

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Encephaloceles are protrusions of the brain parenchyma through osseous defects of the skull base or cranial vault [1]. It may develop congenitally (similar to the neural tube defect) or may occur after acquired events, such as infection, trauma, neoplasms, and iatrogenic causes [23]. The incidence of the congenital form has been estimated at 1 in every 3,000–10,000 live births [4]. Many classification systems for encephalocele have been suggested; however, the most accepted is that from Matson [5], which follows the location of the encephalocele: basal, sincipital, convexity, and atretic. These lesions are usually along the midline, ranging from the nasal to the occiput, where three-quarters encephaloceles occur posteriorly [6].
In cases where the defect occupies only the dura and inner table with an intact outer table of the skull, parenchymal herniation occurs in the intradiploic space and are called intradiploic encephaloceles [7]. Especially, off the midline parietal encephaloceles are rare, comprising only 1% of all cerebrospinal malformations and 10% of encephaloceles [28]. Here, we report a case of parietal intradiploic encephalocele during a 2-year follow-up with CT and MR images.
CASE REPORT
A 52-year-old man was referred for further evaluation of a skull osteolytic lesion on CT due to intermittent headache for 7 months. He had no history of seizures, central nervous system infections, stroke, brain tumor, or trauma. His neurological examination was normal, without any palpable mass or pulsation on his scalp. We proceeded with MRI to exclude osteolytic lesion such as vascular lesions or other tumorous conditions. We confirmed a herniation of the brain parenchyma with the surrounding cerebrospinal fluid (CSF) space into the diploe. These confirmed a diagnosis of right parietal intradiploic encephalocele (Fig. 1). The headache was controlled with medicines without neurological symptoms and signs. Two-year follow-up CT findings showed no change in the lesion (Fig. 2) and the patient doing well without symptoms.
DISCUSSION
Intradiploic encephalocele refers to brain parenchyma herniation into a diploic space with a destroyed inner table and an intact outer table [7]. Intradiploic encephalocele has characteristics that distinguish it from classic encephaloceles. In fact, it is debatable whether the nomenclature reflects the true nature of this disease and should be referred to as brain herniation into the calvaria surrounding the CSF [9].
Intradiploic encephaloceles share more common morphological features with expanding skull fractures and intradiploic arachnoid cysts [2]. Causes are unclear, but the mechanism of lesion may be similar with the “growing skull fracture” [27]. Cranial fractures in childhood can lead to a growing skull fracture [1011]. Fracture with a dural tear may cause herniation of the arachnoid tissue through the dural defect, and the fracture is gradually enlarged, and bone margins are separated by the continuous pulsation of the CSF [12]. In some cases, the CSF and brain tissue may herniate into the diploic cavity through a dura and inner table defect without damaging the outer table. The integrity of the outer table can be elucidated by a strong occipital muscle and pericranium that prevent bone erosion from the pulsation of CSF [13].
A similar mechanism can also be developed for low-velocity blunt injury that causes fracture only in the thinner inner table. The cracked inner table depresses and rebounds during initial insult. The depression then tears the dura, and the recoil creates a negative pressure that forces the underlying arachnoid and brain into the diploic space [14]. The lesion then grew with CSF pulsation.
As in the present case, anatomical factors are considered more important because of the lack of history of acquired risk factors. An anatomical and physiological defect of the cranial inner table, foveolae granulare, generate intradiploic encephalocele [15]. These granulations are usually located in the frontoparietal bone and near the superior sagittal sinus. In a situation of head trauma, the dura and arachnoid membranes rupture without skull fracture. CSF pulsation then widens the intradiploic space over time. Communication could also allow the brain parenchyma to escape into the diploic space.
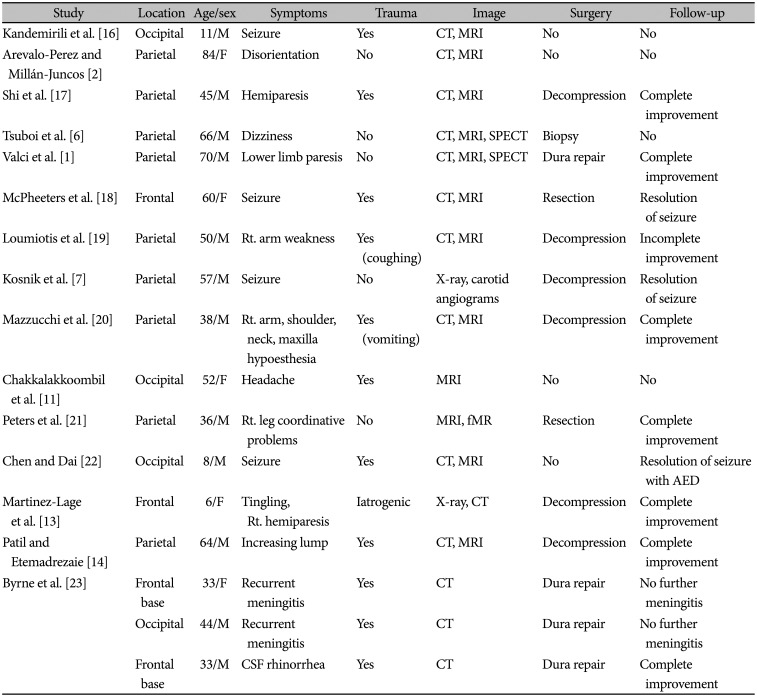
In the literature, 10 patients (10/17 cases) presented with seizure activity or neurologic deficits (Table 1). Others have non-specific symptoms such as headache, dizziness, and cognitive problems. Most intradiploic encephaloceles were found incidentally. Various symptom presentations might be related to the location of involvement; herniation of the eloquent cortex may cause non-specific symptoms. Some patients could present with acute onset of clinical symptoms when a sudden increase in intracranial pressure occurs, such as in an episode of vomiting or coughing. Surgery was performed in 13 cases if the radiologic findings corresponded to the clinical findings. The main purpose of surgery is to repair the dural defect along with the decompression of the herniated cortex.
The differential diagnosis of an osteolytic calvarial lesion in both pediatric and adult populations includes eosinophilic granuloma, plasmacytoma, metastasis, hemangioma, epidermoid or dermoid cyst, and intradiploic arachnoid cyst [1]. The confirmation of a herniated brain parenchyma through the osseous defect into the diploic cavity by MRI is the most important feature that separates intradiploic encephalocele from other possible diagnoses.
Intradiploic encephalocele is extremely rare, and the present case adds to the existing literature. The diagnosis of the lesion can be with typical MRI findings. MRI shows osteolytic lesion involved inner layer of skull and presence of herniated brain tissue within the diploic space. Understanding this condition helps to facilitate diagnosis and avoid confusion with vascular and malignant lesions. Ultimately, it provides adequate management and prevents potential surgery in asymptomatic patients.


 XML Download
XML Download