

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rathke’s cleft cysts (RCCs) are thought to be undegenerated epithelial remnants of the embryogenic Rathke’s pouch [123]. RCCs are usually located within the sellar turcica or with both intrasellar and suprasellar components, and lie between the pars anterior and the pars intermedia of the pituitary gland [123]. Most lesions are between 10–20 mm in diameter and contain mucoid or gelatinous substance encapsulated in a thin cyst wall of simple pseudostratified cuboidal or columnar epithelium [4]. Patients with symptoms are rare, but the most common presenting symptoms include headaches, visual disturbance, and pituitary hormone abnormalities [4]. Symptomatic RCCs can be treated by surgical procedure with low morbidity and mortality, usually through an endonasal transsphenoidal corridor using either a microscope or an endoscope [5]. Simple cyst fenestration is preferred to cyst wall resection to prevent surgical complications such as cerebrospinal fluid (CSF) leakage and hormonal disturbance [67]. However, recurrence after simple fenestration or marsupialization is relatively common and reported to be 9.6%–42.9% [6]. In addition, RCC combined with suprasellar cyst is neurosurgically challenging, like craniopharyngioma, because of their proximity to the vital structures and surgical complications [8].
Here, we report a case of a large suprasellar extended RCC causing obstructive hydrocephalus, which was efficiently managed by a novel surgical route named “reverse” trans-sellar approach using a transventricular neuroendoscope instead of the conventional trans-sellar approach. Surgical goals, including drainage of cyst contents and relief of hydrocephalus without complications, were successfully achieved through surgery.
CASE REPORT
A 48-year-old woman complained of persistent headache and a tendency to fall that had begun 6 months before visiting our clinic. She also presented with intermittent aggressive behavior, mild confusion, and dullness. There were no visual disturbances or hormonal dysfunctions. No other neurological abnormalities were observed.
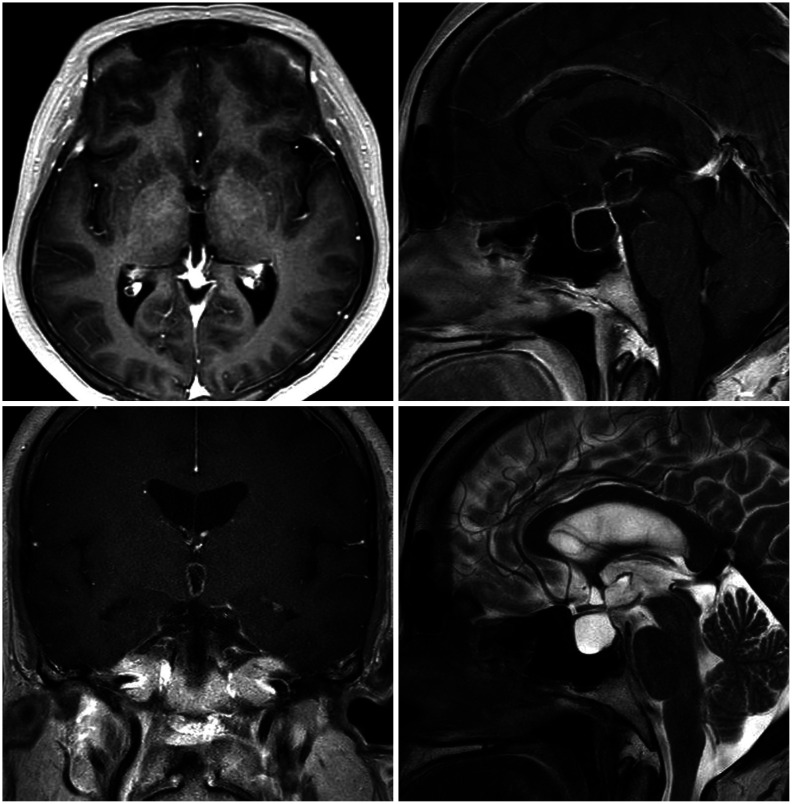
Preoperative MRI scan revealed an intrasellar cyst with a huge suprasellar extension (shape of ‘8’) which occupied the entire third ventricle (Fig. 1). T1-weighted gadolinium-enhanced axial, coronal, and sagittal images showed intra- and supra-sellar cystic masses occupying the third ventricle with obstruction of the foramina of Monro and aqueduct of Sylvius. The cystic wall showed a slight enhancement and the cystic contents showed iso-signal intensity on T1- and T2-weighted images.
The patient was admitted and the cystic mass was decided to be removed. Instead of trans-nasal trans-sellar surgery, we decided to operate using a conventional transventricular endoscope. The decision was made considering the location and size of the tumor. It was thought that access to the foramina of Monro and the aqueduct of Sylvius as well as the floor of the third ventricle for ventriculostomy would be easier and lesion removal would be necessary to relieve obstructive hydrocephalus.
Under general anesthesia, the operation was performed with the patient in the supine position, and a burr-hole was placed 2 cm anterior to the coronal suture and approximately 3 cm lateral to the midline. Then, the operator used a cannula to puncture the ventricle and inserted the endoscope with the guidance of the navigation system (StealthStation™ S8, Medtronic, Minneapolis, MN, USA) and continuous irrigation fluid.
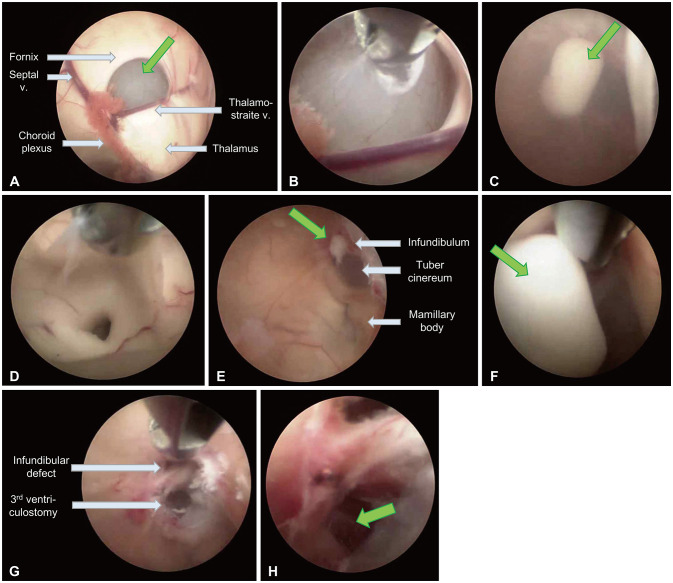
Foramina of Monro was identified and it was found to be obstructed by the cyst wall (Fig. 2A). A thin cystic capsule was fenestrated using a bipolar coagulator and widened using forceps (Fig. 2B). A cloudy cystic fluid spread out, which was a mixture of CSF and mucinous cyst content (Fig. 2C). The cyst wall was partially removed, and the cyst wall fragments covering the aqueduct of Sylvius were completely removed (Fig. 2D). Whitish mucinous cystic contents spilled out from the sellar cavity through the defect on the infundibulum when the sellar compartment was compressed using forceps, and this was removed completely (Fig. 2E and F). The thinned tuber cinereum was perforated and widened using forceps, and infundibular tissues around the defect were collected for histological examination as well as for widening the reverse transsellar corridor (Fig. 2G). Endoscopic examination through the infundibular corridor and the site of the third ventriculostomy confirmed the absence of residual cystic contents and the basilar artery, respectively (Fig. 2H). There was a risk of chemical meningitis due to internal cystic fluid drainage, but the risk was minimized by using steroids after surgery. Fortunately, no abnormalities were observed.
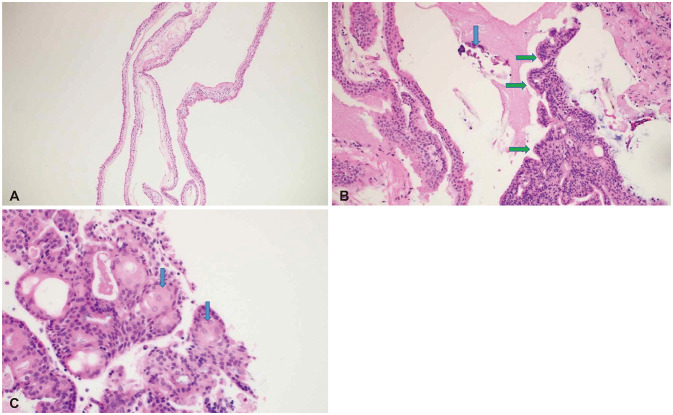
Histological examination showed that the cyst was lined with a single cell layer of ciliated cuboidal or columnar epithelium (Fig. 3A). The cystic lesion contained eosinophilic mucoid materials with focal calcification and the lesion partly demonstrated solid proliferation of epithelial cells with palisading columnar cells at their periphery (Fig. 3B). The lesion also showed squamoid epithelial cells with a vague whirling pattern (Fig. 3C). The final pathological finding revealed a Rathke’s cleft cyst with focal metaplasia.
After the surgery, the patient was immediately relieved of the headache and appeared alert. No abnormal findings were observed during the hospitalization, and the patient was discharged 7 days after surgery without any complications. During the 1 year follow up at the outpatient clinic, MRI showed resolution of the hydrocephalus and residual sellar lesion with a shrunken and fragmented suprasellar cyst (Fig. 4). The corridor between the sellar and suprasellar cysts remained stable.
DISCUSSION
RCCs are the most common incidentally discovered sellar lesions, followed by pituitary adenomas [9]. During general autopsies, RCCs are encountered in 13%–33% of normal pituitary glands [10]. In a retrospective review of 2,598 patients undergoing at least one pituitary MRI scan from 1999 to 2009 in a tertiary pituitary center, non-adenomatous sellar masses accounted for 18% of visible lesions, of which RCCs were the most frequent (19%) [11]. They has been reported in all age groups and occur most often between the age of forties and sixties [12]. RCCs are usually present in intrasellar and/or suprasellar cysts, and are rarely present only in the suprasellar region [13]. The case of suprasellar extension from the sellar turcica was observed in 16%–97% of RCCs, which has been variously reported according to the research [141516]. RCC extending to the third ventricle through the diaphragm and mimicking craniopharyngioma is extremely rare and seldom reported [17].
In general, RCCs are not treated in asymptomatic cases, but when symptoms are present, there is no objection to removing them to improve symptoms and prevent recurrence. Aho et al. [18] reported that radical resection of 118 patients did not appear to be associated with a decreased rate of recurrence; therefore the authors preferred less aggressive resection. In a recent meta-analysis, there was no conclusive evidence to determine differences in recurrence rates between a gross total resection and subtotal resection and drainage [19]. In general, the goal of surgery for symptomatic RCC includes the drainage of cystic contents and the relief of symptoms without surgical morbidities.
In recent times, the surgical method using a transsphenoidal approach with an endoscope has been preferred over the traditional microscopic transsphenoidal surgery [20]. Some surgeons reported advantages of endoscope over microscopic surgery because of better lighting and wider panoramic visualization of important structures [21]. In particular, the endoscopic approach is known to have a lower complication rate, better tolerance, and a shorter hospital stay than microscopic surgery [22]. In a recent meta-analysis, patients treated with the microscopic transsphenoidal approach had slightly higher rates of recurrence and endocrine dysfunction than those treated with the endoscopic sphenoid approach [19]. However, suprasellar RCCs are surgically difficult because of their close vicinity to the optic chiasm and infundibulum. A case series reported seven patients with suprasellar RCCs and surgery via endoscopic endonasal transtuberculum sellar approach relieved headache effectively and safely with the preservation of endocrinologic functions [23]. A retrospective review reported that compared to microsurgery, the extended endoscopic endonasal approach was associated with a significantly improved rate of complete RCC removal and improved visual outcomes, along with somewhat better headache outcomes [8]. However, extended trans-sphenoidal surgery is prone to the risk of CSF leaks, rhinonasal complications and damage to the hormonal axis [24]. To date, no case of RCCs surgery through the trans-ventricular endoscopic approach has been reported.
In this patient, we focused on resolving hydrocephalus, which caused the symptoms, and drainage of the cystic component. This was a rare case in which RCC had grown into the third ventricle, and obstructive hydrocephalus had occurred due to its size and shape. Although the transsphenoidal approach was effective in this patient, high-flow CSF leakage was predicted and the removal of the cyst wall blocking the foramina of Monro and the aqueduct of Sylvius was uncertain; additional shunt operation would most likely have been necessary. Therefore, considering the location and size of the tumor, we chose an unusual surgical approach rather than a more popular approach, and we named it reverse trans-sellar neuroendoscopic surgery.
There may be several concerns to this new approach. Some authors reported close relationship between RCC and craniopharyngioma [2526]. Though the treatment was primarily decided depending on the MRI findings of RCC and histologic examination confirmed RCC rather than craniopharyngioma, the possible transformation to craniopharyngioma should be checked regularly. In addition, internal cystic drainage has a risk of unexpected adverse events in later period such as chemical irritation and CSF circulation blockade. The authors decided the surgical strategy because of the following reasons: 1) simple intrasellar cyst fenestration might be insufficient to treat the patient; 2) the lesion blocked completely both foramina Monro and aqueduct of Sylvius which were not favorable regions to inspect or manipulate via transnasal endoscopic surgery; 3) the authors thought that high-flow CSF leakage might be forecasted after managing the lesion and the third ventricle through the diaphragm and defect on the third ventricular floor. Though this technique is not suitable for use in general RCCs, but is a relevant alternative method in highly selective cases. Long-term follow-up for the confirmation of efficacy and safety may be warranted.
In this report, we efficiently managed a large RCC by transventricular neuroendoscopic surgery with cyst fenestration and third ventriculostomy, and simultaneously drained the sellar contents using a novel surgical route. Reverse trans-sellar neuroendoscopic surgery is a relevant treatment option for selective patients with large suprasellar extending RCCs.

 XML Download
XML Download