

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Spontaneous regression of tumors is defined as spontaneous remission of a tumor in the absence of any treatments [1]. Although the mechanisms of spontaneous regression remain unclear, they are known to include infection, apoptosis, or immune system activation [23]. Meningiomas, originating from the arachnoid cap cell, are the most common primary intracranial tumors in adults [45]. Meningiomas are generally slow-growing tumors [5]. But spontaneous regression of meningiomas has been rarely reported. We report a case of an incidentally diagnosed meningioma with spontaneous regression after 10 years.
CASE REPORT
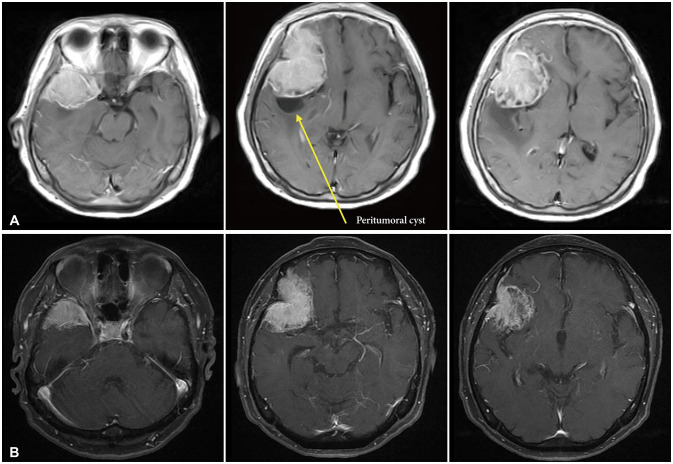
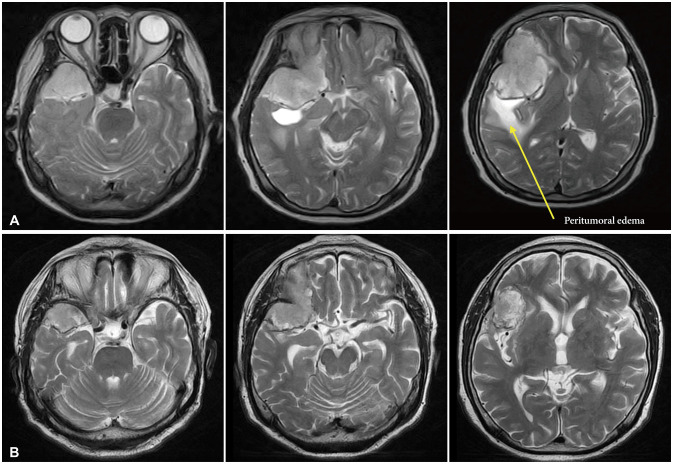
A 73-year-old female patient with an incidentally diagnosed meningioma was introduced to our hospital in 2012. She was diagnosed with type 2 diabetes mellitus (DM). She had no other past history of infections. There were no neurologic symptoms nor subjective complaints related to the tumor. Contrast-enhanced brain MRI revealed a large meningioma (47.04×40.18×62.31 mm) of the right sphenoid (Fig. 1A). This meningioma showed a high intensity on T2 MRI with significant edema (Fig. 2A). Blood sugar had been well controlled with medication-metformin. We planned operation. However, the patient refused surgical treatment. She was lost to follow-up at the outpatient department.
Ten years after, she was admitted to our hospital after checked contrast-enhanced brain MRI in 2022 due to decreased cognitive function five years ago. Blood sugar had been well controlled with medication-metformin. The MRI showed shrinkage of the meningioma to a size of 42.66×31.72×54.92 mm (Fig. 1B). This meningioma showed decreased edema on T2 MRI (Fig. 2B). She had not received any treatment such as gamma knife surgery, for meningioma. The initial volume (=length×depth×width×0.5) [6] was 58.59 cm3. It regressed to 37.16 cm3 10 years later. Since there were no other neurological symptoms, we decided to follow up this patient later.
DISCUSSION
Meningiomas are the most frequently diagnosed primary brain tumors [7]. Meningioma tumor growth shows a curve pattern [8]. But there have been very few reports of meningioma regressing spontaneously.
Kumaria et al. [9] have reported one patient with spontaneous regression of meningioma. They reported that the size of the meningioma was reduced from 36.0 cm3 to 11.2 cm3 over 7 years. In their study, although the mechanism was unclear, they considered that menopause might have induced tumor shrinkage. They also mentioned that microangiopathic changes on a histological level might have contributed to tumor shrinkage.
Hirota et al. [10] have reported one case of spontaneous regression of meningioma. They reported that the size of meningioma was reduced from 25.5 cm3 to 9.9 cm3 over 7 years. In their study, they considered that uncontrolled DM and insulin might be probable causes of the regression spontaneously.
Our hypothesis is that calcification of arteries can occur due to old age and DM, followed by a decrease in blood supply in tumor, which leads to a decrease in tumor size. DM causes various complications, and the association between DM and brain damage has been widely reported. According to Shukla et al. [11], DM increases the risk of cerebral ischemia. They reported that DM induced atherosclerosis, which might have increased the risk of ischemic stroke. DM was also present in our case, and it was presumed that the mass size was reduced by DM.
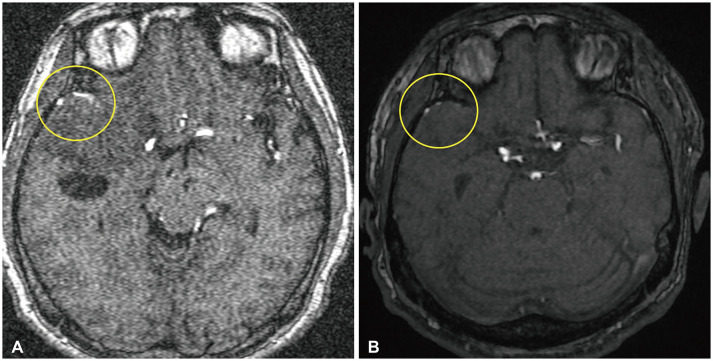
Atherosclerosis seen in spontaneous tumor regression might be similar to the effect after embolization in meningiomas. Several studies have reported a reduction in tumor volume following embolization, showing substantial tumor shrinkage after embolization feeders [12131415]. Although there is no clear blood vessel study such as cerebral angiography, our case showed that arteries on magnetic resonance angiography were less visible after tumor regression (Fig. 3).
In our case, a decrease in peritumoral edema was also seen as the tumor size decreased. We hypothesize that the decrease in peritumoral edema is the result of activation of collateral vessels. The relationship between peritumoral edema and collateral vessels has been described in other paper [16]. The function of collateral vessels pressed by tumor might be normalized due to the regression of tumor size, leading to a decrease in peritumoral edema. We also confirmed the regression of a peritumoral cyst. Although the exact cause of peritumoral cyst in meningioma has not been elucidated, an increase in collateral vessel function might be associated with a decrease in cyst.
Our study had several limitations. First, it is difficult to generalize our hypothesis as we report only one case. Second, no pathological tests were made to support the hypothesis. Further research will be needed on this point.
We reported a case of spontaneous regression meningioma. Through this case, if the patient is asymptomatic, further discussions should be considered whether early operation should be performed for large meningioma. And further studies are needed on the relationship between DM and spontaneous regression of meningioma.
 XML Download
XML Download