

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Leptomeningeal metastasis (LM), a terminal disease in which cancer cells spread via the cerebrospinal fluid (CSF), affects 5%–10% of patients with solid tumors, particularly melanoma, breast, lung, and ovarian cancers and primary brain tumors [1]. LM has a poor prognosis, as the life expectancy after diagnosis is 4–6 weeks without treatment [12].
LM is challenging to treat in many ways. Localized radiation has a limited role, as the disease is disseminated along the entire neuraxis [3]. Systemic chemotherapy is ineffective due to the blood–brain barrier [4]. Intra-CSF chemotherapy, administered either intrathecally or intraventricularly, can maintain therapeutic drug concentrations in the CSF for 48–72 hours [5]; however, a marginal survival benefit of 3–6 months and risks of neurotoxicity have raised questions about its effectiveness [67].
Infiltration of the CSF space by cancer cells may obstruct CSF pathways and cause CSF malabsorption, resulting in increased intracranial pressure (ICP) or hydrocephalus [8]. Common presenting symptoms of LM include headache, nausea, vomiting, and altered mental state, all of which are related to increased ICP/hydrocephalus. Furthermore, increased ICP interferes with the distribution of intrathecally or intraventricularly administered drugs, making them less effective against LM [9].
In our previous study, we showed that CSF shunting (including both ventriculoperitoneal [VP] and lumboperitoneal [LP] shunts) benefits LM patients by alleviating ICP-related symptoms and improving overall survival (OS) [10]. However, the shunting of ventricular CSF by VP shunts precludes the distribution of intraventricularly injected drugs to the extra-ventricular CSF space, preventing access to progressive LM. Thus, intraventricular chemotherapy is impractical in LM patients who have received a VP shunt. By contrast, the LP shunt, which detours CSF from the thecal sac to the peritoneum, could allow intraventricularly injected drugs to travel through the subarachnoid space to reach the lumbar CSF. Therefore, we hypothesized that combining an LP shunt with an Ommaya reservoir would enable the continuation of intraventricular chemotherapy while controlling ICP.
This retrospective study evaluated the feasibility of a combined LP shunt and Ommaya reservoir in patients with LM. The primary objectives were to 1) show the distribution of intraventricularly injected drugs to lumbar CSF samples and evaluate the pharmacokinetics of methotrexate, such as the elimination half-life; and 2) measure adverse events associated with the procedure and drug administration. The secondary objectives were to evaluate the number of intraventricular MTX chemotherapy sessions using this combination system and the OS of patients.
Go to : 
MATERIALS AND METHODS
Patients’ eligibility
This retrospective review was based on the electronic medical records of 16 consecutive patients with LM who received both an Ommaya reservoir and an LP shunt, either concurrently or sequentially, and received continuous intraventricular chemotherapy after the installation between 2002 and 2021 at our institution. All patients were diagnosed by CSF cytology and had a suggestive or definite finding of LM on gadolinium-enhanced MRI [11]. Increased ICP (>20 cm H2O) was confirmed either at LM diagnosis or during treatment. This retrospective study was reviewed and approved by the Institutional Review Board of the National Cancer Center of Korea (NCC2014-0135).
Operative procedure
Ommaya reservoirs were installed as previously described [12]. Briefly, an elongated semicircular incision was made to the anterior third, centered at Kocher’s point. After burr hole trephination on Kocher’s point, an Ommaya reservoir (Baxter, Heyer-Schulte, Deerfield, IL, USA), Chemoport (B. Braun, Boulogne, France), or H-port (Insung Medical, Seoul, Republic of Korea) [12] was secured according to the manufacturer’s protocol and connected to a ventricular catheter, which was inserted via a planned trajectory to a predefined depth using a stereotactic system (CRW, Seolim Medical, Seoul, Republic of Korea). LP shunt installations were performed under general anesthesia in a lateral position, as described in previous studies [1314]. A spinal subarachnoid catheter was introduced through a 3-cm-long incision at L3–L4 or L4–L5. A Tuohy needle (14-gauge) was inserted into the CSF space with or without fluoroscopy guidance, followed by the insertion of a small diameter proximal catheter up to 10 cm. A semicircular to hockey stick–shaped incision was made on the anterior superior iliac spine to secure a valve reservoir (Spetzler LP shunt system, Intergra NeuroScience, Phoenix, AZ, USA; or Strata LP shunt, Medtronic, Goleta, CA, USA). After connecting proximal and distal catheters to the valve reservoir, a distal catheter was inserted through an incision made at McBurney’s point into the periosteum.
Endpoints and clinical variables
The primary endpoints were 1) the confirmation of drug distribution in CSF samples obtained from Ommaya and LP shunt reservoirs and associated pharmacokinetic data; and 2) adverse events associated with the procedure and drug administration. Secondary endpoints included the number of MTX chemotherapy sessions administered after the combined system installation and the OS of patients. Survival time was calculated from either the date of LM diagnosis or the date of shunt placement until the date of death or last follow-up visit. Clinical variables, such as demographic profile, preoperative Karnofsky Performance Status (KPS) score, systemic cancer status, the extent of LM, and previous treatment for LM, were analyzed as possible factors affecting the shunt results.
Statistical analysis
Pharmacokinetic data were obtained automatically using GraphPad Prism software (version 3.0; San Diego, CA, USA). The elimination half-life of intraventricularly injected MTX was calculated under the assumption of a ‘first-order reaction,’ as follows [15]:

where t1/2 is the half-life of the drug, [R0] is the baseline MTX concentration measured at the ventricular reservoir, [R] is the MTX concentration obtained via the LP shunt reservoir at a given time (t), and k is the rate of drug elimination.
Although this first-order reaction is a rough model, we assumed that the half-life calculated in this fashion would estimate the time required for drug in the ventricle to reach the LP shunt reservoir.
Kaplan–Meier curves were used to analyze OS using the Statistical Package for the Social Sciences (version 18; SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
Patient characteristics
Sixteen patients (13 female, 3 male) underwent both LP shunt and Ommaya reservoir insertion and eventually received post-operative intraventricular chemotherapy during the study period (Tables 1 and 2). The median patient age was 55 years (range: 18–70 years). The median preoperative KPS score was 60 (range: 50–90). The burden of systemic cancer was classified as progressive disease (n=9), partial response/stable disease (n=5), and no evidence of disease (n=2). The extent of LM, as determined by gadolinium-enhanced MRI, was confined to either the brain (n=6), the spine (n=2), or both (n=8). Treatment for LM prior to LP shunt installation included no treatment (n=2), CSF chemotherapy (n=8), or both CSF chemotherapy and radiation therapy (n=6).
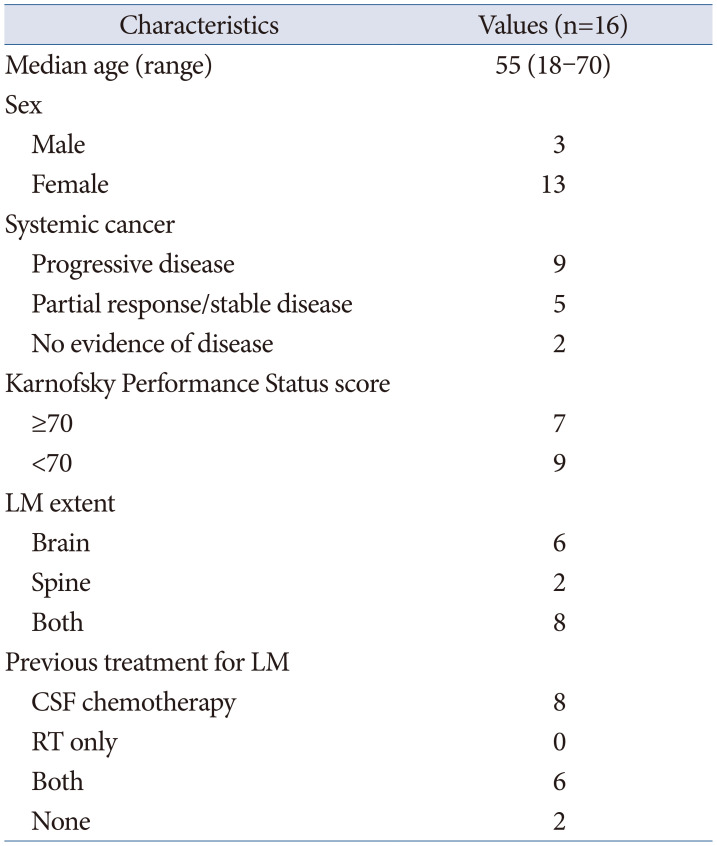
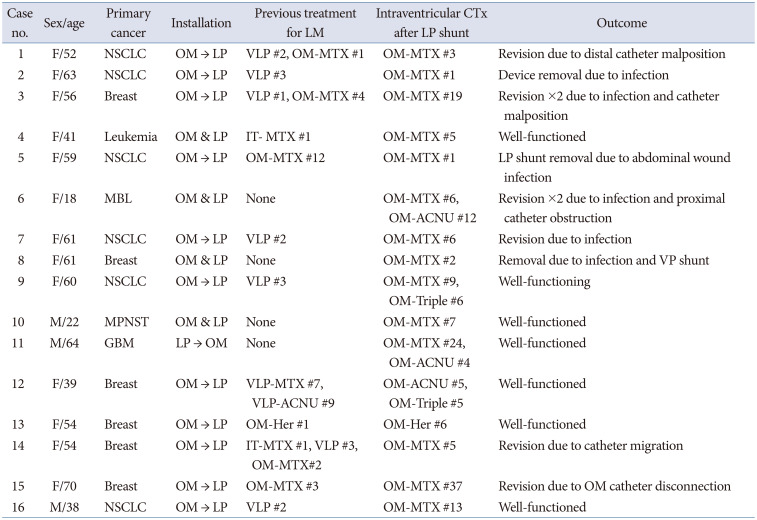
Table 1
Characteristics of patients with leptomeningeal carcinomatosis receiving CSF shunt operation
![]()
Table 2
Description of LP shunt installation and rounds of intraventricular chemotherapy
LP, lumboperitoneal; LM, leptomeningeal metastasis; CTx, chemotherapy; NSCLC, non-small cell lung cancer; MBL, medulloblastoma; MPNST, malignant peripheral nerve sheath tumor; GBM, glioblastoma; OM, Ommaya; VLP, ventriculolumbar perfusion chemotherapy; MTX, methotrexate; IT, intrathecal; ACNU, nimustine; Her, herceptin; VP, ventriculoperitoneal
![]()
Compatibility of the combined Ommaya reservoir and LP shunt for intraventricular chemotherapy with pharmacokinetics
After the placement of the Ommaya reservoir and LP shunt, catheter function was confirmed by smooth aspiration and injection through the Ommaya reservoir, prompt refill of the LP shunt reservoir on thumb pressure, and simple X-ray confirming appropriate catheter placement. To obtain pharmacokinetic evidence supporting the CSF distribution of intraventricularly administered chemotherapy, we sampled the Ommaya reservoir 0.5 h after administration and sampled the LP shunt reservoir 6 and 12 h after administration in six patients. Chemotherapeutic drug concentrations were measured in each sample and plotted according to the time elapsed after administration of intraventricular chemotherapy (Fig. 1A). The initial mean MTX concentration measured at the Ommaya reservoir was 610.4±419.7 µM and varied (range 339.9–1,523.5 µM) depending on ventricular CSF volume (data not provided). The MTX concentration measured at the LP shunt reservoir ranged from 7.4 to 59.5 µM at 6 h (mean 43.8±29.3 µM) and from 1.1 to 52.7 µM at 12 h (mean 24.5±19.5 µM). To obtain the MTX elimination rate from the ventricle, we normalized the LP shunt reservoir concentration (R) to the initial Ommaya reservoir concentration (R0) to obtain a ratio (R/R0) that reflects the final concentration relative to the baseline concentration (Fig. 1B). Relative drug concentrations were more uniform than naïve MTX concentrations, and the mean ratios at 6 and 12 h were 0.08±0.05 and 0.05±0.05, respectively. The elimination half-life (t1/2), calculated under an assumption of first-order kinetics (see MATERIALS AND METHODS), was 2.63 h. Based on this, we concluded that intraventricular MTX chemotherapy was effectively distributed throughout the CSF at a uniform rate in patients with combined Ommaya reservoir and LP shunt.
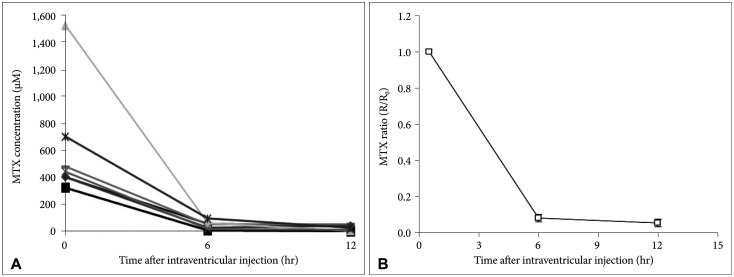 | Fig. 1Pharmacokinetics of intraventricular MTX distribution from the ventricle to LP shunt reservoir. A: MTX concentrations in cerebrospinal fluid. B: MTX ratios were calculated as the ratio of the MTX concentration obtained via the LP shunt reservoir at a given time (R) to the baseline MTX concentration at the ventricular reservoir (R0). MTX, methotrexate; LP, lumboperitoneal.
|
Complications associated with the combined Ommaya and LP shunt system
The median follow-up time was 5.2 months (range: 0.9–66.2 months, 95% confidence interval [CI]: 3.7–6.3 months) after the LP shunt installation. Nine patients (56%) underwent revision surgery due to malfunction (n=3), infection (n=4), or both (n=2). The average time between the initial surgery and the revision surgery was 0.74±0.36 months (22.2±10.8 days). Two patients required a second revision surgery. Three patients underwent complete removal of both the LP shunt and the Ommaya reservoir due to infections (Cases 2, 5, and 8) diagnosed at the time of the intraventricular chemotherapy or within 2 weeks after the installation. Two of these cases (Cases 5 and 8) received VP shunts for the management of increased ICP.
The median number of intraventricular chemotherapy sessions was seven (range 1–37). CSF infections attributable to intraventricular injection (>2 weeks after system installation) occurred in three patients (Cases 3, 6, and 7). After Case 8, we adopted a higher level of aseptic technique for intraventricular sampling and injection. No further CSF infections occurred, but one Ommaya catheter disconnection and one distal catheter migration occurred.
Overall survival
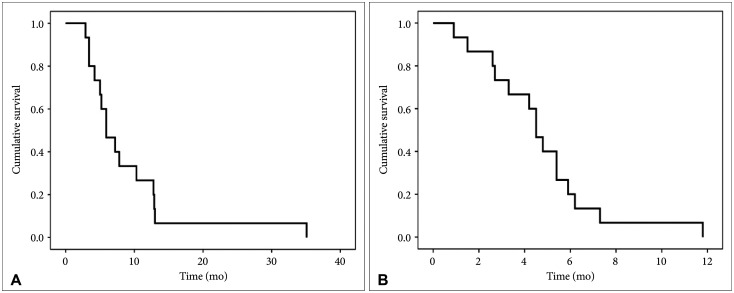
All patients had died at the time of retrospective observation, except one patient with leukemia who went into complete remission after receiving a bone marrow transplantation (Case 4). Perceiving a difference between LM prognoses for solid cancer and hematologic malignancy, we excluded this patient from the OS analysis. Thus, the median survival of 15 patients was 5.9 months (range: 2.9–35.1 months, 95% CI: 3.4–8.4 months) after LM diagnosis and 4.5 months (range: 0.9–11.8 months, 95% CI: 3.7–5.3 months) after LP shunt insertion (Fig. 2).
Go to :
DISCUSSION
Continuation of intraventricular chemotherapy
Few effective treatment options exist for LM, as chemotherapy drugs must cover the whole neuraxis and avoid neurotoxicity. Systemic chemotherapy has a limited role, as these drugs rarely penetrate the blood–brain barrier apart from epidermal growth factor receptor inhibitors in non-small cell lung cancer (NSCLC) [2]. Patients with bulky localized disease may benefit from radiation therapy, but whole-brain radiation therapy often results in cognitive dysfunction and fails to prolong patient OS [3]. Among these treatment options, intra-CSF chemotherapy with MTX—a hydrophilic drug with well-studied pharmacokinetics [59161718]—is frequently performed. Some studies report a survival benefit with no immediate neurotoxicity, but these studies were not prospective randomized controlled trials [11920]. Other studies insist that long-term neurotoxicity surpasses the marginal OS benefit [67]. In our previous study, we verified that intraventricular chemotherapy increased OS among patients with LM due to NSCLC [20]. Using the time-dependent covariates method, we showed that more rounds of intraventricular chemotherapy (median five rounds) correlated with significantly prolonged OS. The median number of intraventricular chemotherapy rounds in this study was seven. Therefore, we conclude that the continuation of intraventricular chemotherapy in patients with an LP shunt to control ICP may have additional survival benefits over intra-CSF chemotherapy in the absence of a shunt.
Complications associated with the combined Ommaya reservoir and LP shunt system
Ommaya reservoirs have been used to access ventricular CSF for both sampling and intraventricular drug injection [17]. However, CSF infection and device malfunction have been reported with the use of Ommaya reservoirs, including rare but serious complications of encephalitis and hemorrhage around the ventricular catheter [182122]. To prevent complications associated with chemotherapeutic agents such as intraventricular hemorrhage or wound dehiscence, we adopted a solid chamber Chemoport in place of an Ommaya reservoir (starting with Case 4) and did not note the incidence of encephalitis, hemorrhage, or wound dehiscence around the ventricular catheter in this study. The only Ommaya reservoir–associated complication was ventricular catheter disconnection from the Chemoport due to the loosening of the tie knot (Case 15).
LP shunts were developed as early as 1960, allowing for the avoidance of cranial surgery and for small ventricle access in communicating hydrocephalus [2324]. Earlier versions of the LP shunt lacking a programmable valve reservoir were associated with problems including over-drainage, kinking/migration of the catheter, and difficulty assessing shunt patency [232526]. Recent LP shunt versions with a programmable valve reservoir showed compatible efficacy in controlling hydrocephalus as VP shunts [1327]. Among five cases of LP shunt malfunction in this study, three cases involved distal catheter migration or disconnection from the valve in obese patients (Cases 1, 3, and 14). We routinely anchored the LP shunt reservoir on the pelvic muscle fascia, but in obese patients where the fascia was not readily visible, we anchored the reservoir on subcutaneous fatty tissue, which resulted in catheter migration. After such catheter migrations were noted, we meticulously identified pelvic muscle fascia even in obese cases, and strengthened anchoring measures using purse-string sutures. The other case of malfunction (Case 6) involved proximal catheter inlet obstruction by cancer cells in a medulloblastoma patient whose spine MRI showed a subarachnoid block from leptomeningeal spread. No other cases of catheter obstruction related to cancer cell seeding or sludge accumulation were reported during the study period.
CSF infection due to intraventricular chemotherapy rather than system installation is an inherent potential problem of this combined system, necessitating the removal of all installed systems to control the infection, in addition to antimicrobial therapy [1213]. Repeated chemotherapy injections and CSF sampling through the Ommaya reservoir and LP shunt increase the infection risk; thus, these manipulations require aseptic techniques. In our study, the earlier cases were frequently associated with higher rates of infection. Furthermore, Staphylococcus or Streptococcus species were identified in all infection cases, confirming that infection occurred via the percutaneous route (individual data not provided). In earlier cases, we used a simple aseptic technique with only local betadine sterilization, simple gloving and open dressing after Ommaya reservoir manipulation. After Case 8, we adopted complete aseptic CSF manipulation techniques and guidelines, consisting of chlorhexidine sterilization, complete surgical draping and gowning, followed by semi-occlusive dressing. No further cases of CSF infection were reported afterwards.
There have been other attempts to continue intraventricular chemotherapy in LM patients with increased ICP. Burger et al. [28] reported use of a VP shunt equipped with an ‘on-off’ valve, enabling for both intraventricular injection and CSF drainage in a single device. However, this system precludes simultaneous CSF drainage while intraventricular injection, which may result in transient increase in ICP. Furthermore, there is insufficient evidence proving that intraventricular injection of chemotherapeutic agents eventually distribute throughout the subarachnoid space, where metastatic cancer cells reside.
In conclusion, despite the poor prognosis associated with LM, patients with LM experiencing increased ICP can benefit from combined Ommaya reservoir and LP shunt installation to allow for continued intraventricular chemotherapy. Furthermore, LP shunt malfunctions can be reduced with surgical experience, and infections associated with the intraventricular injection can be prevented with a careful aseptic technique.
Go to :
 XML Download
XML Download