

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The Guideline Working Group of Korean Society for Neuro-Oncology (KSNO) continues development effort for the clinical guideline in the management of patients with brain tumor since 2017. A well-established clinical guideline helps clinician's daily practice by following current best management options, improving diagnostic accuracy, and promoting treatment efficacy. To select the topics of the urgent needs for standard of practice, it is important to grasp the diversity of current clinical practice in the point of care. Elucidating the details of the variation of management pattern among physicians may help improving medical practices by bringing to light new problems that need to be solved. This information can also be used for helping to establish national health insurance policy involved in brain tumor care in Korea. Thus, the Guideline Working Group conducted a nationwide questionnaire survey on the clinical practice of brain tumor which was comprised of 6 categories. As part I of the survey result, here we report the current status on antiepileptic drug (AED) and steroid usage in brain tumor management.
Seizures are one of the most common medical complications in brain tumor patients, which can be provoked during the perioperative period of brain tumor resection. Therefore, AEDs are frequently used for therapeutic or prophylactic purposes in brain tumor patients [1]. It is widely accepted that perioperative seizures must be controlled with AED administration, but the proper duration of AED maintenance is not established [2]. Moreover, it is still controversial to use prophylactic AED for patients undergoing brain tumor resection with no prior seizure history [3].
Steroids have long been used in the medical care of brain tumor patients for approximately 60 years, which especially help to reduce peritumoral vasogenic edema and relieve increased intracranial pressure symptoms related with brain tumor in the perioperative period [4]. In spite of various benefits, they are not without burden because of its potential to cause side effects [5]. Careful steroid usage under minimizing toxicity is important to care for brain tumor patients. However, there is a lack of standard consensus for the dose, maintenance duration with tapering schedule, and prophylaxis strategy of complications on long-term usage in steroids.
The survey result showed a wide variance of current clinical practice in brain tumors that need to be addressed for the development of guidelines in the future.
MATERIALS AND METHODS
The survey topics and questionnaire were selected and developed by the Guideline Working Group of KSNO composed of 26 multidisciplinary members including 15 neurosurgeons, 5 radiation oncologists, 1 medical oncologist, 2 neuroradiologists, 2 pathologists, and 1 neurologist. The nationwide survey was performed using Google Form, a web-based survey system and was emailed to all members of the KSNO (n=423). Respondents could complete the questionnaire online through the link that was available between 3rd and 17th November 2019, at which point the survey was closed. Participation was voluntary and not remunerated. All respondents received the same set of questions. The entire questionnaires dealt with the following management topics: 1) AED usage for brain tumor patients; 2) steroid usage for brain tumor patients; 3) management strategies of diffuse midline glioma; 4) decision of proper management of brain metastasis; 5) management strategies of meningioma; 6) management policy of primary central nervous system lymphoma (PCNSL). Respondents were also asked to indicate their specialty and number of years in practice.
The questionnaires about AED (9 questions) and steroid (5 questions) usage for patients with brain tumor was structured around existing controversies regarding real clinical management in patients (Appendix). In the relation with AED usage, survey questions focused on the usage or non-usage of AEDs in the peri/postoperative period according to whether the seizure or not, duration and tapering schedule of preventive AEDs, choice of AED, and driving a car for patient with seizure. As for the steroid usage, participants were asked about their usage or non-usage of steroid in the peri/postoperative period, factors determining steroid usage, dose and duration with tapering schedule of steroid, and preventive management of long-term steroid usage. All responses were analyzed descriptively as well as quantitatively wherever appropriate.
RESULTS
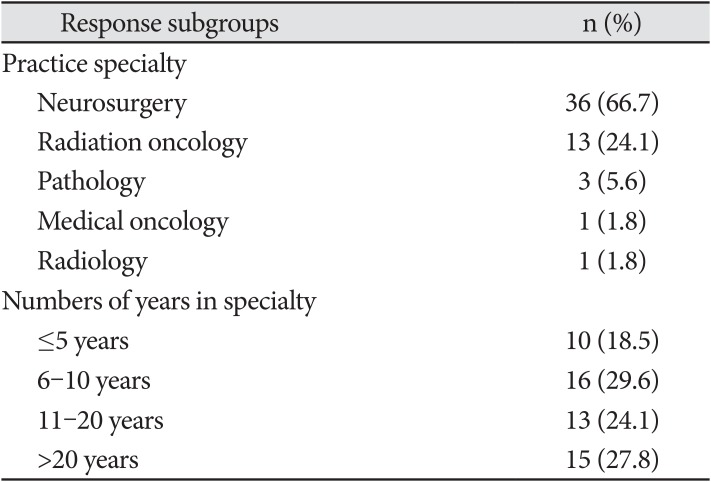
The survey was responded by 54 respondents for an overall response rate of 12.8%. Not all questions were answered by all respondents. Most respondents were neurosurgeons (n=36, 66.7%) followed radiation oncologists (n=13, 24.1%). The majority of respondents (n=44, 81.5%) had more than 5 years of experience in practice specialty. A summary of the characteristics of the respondents is shown in Table 1.
AED usage
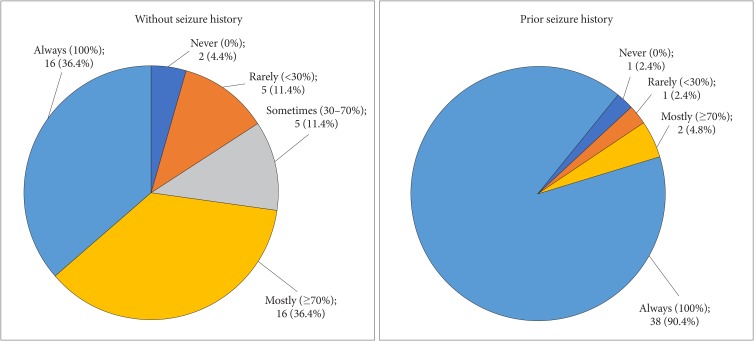
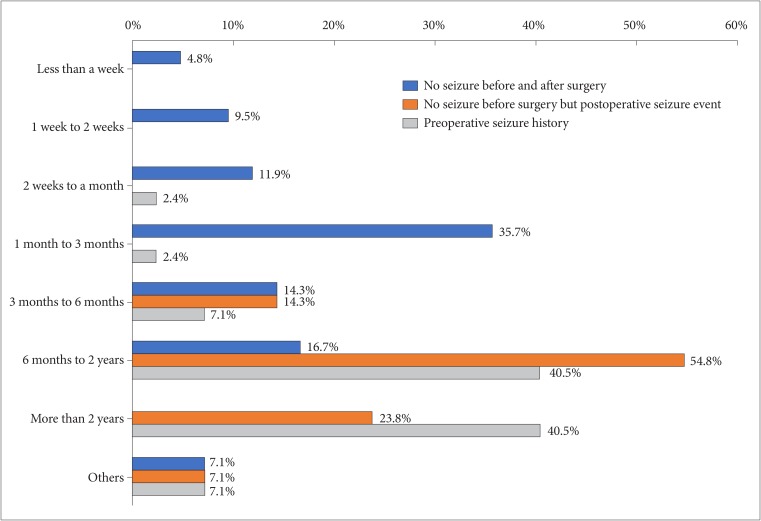
A total of 32 of 44 (72.8%) respondents routinely (always and mostly) prescribed prophylactic AEDs for seizure-naïve patient in the peri/postoperative period, and only two (4.4%) respondents never prescribed prophylactic AEDs in this setting (Fig. 1). For patients with seizure history, most respondents (95.2%) prescribed prophylactic AEDs routinely (Fig. 1). The duration of AED prophylaxis varied depending on the presence of seizure in the peri/postoperative period (Fig. 2). In seizure-naïve patients, 32 of 42 (76.2%) respondents stopped AEDs within 6 months, and no respondents used it for more than 2 years. However, if a patient experienced postoperative seizure event, the preferred duration of AED prophylaxis was long enough to reach more than 6 months in 78.6% of respondents including 23.8% offering more than 2 years. For those patients with prior history of seizure before surgery, long-term AED prophylaxis was preferred in the majority of respondents; 81.0% respondents continuous AEDs for at least 6 months, including 40.5% offering for at least 2 years from last seizure episode (2-year seizure-free interval).
Most respondents (94.9%) reported that the presence of seizure in the peri/postoperative period is the most important factor in determining the duration of prophylactic AEDs. Respondents also reported other important factors in determining it in the following order: location of brain tumor (n=31, 79.5%); extent of peritumoral edema (n=19, 48.7%); abnormality of electroencephalography (n=18, 46.2%); type of brain tumor (n=17, 43.6%); presence of residual tumor (n=12, 30.8%); extent of postoperative hemorrhages in surgical field or intraoperative bleeding (n=10, 25.6%); usage of AED combination therapy (n=10, 25.6%).
Levetiracetam is the most preferred AED, with 34 of 41 (82.9%) respondents considering it as a first-line prophylactic agent followed by phenytoin (n=2, 4.8%) and topiramate (n=2, 4.8%) with the remaining 7.5% (n=3) comprising of other drugs such as valproate, lacosamide, carbamazepine, oxcarbazepine, and zonisamide. The medical status of each patient (n=24, 61.5%), such as liver and renal function, emerged as the most important factor in choosing the AED followed by drug interaction with anticancer drug (n=12, 30.8%). Ten (25.6%) respondents reported that there were no factors to consider it, and one (2.6%) respondent considered the type of brain tumor.
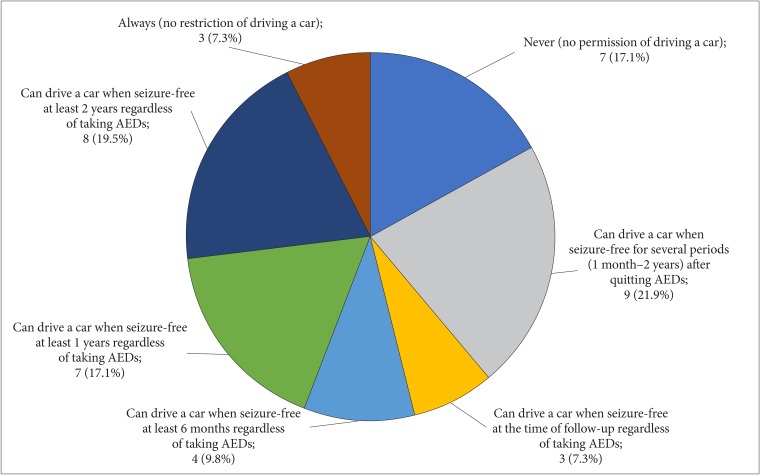
It is a difficult judgement to recommend a patient who is taking AED to drive a car. There was a great diversity of opinion about allowing patients to drive a car and about its conditions (Fig. 3).
Steroid usage
As many as 90.5% of respondents use steroids in perioperative period for brain tumor patients, including 34.2% of them as a routine manner. However, 25 (65.8%) respondents prescribed steroids for specific situations. They considered following factors determining usage or non-usage of steroid in the peri/postoperative period: presence of peritumoral edema (90.9%), degree of clinical symptoms (60.6%), type (e.g., extraaxial or intraaxial tumor) of brain tumor (51.5%), location and size of brain tumor (39.4%), presence of underlying diseases (e.g., hypertension, diabetes, osteoporosis and immunosuppressive state) of patients (33.3%), and type (e.g., fluorescence guided surgery or awake surgery) of surgery (15.2%).
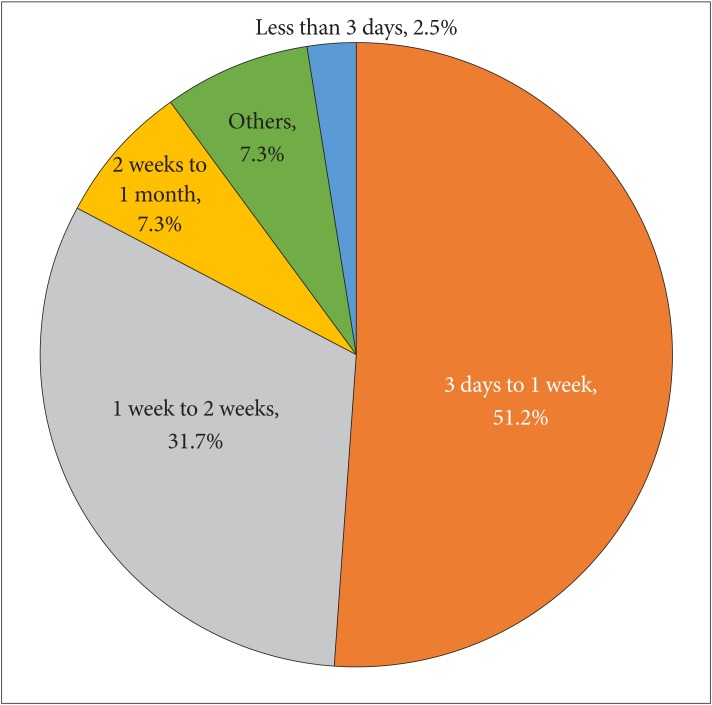
The result of the questionnaires on the dosage and duration of steroid usage showed no significant differences among the respondents. Among 39 respondents, 10 (25.6%) respondents used 12–16 mg steroid of maximum dose per day, and 25 (64.1%) respondents answered higher than 16 mg steroid of maximum dose per day. For duration including tapering schemes of steroid, 85.4% of respondents discontinue the steroid within 2 weeks after surgery, and no respondents used it for more than 1 month (Fig. 4). For the prophylactic care for complications of steroid usage, such as osteoporosis and pneumocystis pneumonia, only 12 of 42 (28.6%) respondents always performed preventive management during long-term steroid usage.
DISCUSSION
Although KSNO members frequently administer prophylactic AED to patients with brain tumor, there is limited evidence on the efficacy of prophylactic AED to prevent first seizures. The American Academy of Neurology recommends not to use prophylactic AED routinely in seizure-free brain tumor patients [6]. Following studies and meta-analyses have confirmed these recommendations [78910]. When prophylactic AEDs were administered, it is suggested that they be tapered off in the first week after surgery [6]. Meanwhile, chronic AED administration can be justified in patients who have experienced seizure before and after brain tumor resection. After gaining seizure freedom in brain tumor patients, withdrawal of AEDs can be attempted following the general recommendation of the general epilepsy population [11]. However, no studies have systematically investigated the proper strategy for AED withdrawal in brain tumor patients.
There are several considerations in choosing AED for brain tumor patients. First, the possibility of cytochrome P450 drug interaction should be considered for brain tumor patients who will need to use many chemotherapeutic agents [12]. For example, if irinotecan is applied with concurrent enzyme-inducing AEDs, its clearance rises and the maximum tolerated dose will become 3.5 times higher [13]. Therefore, newer generation AEDs without enzyme-inducing properties, such as levetiracetam, zonisamide, pregabalin and lacosamide, should be preferred [11]. Second, certain AEDs should be given with the consideration of its adverse effects. Many AEDs may cause rash or cytopenia, topiramate may cause cognitive dysfunction, and topiramate or zonisamide may cause weight loss which are important issues in the management of brain tumor patients [14]. Lastly, anti-tumor effects of certain AEDs, such as valproate [15], levetiracetam [16], and perampanel [17], have been suggested based on the experimental data but further evidence is required.
Steroid usage for brain tumor patients with clinical symptoms related with mass effect and peritumoral edema is generally recommended [18], but there is little evidence of steroid usage for brain tumor patients without them. The response of KSNO members about steroid usage in the peri/postoperative period reflects the general principle. Recently, the American Society of Clinical Oncology (ASCO) and the Society for Neuro-Oncology (SNO) endorsed the guidelines of the Congress of Neurological Surgeons (CNS) for steroid usage in metastatic brain tumors [19]. In their recommendations, corticosteroids are recommended to provide temporary symptomatic relief for only patients with symptoms as Level 3 evidence.
Dexamethasone is the most commonly used steroid in the neuro-oncology field, because of the least amount of mineralocorticoid activity of all the corticosteroids. The optimal protocol of dexamethasone for brain tumor patients in the peri/postoperative period has not been clearly evaluated. In the relation with starting maximum dose per a day, a dexamethasone dose of 16 mg/day has been universally accepted for management of brain tumor patients, since a dose-response curve was firstly constructed in the report of pre-operative dexamethasone usage in brain tumor patients [4]. However, one randomized controlled trial of dexamethasone starting doses in metastatic brain tumors for pre-radiotherapy demonstrated that each starting dose of 4, 8, or 16 mg/day achieved the same improvement in Karnofsky performance status after 1 week of corticosteroid therapy, and side effects were significantly more frequent in group prescribed with 16 mg/day [20]. Besides, it remains doubtful whether dose higher than 16 mg dexamethasone per a day provides additional benefits [21]. In the relation with duration including tapering-schedule of steroid, there is general consensus in the literature that significant adrenal suppression may occur after 2 weeks of corticosteroid usage [22]. Therefore, it is generally recommended that steroids can be stopped quickly after using for a short period of no longer than 10–14 days, and tapering needs to be more cautious after 10 days of administration to promote adrenal recovery. In the guideline of the CNS endorsed by the ASCO and SNO, the maximum dose per a day of 4 to 16 mg/day are recommended according to the severity of symptoms related with mass effect and peritumoral edema, and tapering is recommended as rapidly as possible in clinically tolerable degree [19]. It is necessary to use steroids to adjust for each brain tumor patient. The prophylactic care for complications of long-term steroid usage should be considered for patients receiving steroids for more than 1 month and undergoing chemotherapy or radiotherapy [2324].
As with any online survey, the major limitation of this study is response bias that respondents might be influenced by the pressure to follow the related guidelines. Additionally, the relatively low response rate may give rise to sampling bias interfering with the valuable interpretation of several questions, such as about permitting driving a car for patients with seizure and about management for preventing the complication of long-term steroid usage.
In conclusion, the survey demonstrates the variation and similarity of clinical practice about AED and steroid usage for patients with brain tumor among members of the KSNO. It is important to reduce the variation for establishing the guideline based on the best available evidence.
 XML Download
XML Download