

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chordomas are rare, malignant, primary bone tumors with poor prognosis. They only account for 1%–4% of all primary bone tumors which are thought to arise from ectopic embryonic notochord remnants along the neuroaxis [123]. Although, not common, chordoma is the most frequent primary malignant neoplasm of the sacrum [4]. It has been reported that the most common sites are the sacrum (40%–50%), spheno-occipital area (35%–40%), and the vertebral bodies (15%–20%) [56]. There are not many cases of extraaxial chordomas in the soft tissues and appendicular bones in the literature [789]. Chordoma occurs in approximately 0.08 per 100,000 cases annually, with a male predominance and peak incidence in the 5th decade [10]. Although, histologically considered to be a benign neoplasm, chordomas have a malignant potential due to a remarkable recurrence [10]. Nonspecific symptoms may lead to late diagnosis and consequently poor prognosis in patients with sacral chordoma [11]. The tumor can expand proximally to the foramina and causes neural canal obstruction and extend posteriorly with invasion to the muscles around pelvis, hip, and the sacroiliac joints. Anterior invasion to the rectum is uncommon due to presacral fascia [121314]. Chordoma is a slow-growing neoplasm with poor response to the chemotherapy and conventional radiotherapy. Thus, surgical resection is the first line of treatment [15]. Herein, we describe a 50-year-old man with a giant sacrococcygeal mass.
CASE REPORT
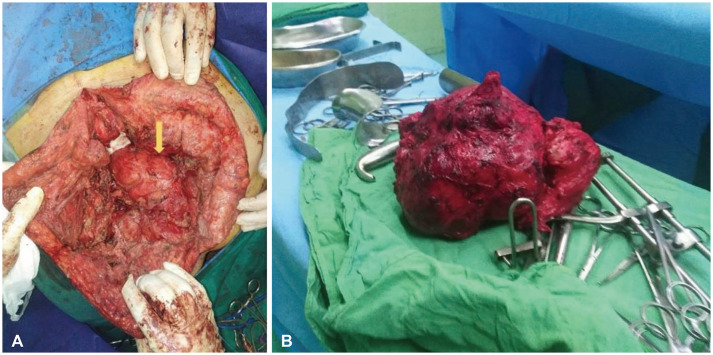
A 50-year-old male admitted to our hospital with a huge, obviously bulged sacrococcygeal mass (Fig. 1). Prior to this surgery, the patient had undergone another procedure on the lumbar area for mild canal stenosis. He complained a 10-months history of localized pain and foot drop in the left leg. In the physical examination, he had left foot drop and all other neurological examinations were normal. Sacrococcygeal CT and MRI revealed a giant heterogeneous mass, measuring 18×12 cm with invasion to sacrum, coccyx, iliac bone and gluteal muscles which was extended to pelvic cavity as well (Fig. 2).
Surgery was done in two stages. In the first stage, after general anesthesia, the patient positioned supine and secured to the table and all pressure points were padded. Midline vertical abdominal incision under umbilicus was done by a general surgeon.
After pelvic exploration rectal invasion was not seen so the bowel was pushed out and posterior peritoneum was opened. Left and right internal iliac arteries (feeder branches of the tumor) were explored and ligated with the help of a general surgeon. Anterior release of the mass was carried out and a loop sigmoid colostomy was created to decrease the risk of infection. The next day we performed the second stage. The patient positioned prone and a midline vertical incision was done in the lumbosacral region. After midline bilateral dissection of the fascia and the muscles of the lumbosacral region, a very large mass was exposed which had invaded the sacrum, coccyx, iliac bone, left sciatic nerve and the gluteal muscles. The sacroiliac joint had less than 50% involvement. After determination of S1 and S2 lamina with C-arm (fluoroscopy), S2 laminectomy was carried out with Kerrison rongeur and the thecal sac was ligated below S2 segment. Total en bloc resection of the well demarcated huge mass was carried out by using suction and bipolar cautery. The weight of this mass was 2,450 grams (Fig. 3). The tumor was very hemorrhagic with multiple vascular supplies. As noted above, the sciatic nerve was tumoral so it sacrificed. Because the lesion was placed below the S1–S2 level and involved less than 50% of sacroiliac joint, the spine stability was preserved so no devices were needed. Postoperative images are shown in Fig. 4.
Unfortunately, one week after the surgery, dehiscence occurred in the lower part of wound. Complete wound healing achieved with vacuum assisted closure after two months.
In follow up the patient still had left foot drop which was predictable due to the sciatic nerve involvement and resection. No other neurological deficits was seen.
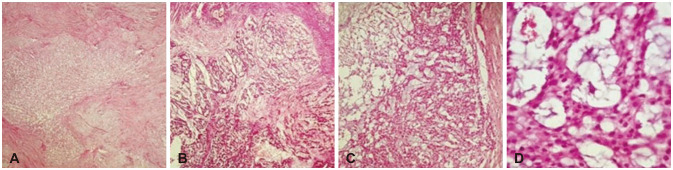
The huge lobulated mass, measuring 18 cm in the greatest dimension was sent for histopathological evaluation. The cut surface of the tumor was gelatinous and fleshy. Microscopic study revealed a neoplastic proliferation with lobular architecture and fibrous bands, which separated the lobules. The lobules were composed of cords, nests, and single cells of epithelioid cells within a myxoid matrix. Physaliphorous cells with bubbly cytoplasm were also noted (Fig. 5). To confirm the diagnosis, immunohistochemical studies were performed for cytoketatin (CK), epithelial membrane antigen (EMA), and S100 to rule out pathologic differential diagnoses, i.e., myxoid chondrosarcoma and mucinous carcinoma. As CK and EMA were positive, chondrosarcoma was ruled out and S100 positivity ruled out the possibility of carcinoma (Fig. 6).
DISCUSSION
Chordoma is a rare, slow-growing but locally invasive tumor. It accounts for less than 5% of all primary bone neoplasms [10]. Patients typically present in the 5th and 6th decade (mean age of 55 years old) and the majority of them are sacral chordomas [16]. Sacral chordoma produces vague clinical presentations, which provides challenges in early diagnosis for physicians. All these patients complained of low back pain, which commonly aggravates in the sitting position [1217]. One-third of the cases suffered from pain and radiculopathy due to the sciatic nerve or iliolumbar trunk compression [18]. A few patients with masses in the S1–S2 region reported weakness or unilateral loss of L5-S1 function [19]. The lesion can occur anywhere in the sacrum with preference toward the 2nd and 3rd sacral bodies [1320]. The destruction of L5-S1 junction and anterior ligament may result in pelvic instability. Moreover, the skin of the affected area may change due to the posterior extension of the tumor [4].
Conditions which mimic sacral chordoma should be considered. The top differential diagnosis is chondrosarcoma which mimics this tumor both histologically and radiologically. Thus, immunohistochemical studies are necessary to confirm the diagnosis. Chordoma would be positive for EMA and panCK. Other similar conditions are giant cell tumor and plasmacytoma. These tumors are aggressive and tend to extend to the sacroiliac joint which cause challenges in radiological assessment. Metastatic diseases, originating from carcinomas of prostate, breast, thyroid, lungs, and colon should always be kept in mind, especially in the elderly. Tuberculosis and fungal infections can mimic sacral chordoma as well [21].
In several studies, the tumor size has been reported as a predictor of surgical outcome, so that the sacral chordomas larger than 10 cm or 200 cm3 may cause an adverse prognosis [122223]. Recurrence and metastasis can occur for years post-surgery. Also it is reported that sacral chordoma can metastasize to some organs such as lung, bone, liver, lymph nodes, soft tissue, and skin [24].
Since chordoma is poorly sensitive to chemotherapy and radiotherapy, surgery is the treatment of choice [25]. For the preoperative evaluation, CT scan is necessary to identify the local bony extension and MRI is used to determine the sacrectomy level. Tumor resection with the least possible nerve injury is the purpose of surgery [192627]. Previous studies showed a correlation between the damage of the capsule around the tumor and higher rate of recurrence. Therefore, the capsule should be preserved carefully [1728].
It is important to protect the lumbosacral trunks and sciatic nerves as much as possible. The optimal approach for the tumor resection is controversial. Some surgeons believe an exclusive posterior procedure is beneficial, while others recommend a combined anterior and posterior approach. Nevertheless, studies showed that a mere posterior approach has provided good results with slightly lower rate of recurrence than the combined approach [2930].
In partially resected sacral chordomas, radiotherapy is not very effective. So to improve the survival and reduce the recurrence rate and morbidity of these patients, total resection is the cornerstone treatment.
After taking few parameters into account such as the tumor size, invasion to the surrounding tissues, and surgeon’s experience, the anterior and posterior approach was selected for this case.
The novelty of this case report was its huge size, special surgical (combined anterior and posterior) approach, and interdisciplinary cooperation between general surgeon and neurosurgeon.




 XML Download
XML Download