prognostic factors following radiosurgery on brain metastases from NSCLC. Na et al. [33] reported that systemic disease status, use of EGFR-TKIs, and the number of brain lesions were statistically significant predictors of early distant brain failure. Bragstad et al. [34] reported that the volume of brain metastases was a predictor for the quality of life and length of survival in patients with lung cancer. Perilesional edema in brain metastasis from NSCLC was reported as a predictor of response to radiosurgery by Tini et al. [35]. Cho et al. [28] reported that the number of the lesions and cumulative tumor volume were prognostic factors after radiosurgery in the patients with metastases from NSCLC. EGFR mutations, primary cancer pathology, and RPA class are positive prognostic factors on intracranial PFS in the study conducted by us.
In conclusion, OS of the patients with brain metastasis from lung cancer was related to EGFR mutations, primary tumor pathologies, RPA class, the patients' age, the number of brain metastasis, and the time to brain metastasis.
In this study, EGFR mutations, primary cancer pathology, and RPA class may be proposed as prognostic factors for intracranial PFS in NSCLC patients after GKRS for brain metastasis.
Go to :
 XML Download
XML Download