

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Glioblastoma multiforme (GBM) is the primary grade IV brain malignancy and carries a fatal prognosis. Despite significant advances in molecular understanding and predictive biomarkers identification, only a handful of drugs are currently approved for GBM [1]. The standard treatment for GBM involves combinational therapies including surgical resection, chemotherapy, and radiotherapy [2]. Nevertheless, the survival rate for patients with GBM is still less than one year [34]. From a clinical point of view, effective treatment of GBM is limited by several challenges. First, the anatomical complexity and size of the tumor influence the extent of resection. This is because a fine balance must be struck between maximum removal of malignant tissue and minimum surgical risk [5]. Even with safe operative resection, residual infiltrating GBM cells that cannot be detected by imaging techniques remain in the tumor periphery, leading to disease progression and inevitable death [6]. Second, the central nervous system features distinctive microenvironment that is surrounded by the blood-brain barrier (BBB), restricting systemically delivered drugs from accessing the brain. This reduces the treatment options available for GBM. Additionally, GBM is characterized by high heterogeneity between intra-tumor and inter-tumor at the cellular level, and histologically characterized by the dissimilar presence of subclonal and clonal differentiated tumor cell population, tumor stem cells, and components of the tumor microenvironment. These characteristics of the tissues that make up GBM lead to the failure of targeted therapy due to different susceptibility to therapeutic agents [78]. Therefore, the development of more sophisticated and powerful treatments is one of the most pressing challenges. Herein, we introduce alternative GBM treatment strategies such as photothermal therapy (PTT) and photodynamic therapy (PDT) utilizing gold nanoparticles (AuNPs), and their potential for oral drug delivery platform featuring the most non-invasive drug administration route.
PTT IN GBM TREATMENT
PTT is based on the local application of high temperatures to tissues to induce irreversible cellular damage at the target site and is considered a promising strategy for cancer treatments [9]. It is a non-invasive treatment that requires local irradiation of the tumor using an external near-infrared (NIR) laser. Upon laser irradiation, the photothermal agent (PTA) harvests the light energy, converts, and releases it as heat [10]. Afterwards, temperature rises for a certain period of time causing protein denaturation, cellular membrane disruption, enzyme dysfunction, and mitochondrial corruption, leading to tumor cell death and coagulative necrosis [11]. The advantage of PTT as a cancer treatment is based on the fact that cancerous tissue is more sensitive to heat than normal tissue. This is probably due to their acidic interstitial environment, reduced heat dissipation capacity, and increased metabolic stress, allowing for maximum anti-tumor effects while limiting damage to surrounding healthy tissue [12]. In addition, when the focal tip of a heat generator is applied to the tumor site, it rises the temperature gradient and a lesion is divided into three distinct areas: 1) a central region with maximum temperature rise (over 50℃) that causes irreversible damage, 2) a peripheral region characterized by sub-lethal PTT (41℃–45℃), where cells undergo apoptosis or recover from injury, 3) as a non-affected zone (<37℃) exists, PTA does not cause hyperthermia in normal tissue if accurately localized to the tumor lesion.
PTT is regarded as a paradigm shifting strategy for the treatment of GBM by using heat to destroy tumors as a non-chemical treatment for disease. It possesses a number of advantages that circumvent the limitations of GBM heterogeneity, drug resistance mechanisms, and adverse effects on surrounding healthy tissues [9]. However, there are challenges to develop PTT nanoparticles (NPs), enabling effective PTT on GBM. Upon systemic administration, it must overcome the BBB and reach the GBM site at therapeutic concentrations, and the NIR irradiation must cross multiple barriers (scalp, skull, and normal brain tissue) to reach the tumor site without adverse effects.
PDT IN GBM TREATMENT
PDT involves photoactivation of photosensitizer (PS) that are selectively incorporated into tumor cells. NIR light irradiation initiate PS activation by energy transfer to excite molecular oxygen to a singlet state and converts it to a triplet state by the intersystem relaxation. In the singlet state, the energy is either converted to heat by internal conversion or emitted as fluorescence. In the triplet state, the energy produces the reactive oxygen species (ROS) required to induce cell death. The generated ROS rapidly react with macromolecules such as unsaturated fatty acids, proteins, and cholesterols. These reactions cause disruption on the membranes of intracellular organelles, such as lysosome, mitochondria, and the endoplasmic reticulum [13]. Thereby, it ultimately induces tumor apoptosis, necrosis, local ischemia (due to occlusion of tumor micro-vessels) as well as subsequent host immunological reactions [14]. Unlike radiotherapy and surgical resection, PDT can treat microinvasive region while protecting sensitive brain areas [15]. These advantages over current therapies may improve the efficacy of GBM in patient populations with low survival and high recurrence rates.
PRECLINICAL STUDIES WITH RECENT ADVANCES IN NP-MEDIATED PHOTOTHERAPY FOR THE TREATMENT OF GBM
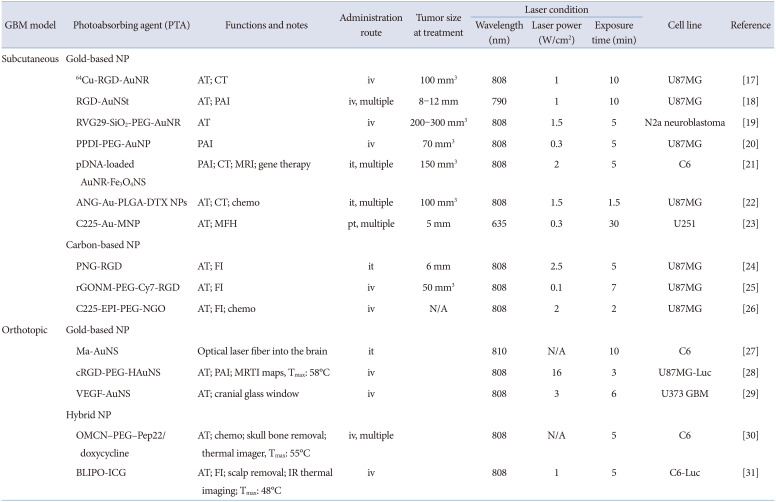
PTT and PDT are promising strategies for the treatment of GBM because they can destroy tumors as non-chemical treatments for diseases that circumvent the limitations of GBM heterogeneity, existing drug resistance mechanisms, and adverse effects on surrounding healthy tissues [16]. However, because they are hampered by the unique properties of the brain, strategies such as active targeting, multimodal imaging, or chemo/gene therapy must be developed to enhance the therapeutic efficacy of phototherapy on GBM. Therefore, to date, NPs with unique optical properties (e.g., Au-based or other semiconducting metal-based NPs, magnetic Fe3O4 NPs, carbon-based nanomaterials) or small photo-absorbable (PTA) molecules (e.g., cyanine or porphyrin derivatives) have been used for phototherapy (Table 1) [171819202122232425262728293031].
Since energy conversion and heat dissipation only occur when the frequency of the incident light overlaps the absorption band of the PTA agent, it should exhibit a strong NIR extinction coefficient. In fact, the NIR region corresponds to the transparent window of biological tissues, and light in this wavelength range (approximately 650–900 nm) can pass through soft tissues with minimal absorption, avoiding energy loss prior to irradiation with PTA preparations. In addition, NPs for phototherapy must be non-toxic without laser exposure and must have physicochemical properties (e.g., size, shape, zeta potential, and stability) to be administered systemically and to accumulate efficiently in the tumor, either passively or actively.
Given the complexity of GBM in most of the studies described above, targeted therapies have been developed that actively target tumor cells to bypass the BBB and achieve maximal NP tumor uptake. These strategies rely on grafting targeting ligands such as proteins, antibodies, and peptides on the NPs surface to selectively recognize overexpressed receptors in a specific cell population. Targeted drug delivery can bypass the blood-brain tumor barrier, the BBB, or directly access the tumor by specifically targeting brain capillary endothelial cells, tumor neovascular endothelial cells, and/or brain tumor cells. The most common targeting moieties for GBM are the transferrin (Tf), arginine-glycine-aspartic acid sequence (RGD), folic acid (FA), interleukin-13 (IL-13) peptides, and angiopep-2 peptide (ANG). Otherwise, local delivery strategies such as direct intracranial administration or convective-enhanced delivery can be used to bypass the BBB and enhance intracerebral NP concentrations by local delivery to the brain.
However, for phototherapy to treat brain tumors in clinical practice, three typical issues need to be resolved: 1) accumulation of PTA into tumors is restricted by the BBB, 2) monitoring the temperature rise and ROS generation inside the brain is not a simple task, it is essential to obtain safe and efficient photo-treatment, 3) local photoreactive responses, including heat dissipation and ROS generation, should be sufficient to achieve tumor cell death even when tumor localization is deep in the brain. How to develop and test systems to overcome these barriers is being continuously researched to achieve a clear vision for advancements in this field. The systems reported to date have not led to complete eradication of GBM due to the large number of invasive cells penetrating the peritumoral region and non-cancerous subpopulations residing within the tumor mass. However, we expect that selective targeting and efficient phototherapy can lead to partial resection of tumors. Moreover, the combination therapy such as PDT and PTT could potentially lead to enhanced anti-tumor consequences.
AuNPs FOR COMBINATIONAL PTT AND PDT IN GBM TREATMENT
Rapid growth of nanotechnology is an emerging tendency in cancer treatment. AuNPs have aroused interest in this field due to their unparalleled light-to-heat energy conversion and their capability to load and deliver numerous of PDT drugs to target site. Therefore, photothermal (PTT) and photodynamic (PDT) combined cancer treatment is possible by the role of AuNPs itself as a heat agonist and a drug carrier for PS transport. In the presence of AuNPs and PS drugs under photoactivating light wavelength, cytotoxic heat dissipation and ROS induces apoptotic and necrotic cancer cell death [32]. In terms of PTT, the collective oscillation of electrons on the AuNP surface causes surface plasmon resonance (SPR) in light of specific wavelength to generate a strong extinction coefficient, thereby dissipate sufficient heat [33]. In our study, the proximate conjugation of PS on AuNPs accelerated its PDT outcome [34]. The phenomenon that enhances the ability of PS to generate ROS was denoted as metal-enhanced ROS generation (MERos) and it is mediated by intersystem crossover between PS and AuNP. Therefore, heat generation from AuNPs by external light irradiation was sufficient, and the ROS generating ability of PS drugs was greatly increased by the role of nanoantennas of AuNPs, thereby the combination therapy of PTT and PDT was promising for GBM treatment.
A number of recent studies demonstrated nanotherapeutics that combine NIR wavelength-responsive PTA, PS drug achieve synergistic PTT, and PDT effects in tumor therapy [35363738]. Nonetheless, additional research is required to improve treatment protocols by regulating ROS generating capacity, laser power density, light irradiation dose, and improved tumor targeting effect to establish clinical feasibility.
ORAL SYSTEMIC ADMINISTRATION FOR THE TREATMENT OF PTT/PDT IN GBM
Oral drug administration is the preferred mode of drug delivery, primarily because of its simplicity. For daily medications, most patients prefer pills over injections. This arises from certain factors close related to patient compliance, including non-invasive and self-administering medications. In this regard, the large surface area (300–400 m2) of the gastrointestinal tract (GI) lined with a viscous mucosa provides an opportunity for long-term residence of the drug and promotes subsequent absorption [39]. In addition, endocrine cells, microfold cells (M cells), mucous secretary goblet cells, and Paneth cells that make up the GI tract may be promising targets for enhancing oral absorption of drugs [40]. However, the problems faced by oral drug delivery, such as low bioavailability and insufficient drug efficacy, remain unresolved. To this end, novel drug formulations have been developed that utilize NP drug delivery systems to overcome their respective limitations [41].
Nanopharmaceuticals being studied in oral drug delivery systems to date contain NPs (particles <100 nm) that are readily absorbed through the intestine and flow into the bloodstream. The typical oral drug delivery NPs include liposomes [424344], polymeric micelles [4546], drug-conjugated polymers [47], and noble metal NPs [48]. Orally delivered NPs are prepared to target specific region of the GI tract, such as duodenum, ileum, and jejunum, or to passively permeate NPs through the spaces between tight junctions at the epithelial barrier [49505152]. Nanopharmaceuticals have many advantages in oral drug delivery. They represent a large surface area, allowing them to interact with the GI tract and can be altered in a variety methods to overcome barriers in oral delivery. Through modifications in size, shape, and surface chemistry, the nanoscale drug delivery carriers described above have improved hydrophobicity, hydrophilicity, and oral bioavailability of biological agents, which can significantly affect cell transport [53].
CONCLUSION
In our study, AuNPs capable of dissipating high heat under light irradiation by SPR effect were used as PTT formulations. Furthermore, chlorin e6 (Ce6), a type of PDT PS, was bonded to the surface of AuNPs through disulfide bonds. As a result, AuNPs acted as nanoantennas, enhancing the ability of Ce6 to generate ROS. Moreover, AuNPs resolved the low water solubility of Ce6 as a carrier and achieved better tumor accumulation. The aim of this study was to develop a GBM-targeted PTT/PDT through oral administration. Therefore, lactoferrin (Lf) was conjugated to the AuNPs surface to improve the low bioavailability and GBM targeting of AuNPs. Lactoferrin is generally delivered orally and is known to be absorbed by interaction with the lactoferrin receptor (LfR) expressed in intestinal endothelial cells, BBB, and GBM. Receptor-mediated endocytosis occurred by utilizing lactoferrin as a ligand to enhance oral absorption in the GI tract and targeting GBM. Additionally, the nanoscale (10–20 nm) of our AuNP-based platforme allowed passive transport into the BBB by the enhanced permeability and retention effect, which are commonly caused by abnormal vascularization and tumor pressure in the GBM microenvironment. As a result, the developed PTT/PDT formulation enabled effective GBM anticancer treatment by irradiating NIR wavelength to generate high-efficiency heat and ROS. Furthermore, oral absorption and GBM targeting were enhanced by lactoferrin. Therefore, our study demonstrates great significance in that it developed an eating-type photothermal/photodynamic brain tumor treatment technology platform and opened up the possibility of application to the development of brain tumor therapeutics by loading other anti cancer drugs in the future.
 XML Download
XML Download