

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rathke’s cleft cysts (RCCs) are benign tumors of the pituitary gland [1] primarily of the sellar region and less frequently of the suprasellar region [2]. RCCs, which are usually asymptomatic, are most commonly discovered incidentally [34]. Small, asymptomatic RCCs do not require surgical treatment [5].
On the other hand, for symptomatic RCCs [6], surgical treatment is required [3] using a transsphenoidal approach in most cases [7]. The goal of surgical treatment is to safely drain the contents of the cyst and to remove as much of the capsule as possible [5]. Cyst contents vary; either thick, mucous or clear, serous [1].
Currently, CT and MRI are the most popular imaging techniques for RCCs [3]. On CT, they usually appear to have low to slight high density compared to brain parenchyma [8]. On MRI, they generally appear as well-separated cystic mass with a homogeneous intensity signal that is sometimes combined with thin cyst wall enhancement [9]. An MRI signal can be hypo-, iso-, or hyper-intense, depending on the contents of the cyst [10].
The natural history of RCCs is greatly vary and has not been clearly demonstrated [3]. Therefore, we sought to identify factors capable of predicting the prognosis of RCCs. We analyzed the MRI signals in patients diagnosed with an RCC who were either undergoing follow-up or had undergone surgical treatment.
MATERIALS AND METHODS
Patients
We retrospectively reviewed medical records of patients with an RCC who were diagnosed and managed in our institution between April 2004 and April 2020 and generated two different cohorts: an observation group and a surgical group. Patients who had undergone another brain surgery or had been diagnosed with another brain disorder were excluded. Patients evaluated by MRI with insufficient resolution were also excluded as their MRI signals had not been reliably characterized. For the same reason, patients with an RCC smaller than 3 mm were also excluded.
Patients were included in the observation group if they were evaluated and followed up using at least three MRI scans for at least 5 years. A total of 114 patients were included in the observation group, and their MRI signal characteristics were evaluated at both the time of initial diagnosis and during follow-up. We also identified and recruited 99 patients who had undergone surgical treatment for their RCCs for the surgical group. The indications for surgery included visual deterioration, endocrine hormone deficiency, and intractable headache. All RCCs were operated via transsphenoidal approach either microscopically or endoscopically. The preoperative MRI signal characteristics of these patients were also analyzed, and visual and endocrine outcomes were evaluated. This study was conducted in accordance with the Declaration of Helsinki and approved by the Severance Hospital Institutional Review Board (4-2022-1018). The authors have no potential conflict of interest to disclose.
Radiological evaluation
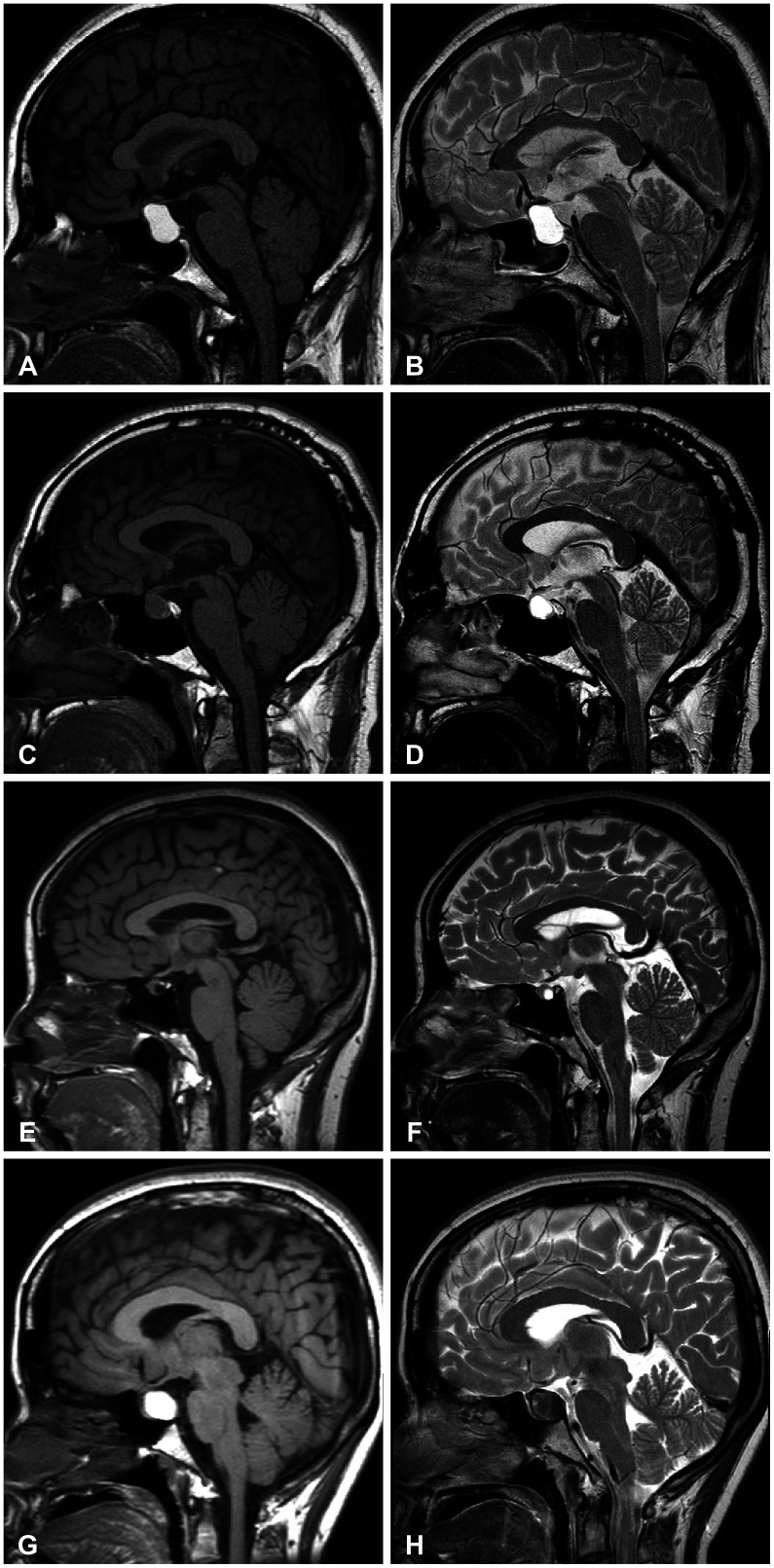
All of the patients were evaluated using dynamic MRI of the sellar region with a 1.5-T (Signa; GE Health Care, Minneapolis, MN, USA) or 3.0-T system (Achieva; Philips, Best, the Netherlands). The MRI evaluation included spin-echo T1-weighted (T1W; repetition time [TR] 500 ms/echo time [TE] 20 ms), T2-weighted (T2W; TR 3,500 ms/TE 100 ms), and dynamic contrast-enhanced (TR 400 ms/TE 10 ms) imaging after the intravenous administration of gadolinium-diethylenetriamine pentaacetic acid (0.1 mL/kg body weight) at a temporal resolution of 25 s.
MRI signals of the cyst were described as hypointense, isointense, or hyperintense and compared with the signal intensity of brain white matter [11]. Changes in cyst size were considered significant only when greater than 1 mm.
Endocrine evaluation
For patients in the surgical group, their endocrine function was evaluated using the combined pituitary function test (CPFT) both preoperatively and postoperatively, as described previously [12]. The CPFT was performed by injecting intravenous insulin (0.1 U/kg), thyrotropin-releasing hormone (TRH, 500 µg), and gonadotropin-releasing hormone (GnRH, 100 µg). Hypoglycemia was defined as a serum glucose level less than 40 mg/dL in a patient without diabetes or less than 50% of the basal level in a patient with diabetes. Serum levels of growth hormone, cortisol, adrenocorticotropic hormone, luteinizing hormone (LH), follicle-stimulating hormone (FSH), thyroid-stimulating hormone (TSH), and prolactin (PRL) were measured during 2 hours. Lactotropic deficiency was diagnosed when the basal serum PRL level was less than 2 ng/mL and failed to increase to twice the initial level. Thyrotropic deficiency was diagnosed when a subnormal serum free T4 level (<0.73 ng/dL) was associated with a low or normal TSH level and failed to increase to a peak value greater than 5 mIU/mL from the basal level after the administration of TRH. Corticotroph deficiency was diagnosed when the cortisol level failed to increase by 70 ng/mL or above a peak value of 180 ng/mL. Gonadotropin deficiency was evaluated based on the GnRH test when LH and FSH failed to increase to peak values greater than 10 mIU/mL and 2 mIU/mL from their basal levels, respectively. Gonadotropin deficiency was diagnosed in male patients when the serum level of testosterone was low (<10 nM) in the presence of low or normal levels of gonadotropins (>10 mIU/mL). In premenopausal women, gonadotropin deficiency was diagnosed in the presence of amenorrhea or oligomenorrhea and infertility when gonadotropins were low or below normal in the setting of low estradiol levels (<123 pM). In postmenopausal women, gonadotropin deficiency was considered when the LH and/or FSH levels were inappropriately low for the women’s age (<20 mIU/mL).
Ophthalmological evaluation
Standard automated perimetry using a Humphrey visual field analyzer (Carl Zeiss Meditec Inc., Jena, Germany) was performed when optic nerve compression was evident on MRI. Both the visual field index and mean deviation were taken as visual field parameters. For the surgical group, postoperative evaluations were performed for surgical outcome measurements [13].
Statistics
Differences in basic characteristics of the patients, including age and tumor size, were analyzed using the Student’s t-test, and differences in gender between the observation and surgical groups were analyzed using the chi-square test.
To demonstrate a significant difference in size or surgical status, all MRI signals were divided into two groups and analyzed using the chi-square test. Statistics were derived by dividing one group, for example, a T1 or T2 sequence, by the remaining eight groups. Statistical analyses were performed using IBM SPSS Statistics (v. 23.0; IBM Corp., Armonk, NY, USA), and a p<0.05 was considered statistically significant.
RESULTS
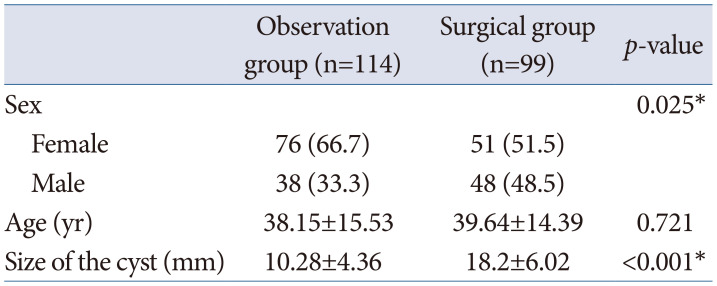
A total of 213 patients (99 patients in the surgical group and 114 patients in the observation group) were recruited for this study, and their medical records were retrospectively analyzed. The basic characteristics of patients in the two groups are summarized in Table 1. The mean age was not statistically different between the two groups: 38.15±15.53 years in the observation group and 39.64±14.39 years in the surgical group, with a p-value of 0.721. In the comparison between two groups, the observation group showed female predominance which was not apparent in the surgical group (p=0.025). Cyst size was larger in the surgical group compared to that in the observation group (18.2±6.0 mm vs. 10.3±4.4 mm, respectively, p<0.001). The most common indication of surgical intervention was visual deterioration caused by optic nerve compression, which was followed by endocrine dysfunction.
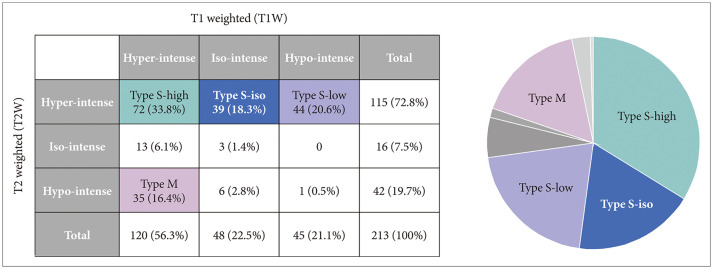
The characterization of MRI signals of cyst contents in both T1W and T2W images revealed nine combinations for our 213 patients (Fig. 1). T2W images showed hyperintensity in the majority of cases (115, 72.8%). Among those with a high T2W signal, the cysts showed hypo-, iso-, and hyper-intensity on T1W images in 44, 39, and 72 patients, respectively. In most of these patients, the cystic contents were found to be serous; therefore, we categorized these three groups as Type S-low, Type S-iso, and Type S-high. For the rest of the combinations, we identified another group of 35 patients whose cysts showed hyperintensity on the T1W images and hypointensity on the T2W images. In most of these patients, the cystic contents were quite mucous; therefore, we named this group Type M. We thus identified four major groups for 89.2% of our patients: Type S-low (20.6%), Type S-iso (18.3%), Type S-high (33.8%), and Type M (16.4%) (Fig. 2).
Comparison between observation and surgical groups
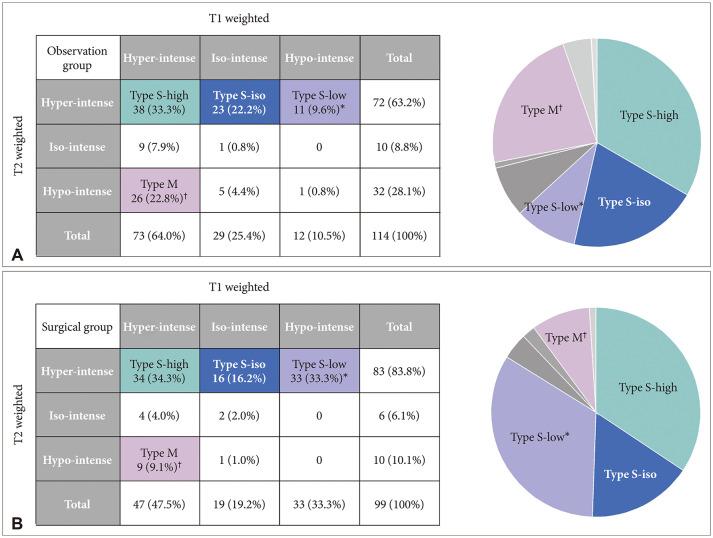
In the comparison between observation and surgical groups, we identified only two major groups in which the number of patients in the surgical and observation groups was statistically different: Type S-low and Type M (Fig. 3). In the Type S-low group, 33 patients (33.3%) underwent surgical treatment, whereas only 11 patients (9.6%) were observed only (p<0.001). However, patients in the Type M group less frequently required surgical treatment: Only 9 patients (9.1%) underwent surgery, whereas 26 patients (22.8%) were simply observed without intervention (p=0.007). In the other two major groups, the number of patients in the surgical and observation groups was not different: Type S-iso (p=0.450) and Type S-high (p=0.876).
Natural course of RCCs in the observation group
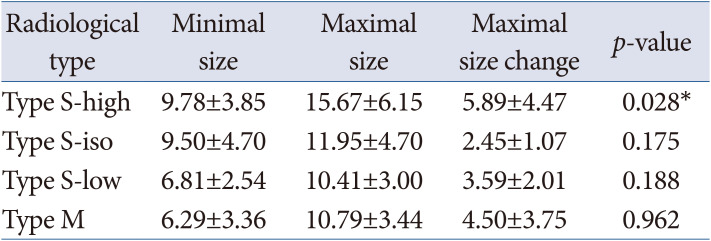
RCCs were monitored without surgical intervention in 114 patients. The average RCC size at the time of diagnosis was 10.28±4.36 mm. In most cases, the size of the cysts continued to change throughout the follow-up period (93.7±27.8 months). The maximal range of fluctuation (MRF) in size was defined as the difference between the minimal and maximal sizes for each case. The MRF was 4.61±3.45 mm in the observation group. Their natural course was stable in most cases as the MRF was less than 5 mm in the majority of patients (94 patients, 82.5%). Only in eight patients (7.0%) did the MRF exceed 10 mm during the follow-up period. In the comparison among the four major radiological types (Table 2), the MRF was higher in the Type S-high group than in the other groups (p=0.028).
Visual and endocrine outcomes in the surgical group
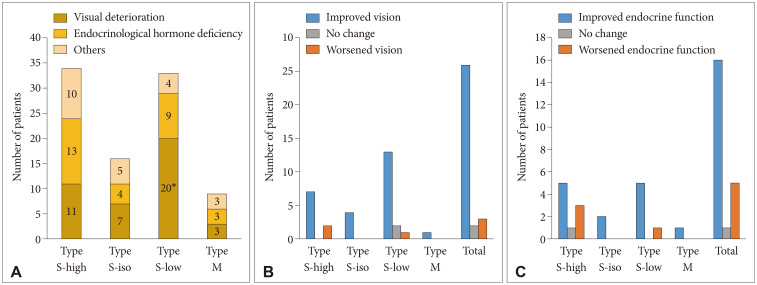
In the surgical group, the main indications of surgery were visual deterioration in 41 patients, endocrine hormone deficiency in 29 patients, and other reasons such as uncontrolled headache in 22 patients. When focusing on the four major radiological types, the Type S-low group included more patients who underwent surgery for the relief of visual symptoms compared with other groups (p=0.034) (Fig. 4). Among 43 patients whose main surgical indication was a visual disturbance, postoperative visual outcome measurements were available in 31 patients. Visual improvement was achieved in 26 patients (83.9%), whereas visual function did not change in 2 patients and worsened in 3 patients. As for endocrine dysfunction as a surgical indication, 33 patients underwent surgery to improve their endocrine function. Among these patients, results of both preoperative and postoperative CPFTs were available in only 22 patients. Endocrine function was improved in 16 patients (72.8%), worsened in 5 patients (22.7%), and did not change in 1 patient after surgery. The intergroup differences in visual and endocrine outcomes were not evident.
DISCUSSION
RCC is a relatively common pathology of the pituitary gland and its clinical course is mostly very indolent [3]. The size of RCC may change during follow-up and many studies reported even spontaneous involution of the cyst [1415]. However, it is also very obvious that many of RCC patients also require surgical treatment with various indications. Surgical strategies, technique and its outcome in the surgical treatment of RCC is very different from those for pituitary neoplasms [16]. Especially, its endocrine outcome is less favorable than in surgical treatment for pituitary adenomas [17]. Furthermore, recurrence after surgery is not uncommon as 12.5% of surgically treated RCCs are reported to experience recurrence after successful surgical decompression [1617]. As considering the indolent and versatile natural course of RCCs, long-term follow-up is essential. In this context, prediction of their natural course would be beneficial in long-term management.
There have been many efforts to categorize the types of RCCs in the past. Hama et al. [18] classified RCCs histologically as having single or stratified epithelial cells of which classification scheme does not convey clinically usefulness for the patient management. On the contrary, Potts et al. [19] classified RCCs according to their location: Pure sellar was Type 1, sellar and suprasellar were Type 2, and pure suprasellar was Type 3. Cyst location is often critical as it determines the nature of symptoms and surgical approaches when it is necessary. Ozoner et al. [20] divided RCCs into three types according to the MRI signals determined by the cystic contents and fluidity of the cysts. Patients with Type A RCCs had T1W-low and T2W-high signals, patients with Type B RCCs had T1W-iso-high and T2W-low signals, and patients with Type C RCCs showed T1W-low and T2W-low signals. Type A RCCs were defined as Type S-low in our cohort, and patients with Type B RCCs appeared most similar to patients in the Type M group. Patients with Type C RCCs only made up 0.5% of our patients. Whereas the Type B group was the most common in their study, the Type M group in our study comprised only 16.4% of all patients. The T1W and T2W signals on MRI for RCCs are diverse [10]. Kim et al. [7] examined the MRI findings of RCCs and found that T1W-high and T2W-high signals were the most common accounting for 26% of their patients [21], which was also supported by Wen et al. [2].
In our cohorts, more female patients were included in the observation group, similar to the results of our study [2223] whereas the number of female and male patients were similar in the surgical group. When the surgical and observation groups were compared, the group that was more statistically likely to undergo surgery was the Type S-low group. In these patients, the cystic content was found mostly serous. Ozoner et al. [20] found that, similar to our study, that patients with Type A RCCs, a group similar to patients in our Type S-low group, received more surgical treatment than other patients with other MRI signals. Therefore, in a patient with a Type S-low RCC, careful follow-up should be made for possible surgical treatment. On the contrary, patients with Type M RCCs were less prone to surgical treatment.
In the observation group, the RCCs showed decrease or increase in the size during follow up. The range of change in the RCC size were about the similar except for Type S-high RCCs. Thus, for patient with Type S-high RCCs, the cysts may change in their size drastically, which implies surgeons should be more careful in surgical decision and more frequent MRI follow up is necessary.
One of the major limitations of this study is that we simply combined two different cohorts for comparative analysis, which may have yielded a bias, inborn nature of the retrospective study. Also, since the radiological type was determined only by the first MRI scan, it did not consider RCCs whose type changed later. Additional studies taking these limitations into account are therefore needed.
 XML Download
XML Download