

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Brain metastasis (BM) is the most common type of brain tumor in adults. It occurs approximately 10 times more frequently than a primary malignant brain tumor [1]. Population-based studies estimate that 8%–10% of cancer patients develop BM [2]. Lung cancer and breast cancer are the most common primary origin of systemic cancer [34]. As cancer treatment, diagnosis, and surveillance improve, the incidence rates of BM continue to increase. However, the prognosis for BM remains poor, and less than 50% of patients die within 24 months [5].
With the advancement of stereotactic radiosurgery (SRS), it has been widely used to treat small-to-medium-sized metastatic tumors. SRS has a local control rate comparable to surgery [6]. Additionally, minimal invasiveness and a low rate of acute neurological complications are important advantages of SRS [78].
The management of BM remains complex and should be performed after multidisciplinary discussions with neurosurgeons, oncologists, and radiation oncologists. The development of new chemotherapeutic drugs, evolving radiation therapy and SRS techniques, and treatment options for BM are varied. However, surgery remains a unique and essential tool for the treatment of BM [910]. In the SRS era, the role of surgery in the treatment of BMs needs to be refined, and efforts to overcome the drawbacks of surgery are necessary. This review covers the refinement role of surgery for BM and recent innovations in intraoperative considerations.
Go to : 
PREOPERATIVE CONSIDERATION
The preoperative workup of lesions suggestive of BM centers on neuroimaging. CT rules out neurosurgical emergencies and allows superior visualization of bony details, including bony involvement. CT angiography shows the arterial and venous relationships of the tumor, and a detailed evaluation of the adjacent arteries and draining veins may help avoid postoperative complications. Contrast-enhanced MRI offers superior sensitivity to detect metastases, especially when the lesions are small. Other MRI modalities, such as diffusion-weighted imaging, perfusion imaging, susceptibility-weighted imaging, and spectroscopy, can help differentiate metastasis from other malignant tumors and inflammatory and infectious conditions [1112]. In addition, advanced MR imaging modalities may help evaluate posttreatment changes or responses to adjuvant radiation or chemotherapy [1113].
For lesions located in eloquent areas of the brain, functional brain MRI and diffusion tensor imaging help establish a surgical strategy [14].
The general medical condition and performance status of the patient are important to evaluate the prognosis of BM treatment. Expected life expectancy is important factors for decision of surgical resection. Although there is no consensus, in our institution, we have decided surgery when life expectancy expect over 3–6 months.
Disease-specific graded prognostic assessment (DS-GPA) has been widely used to assess prognosis and survival in patients with BM. The DS-GPA score provides a more accurate prediction of prognosis based on the primary origin of the cancer than the original graded prognostic assessment; age, Karnofsky performance status, extracranial metastasis, number of BM, and genetic alterations of each cancer are included in the DS-GPA score [15]. Summary of preoperative work up is presented in Table 1.
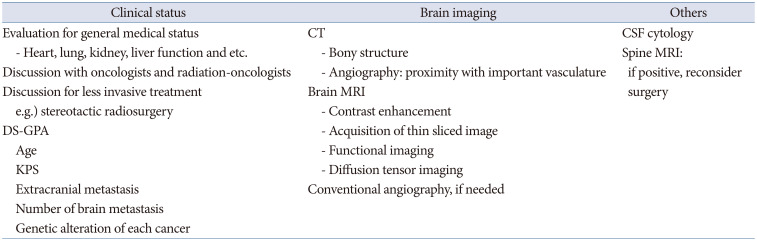
Table 1
Summary of preoperative work-up for brain metastasis
![]()
Go to :
INDICATION OF SURGICAL RESECTION IN BM
Surgical resection is still important treatment of BM. However, decision of surgery should be made considering various factors including patient general condition, alternative noninvasive treatment, and patient preference. Surgical resection is not superior treatment compared to other treatment modalities. The traditional roles of surgery are limited to large mass removal, rapid relief of neurological symptoms, and obtaining tissue for histopathological examination [1016]. However, the treatment option for BM has been varied, and with increasing numbers of treatments by SRS, the role of surgery should be revisited.
Large-mass removal
Fractionated SRS and hypofractionated radiotherapy have shown favorable efficacy for medium-to-large-sized BMs [1718]. However, surgery is undoubtedly the most important treatment for large BM. Surgery can relieve high intracranial pressure and establish coincidental tissue diagnosis. Surgery is the only treatment for emergent situations, such as intracranial hypertension due to large tumors, acute expansion of tumor cysts, or hemorrhage from metastatic tumors [19].
Rapid relief of neurological symptoms
Neurological deficits in the BM can be relieved by surgical removal of the BM. BM usually accompanies a large extent of peritumoral edema, in which both BM and peritumoral edema can lead to neurological deficits [20]. Ambulatory function is the most important function in cancer patients because it is directly related to performance status [21]. SRS can be an option for small-to-medium-sized tumors; however, in case of motor weakness due to peritumoral edema, surgery can relieve peritumoral edema faster than SRS [2022]. From the study by Rahman et al. [23], a mean period of 4.8 months is needed for a 50% volume reduction after SRS for BM. During this latent period, the patient needs long-term steroid usage; sometimes, patients show neurological deterioration. Furthermore, patients may miss the appropriate treatment time for primary origin cancer, which may adversely affect the overall survival of patients with BM. In selected cases, surgical resection of the BM can relieve peritumoral edema more rapidly than SRS or radiation.
Obtaining tissue for histopathological examination
Obtaining tissue through brain biopsy is required for BM from an unknown origin cancer (MUO) patient [2425]. High-grade gliomas can mimic metastatic brain tumors. However, the treatment of glial neoplasms differs from that of metastatic brain tumors; thus, the histopathological diagnosis is essential in cases of BM of unknown origin. Furthermore, SRS carries the risk of radiological misdiagnosis in MUO cases. Surgical resection may be used to diagnose metastatic brain tumors and cancers of primary origin. In addition, patients with only brain recurrence without extracranial disease require brain tumor tissue biopsy for histopathological and genetic tests for systemic treatment.
In some cases, systemic cancer is diagnosed through a brain tumor workup. Primary cancer biopsy, such as lung and breast masses with SRS for BM, is a good option; however, in cases of large BM, simultaneous removal of BM and histopathologic diagnosis through BM may be an alternative for simultaneous treatment and diagnosis.
Treatment of multiple metastatic tumors
Treatment of multiple metastatic tumors is still complicated; whole brain irradiation (WBRT) and SRS may be first considered to treat multiple BM [262728]. Previously, WBRT had been first chosen for multiple metastases; however, WBRT harbors the risk of leukoencephalopathy, which is a cause of severe memory and cognitive impairment [282930]. Numerous studies have shown the efficacy and favorable outcomes of SRS for brain multiple BM, and SRS has been widely accepted as a treatment modality for two to four BM [82627]. However, recently, it has been reported that SRS can be chosen for two to 10 BM and more than 10 BM lesions [27].
In the case of multiple BM that harbors a large mass and is accompanied by other small- or medium-sized tumors, SRS or WBRT alone may be ineffective; it is difficult to decrease the mass effect of large tumors and harbor the risk of adverse radiation effect (ARE) with radiotherapy [831]. Removal of the largest mass combined with additional SRS or WBRT for other lesions may help prolong overall survival and improve quality of life in selected patients [3233]. Resection of multiple large BM tumors located on the same side and same lobe using a single craniotomy may be a good option for patients who show a good performance status or need histological examination [33]. However, surgical treatment may not be recommended for multiple BM combined with leptomeningeal disease or patients with poor performance status. Case-by-case decisions regarding treatment are essential after multidisciplinary discussions.
Rescue surgery for failure of radiosurgery and radiation therapy
Recurrent tumors can be considered salvage options after SRS or radiation therapy, re-irradiation, or surgical resection [343536]. In previous studies, re-irradiation for recurrent BM showed a 2-year local control rate of more than 70% [353637]. Although considering the short survival of patients with BM, long-term ARE may not be a significant problem. However, irradiation carries the risk of ARE, including medically intractable radiation necrosis [2636].
Surgical resection can achieve oncological control and removal of radiation-affected tissue through mass removal during recurrence [34]. When recurrent tumors are located in non-eloquent areas of the brain, surgical resection is a better option than re-irradiation. In high-dose conventional skull base radiation, osteonecrosis, radiation-induced osteomyelitis, or arterial stenosis can be problematic [383940]. In this case, rescue surgery, including surgical debridement and vascularized reconstruction, is needed to manage radiation necrosis of the skull base [40]. Differentiation between radiation necrosis and the recurrent tumor is needed before rescue or surgery after radiotherapy. Positron emission tomography and perfusion MR are helpful for the differential diagnosis between recurrence and radiation necrosis [11].
Skull bone involving metastasis
The cranium is the site of blood-borne metastasis from lung, breast, thyroid, and renal cell carcinoma [414243]. Skull metastasis is classified into cranial vault and skull base metastasis [43]. Clinical syndromes, including orbital syndrome, parasellar syndrome, middle fossa syndrome, jugular foramen syndrome, and occipital condyle, are caused by skull base metastasis [44]. Most skull base metastases are unresectable; therefore, radiation therapy may be chosen as the first choice of local treatment [45]. SRS is a good option for localized small skull bone metastasis, and miliary small bony involvement can be treated with radiation therapy or chemotherapy [4145].
However, surgical resection may be preferred in cases of intracranial cranial vault metastasis involving the dura or brain parenchyma to achieve local control and relieve symptoms [42]. In addition, surgical decompression or resection is first considered for skull metastasis, inducing local pain, exophthalmos, and protrusion of the scalp.
Go to :
SURGICAL STRATEGY
Surgery plays an important role in the treatment of BM. However, surgical resection of the BM carries the risk of intraoperative tumor cell dissemination and the inherent difficulty of microscopic total resection. Neurosurgeons should attempt to minimize tumor cell dissemination and improve local control.
Improving local control
The extent of resection is an important factor in the local recurrence of BM. Total resection showed better outcomes than subtotal resection [46]. Furthermore, Yoo et al. [47] reported that microscopic total resection, including “5 mm further resection margin of the tumor,” showed a better local control rate and prolonged overall survival than gross total resection in BM surgery. Therefore, total resection plus obtaining a safe resection margin may yield the best outcome in BM surgery. However, care should be taken to minimize postoperative neurological deterioration.
The surgical methodology is also important in BM surgery. En-bloc resection of the tumor showed better local control than piecemeal tumor resection [48], and necessarily accompanied the small thickness of the adjacent normal brain resection. En-bloc resection is also known to prevent intraoperative tumor spreading compared to piecemeal resection [49]. Moreover, Patel et al. [50] reported that en-bloc resection was not associated with a high rate of complications or poor functional outcomes. In addition, according to the study by Suki et al. [4951], en-bloc resection can reduce intraoperative tumor spread. However, en-bloc resection is not always feasible, especially in large tumors or cystic tumors. Caution should be taken to minimize intraoperative spillage of internal content and spread of tumor pieces. In addition, a careful examination of the cavity after mass removal is needed to achieve total resection after piecemeal tumor resection.
Go to :
REDUCING TUMOR SPREADING AND LEPTOMENINGEAL DISEASE
The spread of tumor cells is an important issue during BM surgery. In a previous study, proximity to the cerebrospinal fluid pathway and piecemeal resection were risk factors for leptomeningeal dissemination (LMS) [1]. Breast cancer histology, younger age, larger tumor volume, and posterior fossa location are known risk factors for LMS [525354]. In a recent meta-analysis, breast cancer primary and multiple BM tumors were meaningful factors for a high risk of LMS [53]. However, there is still debate regarding the risk factors for postoperative LMS.
WBRT has been known to reduce the incidence of LMS after BM surgery [5255]; however, Ahn et al. [1] reported that WBRT did not show efficacy in reducing LMS. It is still debated that minimizing contact of the tumor with the cerebrospinal fluid space, preventing spillage of tumor content, and reducing intraoperative saline irrigation during tumor resection may help to minimize tumor spread during neurosurgical procedures. Shunt surgery may be helpful to improve quality of life in leptomeningeal disease patients.
Go to :
POSTOPERATIVE COMPLICATIONS
Postoperative complications are an important issue in BM surgery. The development of postoperative neurological deficits is a devastating factor for overall survival and significantly impacts the quality of life of patients with malignant brain tumors [56]. Cancer patients are more vulnerable to medical or surgical complications than the general population. Venous thromboembolism and pneumonia are the most important medical complications [10]. Compression stockings or pneumatic compressors for the lower leg help reduce deep vein thrombosis during the immobilization period. Encouraging sputum expectoration and deep breathing in the immediate postoperative period are required. A detailed evaluation of the patient’s medical condition is needed before surgery.
Postoperative hemorrhage and infarction are the most significant surgical complications after brain tumor surgery [57]. These complications are directly related to the performance status of the patients. Respecting arteries and veins during tumor resection are important to reduce complications. The subpial resection technique helps preserve important vascular and neural structures [58]. Preserving the major arteries is crucial during surgery, and meticulous skeletonization of arteries from the tumor is needed. In addition, preservation of the cortical or deep vein is essential to avoid venous infarction or postoperative swelling [59]. Surgery through multiple cortical openings that preserve the cortical veins and leave a small residual portion of the tumor around the vein could be an alternative surgical strategy. The prolonged use of prophylactic antibiotics did not help reduce surgical site infections [60].
Go to :
ADJUVANT TREATMENT
Surgery plus radiation therapy, including resection cavity irradiation or WBRT, showed better local control than surgery alone [2961]. Adjuvant resection cavity SRS and WBRT showed comparable efficacy for local recurrence; however, the resection cavity SRS showed superiority for neurotoxicity, including cognitive impairment and AREs, compared to WBRT [6162]. However, postoperative resection cavity SRS has difficulty in identifying the appropriate target. A large surgical cavity after resection and an appropriate radiation dose are also considerable issues in postoperative resection cavity SRS [6163].
Preoperative SRS may be an alternative adjuvant option to postoperative SRS or RT. Preoperative SRS can sterilize tumor cells that spread during surgery. Furthermore, preoperative SRS can show effects similar to adjuvant SRS to eradicate microscopic invasion and avoid neurocognitive decline [6364]. The optimal dose and timing of preoperative SRS should be evaluated in future studies.
If there is another adjuvant treatment option, such as tyrosine kinase inhibitor (TKI) chemotherapy in non-small cell lung cancer, postoperative TKI chemotherapy can replace adjuvant SRS and RT in non-small cell lung cancer [6566].
Go to :
FUTURE DIRECTION
Innovations in neuronavigation, intraoperative ultrasound, brain mapping, endoscopy, exoscopy, and fluorescence have advanced BM surgery. Minimally invasive surgery has been widely used in brain tumor surgery [67]. Conventional craniotomies typically produce openings larger than the target, while keyhole craniotomies can create small openings smaller than the target with complete exposure achieved by subtending the angles of the approach. Keyhole approaches minimize soft tissue and bony exposure, decrease postoperative complications, and improve cosmetic results [68]. However, minicraniotomies, including the keyhole approach, require a learning curve [69] and should be applied to patients after adequate training and sufficient experience.
Endoscopic surgery can be used in BM surgery, including the endoscopic endonasal approach (EEA) or the endoscopic transorbital approach (ETOA) [7071]. Zacharia et al. [70] reported a case series of EEA for sellar/parasellar metastatic tumors. They reported very low complication rates, such as cerebrospinal fluid leakage; however, the gross total resection rate was below 50%. EEA can be used for tissue confirmation of the unknown etiology of parasellar tumor; however, there are inherent limitations of total or wide resection of the parasellar area.
Tumors in the temporal lobe or insular area can be treated with ETOA. Park et al. [71] reported the feasibility of ETOA for intrinsic brain tumors in the temporal lobe. There has been a lack of reports of ETOA for metastatic tumor surgery; it may be used in selected cases.
Fluorescence-guided surgery using 5-aminolevulinic acid (ALA) has been used in BM surgery [7273]. Ahrens et al. reported the benefits of 5-ALA in BM surgery [1374]. Previous studies reported the benefits of 5-ALA in BM surgery [7374]. However, not all BM tumors showed positivity for 5-ALA fluorescence; only approximately 60% of BM tumors showed 5-ALA fluorescent staining [7475]. The 5-ALA fluorescent is well detected in the aggressive pathology of metastatic tumors [74]. However, 5-ALA staining can be observed in the area of peritumoral edema that is free of tumor cells [76], which is related to false positivity of 5-ALA fluorescent staining in BM. Therefore, tailored usage of 5-ALA is needed in BM surgery.
Brachytherapy involves the implantation of radioactive isotopes into the tumor cavity and has been investigated as both primary and adjuvant therapy for BMs. Radioactive materials, such as 131Cs and 125I, are commonly used for brachytherapy [7778]. Brachytherapy shows local control rates comparable to SRS. In addition, brachytherapy showed improvement in neurocognitive status and self-assessment of quality of life [79]. The use of brachytherapy as an adjuvant treatment after surgical resection of BM should be included in future studies.
Go to :
CONCLUSION
Neurosurgical advances have altered the treatment of patients with BM, the most common adult brain tumor. The role of surgery in BM has been refined and its use has not been weakened in BM treatment. Total resection and obtaining a safe resection margin are the goals of surgery to improve the local control rate. En-bloc resection may lead to good local control and decreased intraoperative dissemination. Postoperative radiotherapy or chemotherapy can reduce the incidence of local recurrence. Minimally invasive BM surgery can be applied for BM surgery to shorten the recovery period and improve cosmetic results. Preoperative SRS and brachytherapy have highlighted improvements in clinical outcomes.
Go to :
 XML Download
XML Download