

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Meningiomas are the most common benign primary intracranial neoplasms. Their prevalence has increased with advances in diagnostic technology and increasing life expectancy [12]. Meningioma mostly occurs from the cerebral dura mater originating from arachnoid cap cells in arachnoid granulation. They are rarely discovered as primary intraparenchymal meningiomas originating from cap cells of the pia mater [34]. However, in some cases, meningiomas can originate from the choroid plexus stroma [5].
Most meningiomas are convexity meningiomas, followed by sphenoid wing, falx, and parasagittal meningiomas. Meningiomas in the ventricle are relatively rare; among them, the most common location is the lateral ventricle, and only around 8.7% of intraventricular meningiomas are located in the fourth ventricle [6]. Most intraventricular meningiomas are located in the atrium, which refers to the junction of the temporal horn, occipital horn, and lateral ventricle’s posterior body, but can also be found in any ventricular space containing the choroid plexus [78].
Here, we report a rare case of a meningioma originating from the choroid plexus of the foramen of Luschka, which extends to the cerebellopontine angle (CPA) and cerebellomedullary cistern without dural attachment.
CASE REPORT
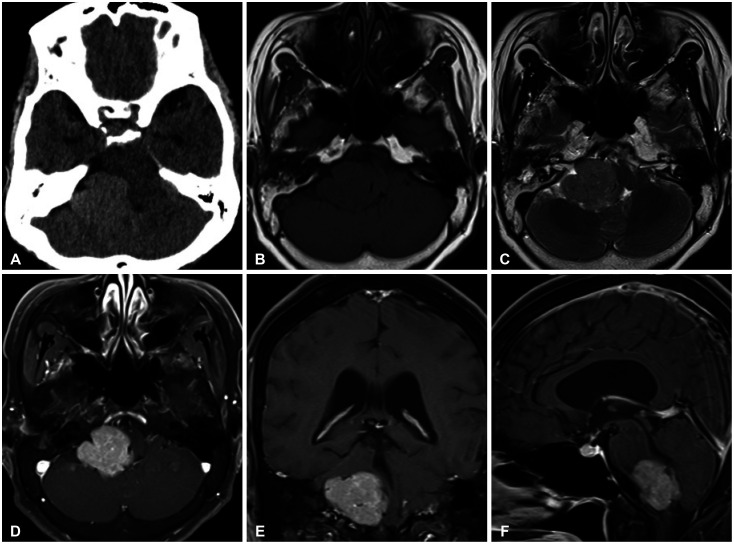
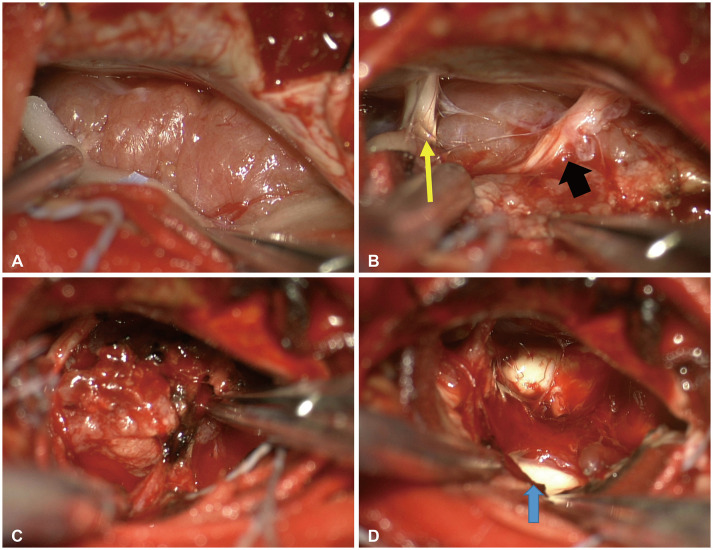
A 63-year-old female patient with a 2-year history of progressively worsening dizziness was admitted due to the new onset of swallowing difficulty. Neurological examination revealed ataxia and gait disturbance. She has had right-sided deafness since childhood and had hypertension as a comorbid disease. Brain CT showed a non-calcified mass in the right posterior cranial fossa (Fig. 1). The mass was round with clear margins, iso-/hypointense in T1-weighted images, and iso-/hyperintense in T2-weighted images. Brain MRI with gadolinium enhancement revealed a homogeneously enhancing mass in the right posterior cranial fossa. The mass size was 3.47×3.15×3.73 cm (tumor volume: 17.9 cm3). The tumor was pressing against the brain stem and the 4th ventricle from the side. However, the tumor was not accompanied by hydrocephalus. Surgical intervention was decided. Surgery was performed in the lateral position. The lesion was approached via retrosigmoid suboccipital craniotomy with bone removal and opening of the lateral border of the foramen magnum. Under an operating microscope, the dura was opened. After cerebrospinal fluid drainage from the cerebellomedullary cistern, the tumor was found with a clear cleavage plane and hypervascularization. Intercapsular debulking of the tumor was performed, followed by dissection of the capsule from the surrounding arachnoid. There was no damage to the cranial nerves 6–12 while removing the tumor. We identified and removed the choroid plexus of the foramen of Luschka, which appeared to be the site of tumor origin (Fig. 2). The mass was subjected to a gross total resection (Simpson grade I). The patient complained of aggravated swallowing difficulty on the first day after surgery, which gradually improved.
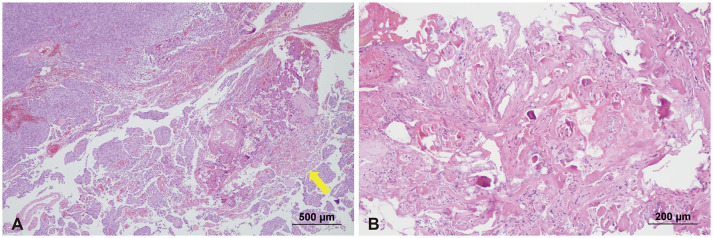
Histopathologic examination revealed a meningothelial meningioma (CNS WHO grade 1). There was moderate hypercellularity without signs of malignancy. There was no necrosis or invasion of the brain. Mitotic activity was up to 2–3/10 HPF. The Ki-67 proliferation index was 2%–3%. The normal choroid plexus was invaded by tumor cells (Fig. 3). Radiological follow-up with contrast-enhanced brain CT showed no residual tumor or decompression of the brain stem.
DISCUSSION
Meningiomas are known to originate from arachnoid cap or meningothelial cells, which not only can cluster on the arachnoid granulation surface but also can be located in the stroma of the choroid plexus, tela choroidea, and pia mater [9]. Most meningiomas are present as dural attachement extra-axial lesions. They are rarely found as intraventricular lesions [6].
Therefore, posterior fossa meningiomas without dural attachment (MWODA) are uncommon. MWODA can be classified into three categories according to Abraham and Chandy [10]: 1) meningiomas arising from the choroid of the 4th ventricle and lying wholly within it; 2) meningiomas arising from the inferior tela and lying partially in the 4th ventricle and partially in the cerebellar hemisphere; and 3) meningiomas lying in the cisterna magna. Shibuya et al. [11] added one category for meningiomas arising from the choroid plexus and lying in the lateral cerebellomedullary cistern in 1999. Gonzalez-Quarante et al. [12] reviewed 11 cases of extraventricular MWODA in the posterior fossa, including those not considered in the previous classification. In addition, there was one case of meningioma similar to ours originating near the foramen of Luschka [13].
Meningiomas originating from the choroid plexus of the foramen of Luschka and located in the CPA without dural attachment are very rare. There might be difficulties in diagnosing such cases. CPA MWODA should be differentiated from ependymomas, medulloblastomas, and lymphomas [14]. It is also important to differentiate between CPA meningiomas and choroid plexus meningiomas when determining the surgical approach because a gross total resection including the origin site is required in the case of intracranial meningioma surgery. Based on a radiological, histopathological, and literature review, our case was different from common CPA meningiomas for several reasons.
First, in CPA meningiomas, enhanced CT typically shows that the choroid plexus is separated from the tumor or moved to the side by the tumor; however, in our case, the choroid plexus was mixed with the tumor on enhanced CT (Fig. 4). Second, unlike dura-attached CPA meningiomas, access to the 5th cranial nerve was not required because the tumor was located in the lower CPA region in our case. As the tumor was pushing the 9th and 10th cranial nerves in the cephalad direction, it should be approached inferiorly after retrosigmoid suboccipital craniotomy. Third, pathological assessment revealed that the normal choroid plexus was invaded by tumor cells. According to Güngör et al. [15], normal choroid plexus tissue was observed in all intraventricular meningioma patients.
We report an extremely rare case of a lower CPA MWODA originating from the choroid plexus of the foramen of Luschka. For meningiomas located in the CPA, the origin site may be the choroid plexus. Therefore, sufficient imaging analysis might be necessary before surgery.

 XML Download
XML Download