

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Craniopharyngiomas are benign, epithelial tumors present in the sellar region and treated primarily by surgical resection and adjuvant therapy. Due to the proximity of the tumor to vital structures located in the anterior skull base, surgical resection remains challenging [1]. It can be performed through the traditional transcranial approach (TCA) or the increasingly adopted endoscopic endonasal approach (EEA) [2]. The EEA follows a ventral midline route and provides direct visualization of the midline suprasellar space. Approaching the tumor inferiorly allows better visualization of the tumor as it descends into the surgical field during dissection and allows visualization of its relation to the hypothalamus and optic chiasm. Transplanum, transsellar, transclival, and superior pituitary extended EEA approaches allow access to tumors within the optic chiasm and various extensions into the ventricles and parasellar regions [34]. However, the EEA may increase risks of postoperative cerebrospinal fluid (CSF) leak [5].
The TCA follows a lateral or subfrontal route and crosses cranial nerves, vascular structures including the internal carotid artery and its branches, and the optic apparatus before the tumor is accessed which may increase risk of damage to these structures [6]. In addition, it requires brain retraction and manipulation of neurovascular structures, which could result in edema, contusion, and venous compromise [7]. Systematic reviews assessing outcomes of the surgical resection of craniopharyngiomas are outdated and rely only on case series [8]. Therefore, we conducted a meta-analysis to synthesize recent evidence assessing the safety and effectiveness of the EEA in comparison to TCA for the resection of adult craniopharyngiomas.
MATERIALS AND METHODS
This systematic review was conducted after protocol registration (PROSPERO CRD42021272119) and reported following the PRISMA statement [9].
Search and selection
Randomized controlled trials (RCT), prospective cohort studies, and case series that compared EEA with TCA for resection of craniopharyngiomas in patients above 18 years of age were included. Inclusion of case series ensured that the review thoroughly consolidated available evidence. Articles where data for craniopharyngiomas in adult populations could not be extracted or calculated, either due to mixed cohorts or unavailability of individual data, were excluded. No restrictions regarding year of publication or language of the article were applied.
On July 9, 2021, the databases of PubMed, Web of Science, and Cochrane Library were systematically retrieved. The following keywords were used: ‘endonasal,’ ‘transsphenoidal,’‘transplanum,’ ‘trans sellar,’ ‘endoscopic,’ ‘endoscopic,’ ‘endoscopy,’‘endoscopy,’ ‘EEA,’ ‘transcranial,’ ‘pterional,’ ‘bitozygomatic,’‘frontolateral,’ ‘bifrontal,’ ‘frontobasal,’ ‘interhemispheric,’‘transpetrosal,’ ‘subtemporal,’ ‘transcallosal,’ ‘transcortical,’ ‘trans lamina terminalis,’ ‘TCA,’ ‘craniotomy,’ ‘microscopic,’ ‘microsurgical,’‘microsurgery,’ ‘microsurgery,’ ‘minimally invasive,’‘craniopharyngioma,’ ‘craniopharyngeal neoplasm,’ ‘craniopharyngeal neoplasm,’ ‘craniopharyngeal tumor’ (Supplementary Material in the online-only Data Supplement). The references of the included studies were also checked to find possible relevant articles. The search included registries of registered trials. The titles and abstracts of the articles were reviewed independently by two reviewers and the full texts of the articles that either reviewer found relevant were acquired with the input of a library consultant. Full texts were then assessed independently by two reviewers for relevancy and disagreements were settled by discussion and by consultation with a third reviewer.
Data extraction and study quality assessment
Data were extracted independently by two reviewers. A third reviewer was consulted in cases of disagreements. Data on the following variables were extracted: study population (number, age, and gender), tumor characteristics (volume, location, extension, consistency and calcification), and patient outcomes (postoperative complications, recurrence, 30-day mortality, and length of stay). Primary outcomes were 30-day mortality following surgery and postoperative CSF leak, stroke (ischemic), hypopituitarism, recurrence on subsequent follow-up, visual impairment, and hydrocephalus. Secondary outcomes identified were postoperative diabetes insipidus, length of stay, grand total resection, and intracranial infection.
The methodological quality of the included RCTs was evaluated independently by two reviewers based on the Cochrane Handbook for Systematic Reviews of Interventions, version 6.0 [10]. The following 5 item scales were assessed: 1) random sequence generation—selection bias; 2) allocation concealment—selection bias; 3) blinding of the participants and personnel— performance bias; 4) blinding of outcome assessments—detection bias; and 5) selective reporting—reporting bias. Each of the items needed to be measured as "Yes" (low risk of bias), "No" (high risk of bias), or "Unclear" (unclear risk of bias). The risk of bias summary figure was obtained using the Robvis visualization tool [11]. The methodological quality of the cohort studies was assessed using the Newcastle Ottawa Scale [12]. The scale uses a star system to assess quality of studies based on selection, comparability of groups, and ascertainment of outcome. Bias was assessed at the study level. The methodological quality of the case series was evaluated using the tool for evaluating the methodological quality of case series and case reports. It consists of eight items, categorized into four domains: selection, ascertainment, causality, and reporting. Five items pertinent to this review were selected by the authors. Each item was given 1 point and measured as “Yes” (low risk of bias) or “No” (high risk of bias). The total score was then calculated by adding the score allotted to each item. Disagreements between the two reviewers in judgment of the quality of the study were settled by discussion and consultation with a third reviewer. The conflict of interest and source of funding reported by all the studies included was also recorded.
Data synthesis
In reporting of categorical outcomes, risk ratios (RRs) with 95% confidence intervals (CIs) were used. Continuous data was analyzed as standard mean differences with similar 95% CIs. Pooled participant data from the identified cohort studies were included in a random-effects model (Mantel-Haenszel method) meta-analysis using RevMan Version 5.4 and displayed in Forest plots [13]. Heterogeneity of subgroups was calculated using I2 statistic with an I2 >40% assumed to represent significant heterogeneity, as recommended in the Cochrane Handbook for Systematic Reviews of Interventions, version 6.1 [10].
RESULTS
Study selection
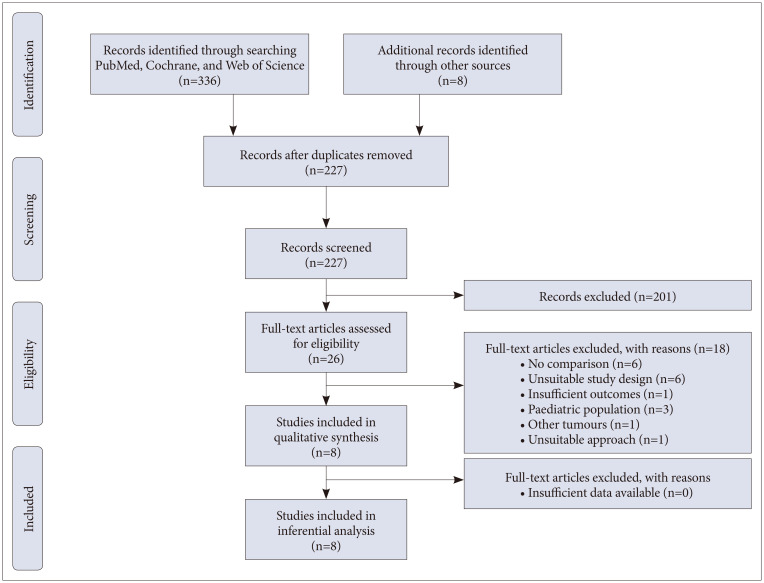
A total of 344 articles were identified from literature databases and through reference and citation searches. After exclusion of duplicates, there were 227 remaining, which were assessed for relevance by reviewing the title and abstract. As a result, 26 articles were found relevant, and, despite the absence of language restriction in the search and selection strategy, the full text was available all in English. After the exclusion criteria were applied, a total of eight articles were included in the final systematic review (Fig. 1) [214151617181920].
Study characteristics
A total of 11,395 subjects were compared for EEA and TCA in the eight included studies [214151617181920]. Age and sex ratio (male:female) were reported in seven studies [2141617181920]. The mean age ranged from 40.3±15.5 to 52.4±17.2 years and the male:female ratio ranged from 0.31 to 3 in EEA and 0.55 to 2.66 in TCA (Table 1). Four studies used an extended endoscopic approach (Supplementary Table 1 in the online-only Data Supplement).
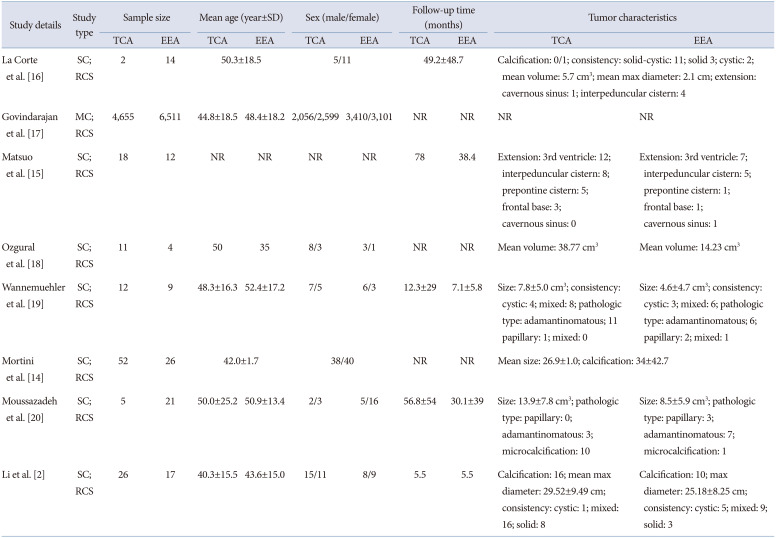
Table 1
Characteristics of patients in studies included in the meta-analysis on endoscopic endonasal versus transcranial resections of adult craniopharyngioma
| Study details | Study type | Sample size | Mean age (year±SD) | Sex (male/female) | Follow-up time (months) | Tumor characteristics | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| TCA | EEA | TCA | EEA | TCA | EEA | TCA | EEA | TCA | EEA | ||
| La Corte et al. [16] | SC; RCS | 2 | 14 | 50.3±18.5 | 5/11 | 49.2±48.7 | Calcification: 0/1; consistency: solid-cystic: 11; solid 3; cystic: 2; mean volume: 5.7 cm3; mean max diameter: 2.1 cm; extension: cavernous sinus: 1; interpeduncular cistern: 4 | ||||
| Govindarajan et al. [17] | MC; RCS | 4,655 | 6,511 | 44.8±18.5 | 48.4±18.2 | 2,056/2,599 | 3,410/3,101 | NR | NR | NR | NR |
| Matsuo et al. [15] | SC; RCS | 18 | 12 | NR | NR | NR | NR | 78 | 38.4 | Extension: 3rd ventricle: 12; interpeduncular cistern: 8; prepontine cistern: 5; frontal base: 3; cavernous sinus: 0 | Extension: 3rd ventricle: 7; interpeduncular cistern: 5; prepontine cistern: 1; frontal base: 1; cavernous sinus: 1 |
| Ozgural et al. [18] | SC; RCS | 11 | 4 | 50 35 | 8/3 | 3/1 | NR | NR | Mean volume: 38.77 cm3 | Mean volume: 14.23 cm3 | |
| Wannemuehler et al. [19] | SC; RCS | 12 | 9 | 48.3±16.3 | 52.4±17.2 | 7/5 | 6/3 | 12.3±29 | 7.1±5.8 | Size: 7.8±5.0 cm3; consistency: cystic: 4; mixed: 8; pathologic type: adamantinomatous; 11 papillary: 1; mixed: 0 | Size: 4.6±4.7 cm3; consistency: cystic: 3; mixed: 6; pathologic type: adamantinomatous; 6; papillary: 2; mixed: 1 |
| Mortini et al. [14] | SC; RCS | 52 | 26 | 42.0±1.7 | 38/40 | NR | NR | Mean size: 26.9±1.0; calcification: 34±42.7 | |||
| Moussazadeh et al. [20] | SC; RCS | 5 | 21 | 50.0±25.2 | 50.9±13.4 | 2/3 | 5/16 | 56.8±54 | 30.1±39 | Size: 13.9±7.8 cm3; pathologic type: papillary: 0; adamantinomatous: 3; microcalcification: 10 | Size: 8.5±5.9 cm3; pathologic type: papillary: 3; adamantinomatous: 7; microcalcification: 1 |
| Li et al. [2] | SC; RCS | 26 | 17 | 40.3±15.5 | 43.6±15.0 | 15/11 | 8/9 | 5.5 | 5.5 | Calcification: 16; mean max diameter: 29.52±9.49 cm; consistency: cystic: 1; mixed: 16; solid: 8 | Calcification: 10; max diameter: 25.18±8.25 cm; consistency: cystic: 5; mixed: 9; solid: 3 |
![]()
Risk of bias within studies
Six studies were reported as good quality [21417181920] and two were reported fair quality [1516] according to the Newcastle Ottawa Scale Criteria (Table 2). All studies received the maximum in the ‘selection’ and ‘ascertainment of outcome’ criteria. There were concerns present in the comparability of cohorts as data was collected using a retrospective design and cohorts were not matched for characteristics of the craniopharyngioma studies and were unable to control for tumor characteristics and age and sex of patients [14151617].
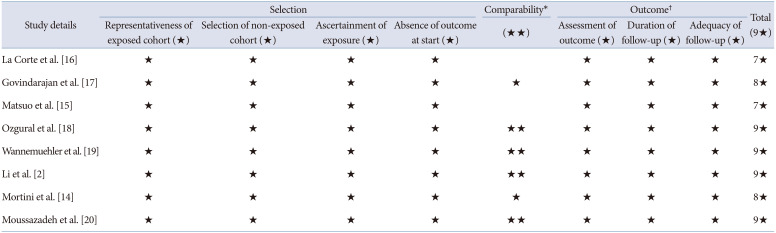
Table 2
Quality assessment of cohort studies using Newcastle-Ottawa Scale for meta-analysis on endoscopic endonasal versus transcranial resections of adult craniopharyngioma
| Study details | Selection | Comparability* | Outcome† | Total (9★) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of exposed cohort (★) | Selection of non-exposed cohort (★) | Ascertainment of exposure (★) | Absence of outcome at start (★) | (★★) | Assessment of outcome (★) | Duration of follow-up (★) | Adequacy of follow-up (★) | ||
| La Corte et al. [16] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 7★ | |
| Govindarajan et al. [17] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 8★ |
| Matsuo et al. [15] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 7★ | |
| Ozgural et al. [18] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 9★ |
| Wannemuehler et al. [19] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 9★ |
| Li et al. [2] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 9★ |
| Mortini et al. [14] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 8★ |
| Moussazadeh et al. [20] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 9★ |
*Comparability assessed as the following: one star rewarded if study controlled for the volume and extension of the tumor, another star rewarded if study adjusted or controlled for age and sex of patients; †Adequacy of follow-up was assessed as the following: one star rewarded if all subjects accounted or if subjects lost to follow up unlikely to introduce bias, i.e., >80% subjects present.
![]()
Primary outcomes (Table 3)
30-Day mortality
Incidence of mortality was analyzed in five studies including 241 patients undergoing TCA and 30 patients undergoing EEA [1416171920]. The risk of 30-day mortality was significantly lower (RR=5.63, 95% CI 3.87–8.19, p<0.00001, I2=0%) after EEA (Fig. 2A).
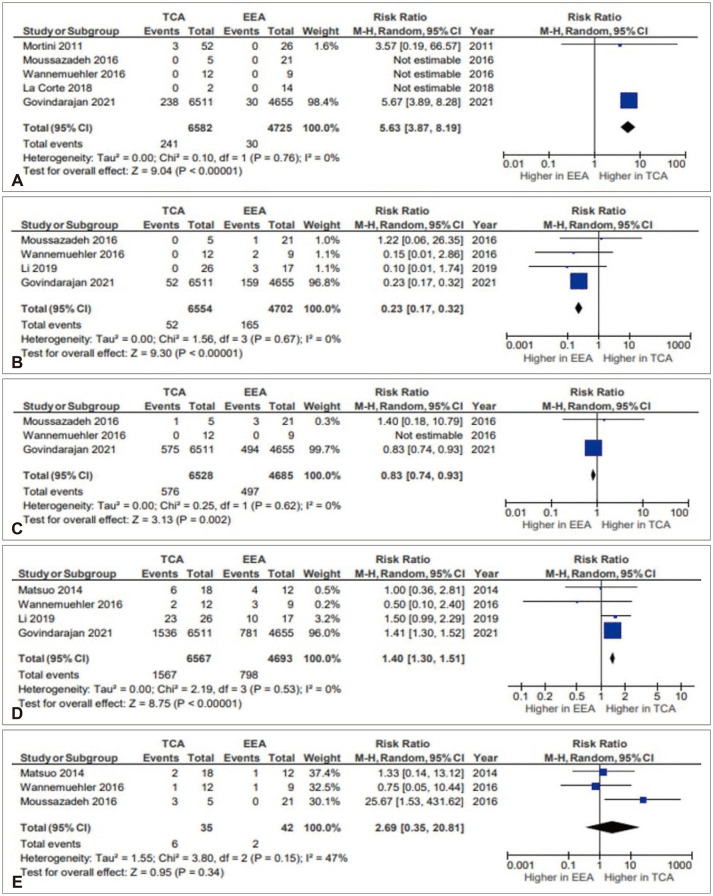
Fig. 2
Incidence of 30-day mortality (A), cerebrospinal fluid leakage (B), stroke (C), hypopituitarism (D), and recurrence (E) in studies included in the meta-analysis on endoscopic endonasal versus transcranial resections of adult craniopharyngioma [2141516171920]. EEA, endoscopic endonasal approach; TCA, transcranial approach; M-H, Mantel-Haenszel method; CI, confidence interval.
![]()
Hydrocephalus
Postoperative hydrocephalus was reported in three studies and included 1,165 patients undergoing TCA and 119 patients undergoing EEA [171819]. The risk of hydrocephalus was significantly lower (RR=6.95, 95% CI 5.78–8.36, p<0.00001, I2=0%) in EEA group (Fig. 3A).
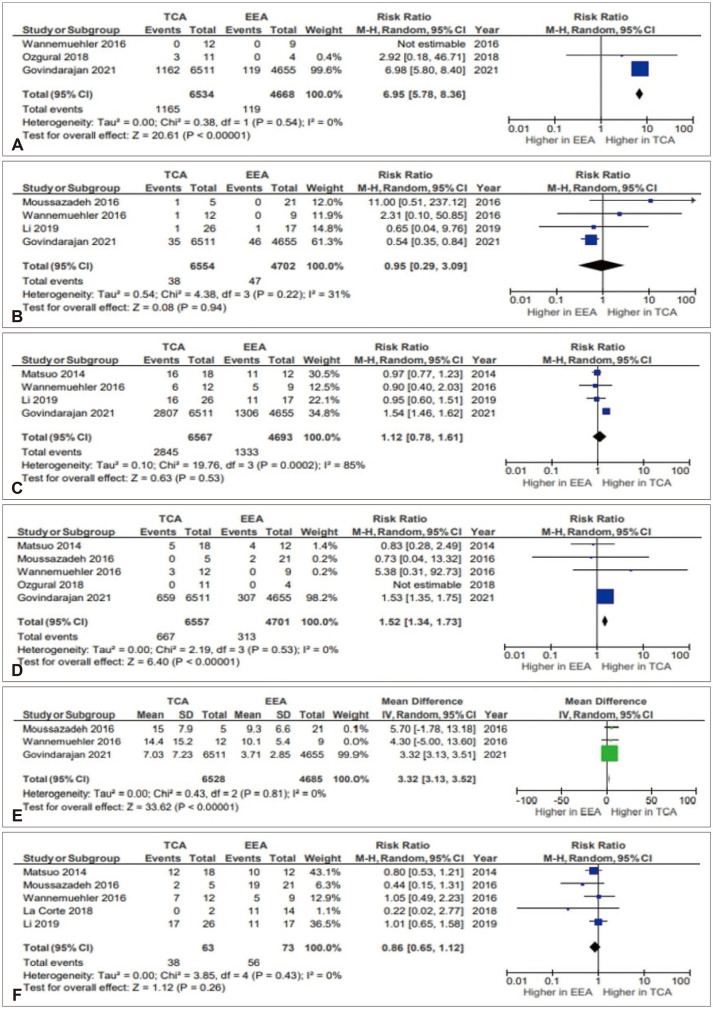
Fig. 3
Incidence of hydrocephalus (A), intracranial infection (B), diabetes insipidus (C), visual impairment (D), length of stay (E), and gross total resection (F) in studies included in the meta-analysis on endoscopic endonasal versus transcranial resections of adult craniopharyngioma [21517181920]. EEA, endoscopic endonasal approach; TCA, transcranial approach; M-H, Mantel-Haenszel method; CI, confidence interval; SD, standard deviation.
![]()
Table 3
Primary postoperative surgical outcomes of patients in studies included in the meta-analysis on endoscopic endonasal versus transcranial resections of adult craniopharyngioma
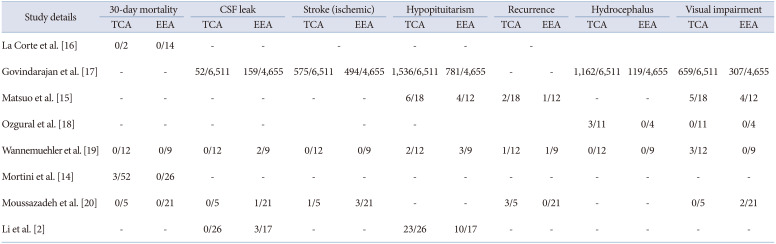
| Study details | 30-day mortality | CSF leak | Stroke (ischemic) | Hypopituitarism | Recurrence | Hydrocephalus | Visual impairment | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TCA | EEA | TCA | EEA | TCA | EEA | TCA | EEA | TCA | EEA | TCA | EEA | TCA | EEA | |
| La Corte et al. [16] | 0/2 | 0/14 | - | - | - | - | - | - | - | - | - | - | - | - |
| Govindarajan et al. [17] | - | - | 52/6,511 | 159/4,655 | 575/6,511 | 494/4,655 | 1,536/6,511 | 781/4,655 | - | - | 1,162/6,511 | 119/4,655 | 659/6,511 | 307/4,655 |
| Matsuo et al. [15] | - | - | - | - | - | - | 6/18 | 4/12 | 2/18 | 1/12 | - | - | 5/18 | 4/12 |
| Ozgural et al. [18] | - | - | - | - | - | 3/11 | 0/4 | 0/11 | 0/4 | |||||
| Wannemuehler et al. [19] | 0/12 | 0/9 | 0/12 | 2/9 | 0/12 | 0/9 | 2/12 | 3/9 | 1/12 | 1/9 | 0/12 | 0/9 | 3/12 | 0/9 |
| Mortini et al. [14] | 3/52 | 0/26 | - | - | - | - | - | - | - | - | - | - | - | - |
| Moussazadeh et al. [20] | 0/5 | 0/21 | 0/5 | 1/21 | 1/5 | 3/21 | - | - | 3/5 | 0/21 | - | - | 0/5 | 2/21 |
| Li et al. [2] | - | - | 0/26 | 3/17 | - | - | 23/26 | 10/17 | - | - | - | - | - | - |
![]()
Secondary outcomes (Table 4)
Diabetes insipidus
Incidence of postoperative diabetes insipidus was analyzed in four studies including 2,845 patients undergoing TCA and 1,333 patients undergoing EEA [2151719]. The risk of diabetes insipidus in EEA was lower (RR=1.12, 95% CI 0.78–1.61, p=0.53, I2=85%) compared to TCA and the values were statistically not significant (Fig. 3C).
Gross total resection
Incidence of gross total resection (GTR) was analyzed in five studies including 38 patients undergoing TCA and 56 patients undergoing EEA. The GTR was non-significantly higher after EEA (RR=0.86, 95% CI 0.65–1.12, p=0.26, I2=0%) (Fig. 3F).
Publication bias
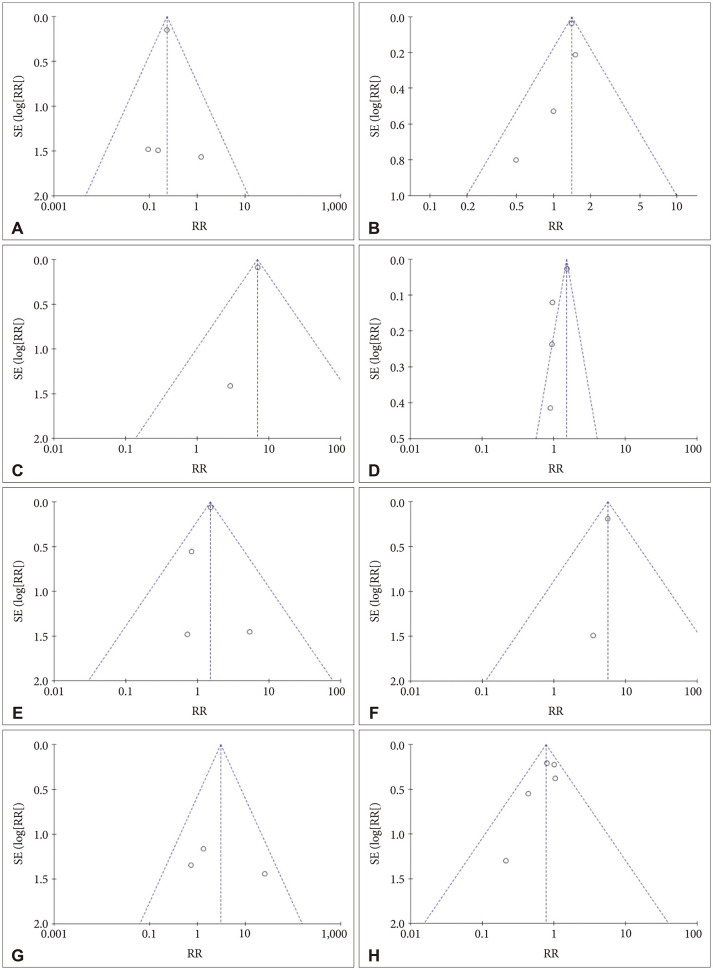
Table 4
Secondary surgical outcomes of patients in studies included in the meta-analysis on endoscopic endonasal versus transcranial resections of adult craniopharyngioma
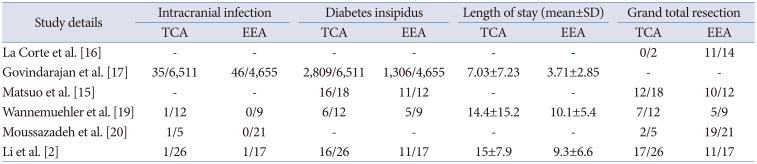
| Study details | Intracranial infection | Diabetes insipidus | Length of stay (mean±SD) | Grand total resection | ||||
|---|---|---|---|---|---|---|---|---|
| TCA | EEA | TCA | EEA | TCA | EEA | TCA | EEA | |
| La Corte et al. [16] | - | - | - | - | - | - | 0/2 | 11/14 |
| Govindarajan et al. [17] | 35/6,511 | 46/4,655 | 2,809/6,511 | 1,306/4,655 | 7.03±7.23 | 3.71±2.85 | - | - |
| Matsuo et al. [15] | - | - | 16/18 | 11/12 | - | - | 12/18 | 10/12 |
| Wannemuehler et al. [19] | 1/12 | 0/9 | 6/12 | 5/9 | 14.4±15.2 | 10.1±5.4 | 7/12 | 5/9 |
| Moussazadeh et al. [20] | 1/5 | 0/21 | - | - | - | - | 2/5 | 19/21 |
| Li et al. [2] | 1/26 | 1/17 | 16/26 | 11/17 | 15±7.9 | 9.3±6.6 | 17/26 | 11/17 |
![]()
DISCUSSION
Our systematic review and meta-analysis is an update to the current understanding of outcomes for surgical approaches for adult craniopharyngiomas. As minimally-invasive endoscopic surgery finds its place in the neurosurgeon’s armament, indications for approaches should be based on the rate of postoperative complications.
Summary of main results
Data collected from cohort studies showed a significantly higher 30-day mortality rate in the TCA group, with low heterogeneity from our analysis. The lower rates of mortality may reflect recent improvements in surgical technique and perioperative management. Tumor recurrence was higher in the transcranial group; data were however heterogeneous and non-significant, warranting further prospective trials for evaluation.
Endoscopic approaches may result in significantly shorter hospital stays for patients in comparison to TCA. This can be affected by postoperative complication rates that have been previously identified as independent predictors of hospital length of stay [21]. Our analysis showed significantly higher rates of postoperative hydrocephalus, stroke, hypopituitarism, and visual impairment in the TCA group. Rates of postoperative diabetes insipidus and intracranial infection were non-significant in either cohort, and we did not find sufficient data in the included studies to warrant comparison regarding cardiovascular, respiratory, or wound complications.
A higher risk of CSF leak was seen after EEA surgery; this is expected as skull base approaches can increase the risk of CSF leak [22]. This has been greatly reduced with the use of vascularized nasoseptal flaps, as has been studied in recent literature [35]. Advanced endoscopic skull base reconstruction techniques show promising results for improvement of CSF leak after surgery, and should be further evaluated.
GTR was evaluated in five studies—although data were homogenous, the results were non-significant. Therefore, surgeons can be more confident in endoscopic resection providing the same extent of resection as TCAs.
Agreements/disagreements with literature
A meta-analysis previously conducted in 2018 took into account all adult craniopharyngioma cohorts and compared outcomes between EEA and TCA groups [23]. A key limiting factor was that only one study was included that directly compared both approaches. Pooled analysis showed higher rates of visual and endocrine symptoms in the EEA group, and no differences in hypopituitarism or diabetes insipidus. Recurrence was also similar in both groups. However, there was significant heterogeneity reported. Our study builds on these findings by providing stronger evidence through comparable cohort studies and homogenous data. Previous systematic reviews have recommended endonasal approaches to be indicated in midline adult-onset craniopharyngiomas, showing improved GTR and outcomes, both endocrinological and visual [24]. They also showed that the rate of CSF leak was strongly diminished with the use of multilayer reconstruction techniques. TCAs were advocated for use in laterally extending or purely intraventricular tumors. However, recent literature has shown endoscopic surgery for craniopharyngiomas with intraventricular extension shows similar outcomes to transcranial surgery [2526]. Similarly, CSF leak rates were brought down with the use of nasoseptal flaps in this approach.
Quality of evidence
There is a discrepancy in study samples sizes, with one study accounting for a majority of the included patient population for certain outcomes [17]. This is to be expected as this study was done through retrospective national database assessment. However, the authors only focused on specific clinical outcomes, and therefore other studies played a larger role in our analysis of surgical outcomes (GTR, recurrence). Secondly, a majority of studies were retrospective chart reviews, with few studies blinding for outcome assessment where possible (radiological tumor outcomes for instance). Lastly, patient cohorts were not matched to account for confounding factors. The size of tumor and its anatomical location can affect the outcomes of a surgical approach and are important scientific questions.
Our study is the first meta-analysis on adult craniopharyngiomas to pool together studies where cohorts were compared. We included standardized outcomes and showed statistical significance within our data set.
Conclusion
This study demonstrates lower complication rates, shorter hospital stays, and lower mortality associated with endoscopic adult craniopharyngioma surgery in comparison to open approaches. EEA may however be correlated with higher rates of CSF leak, warranting further subset analysis of the effect seen by improved skull base reconstruction and vascularized nasoseptal flaps techniques. These findings do not account for difference in tumor size and extension between the EEA and TCA cohort. Further research on patients with comparable tumor characteristics is required to fully assess outcomes, particularly for rates of tumor recurrence and achieving GTR.
 XML Download
XML Download