

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chordoma is a rare primary bone tumor, which develops from intraosseous notochordal remnants along the neuroaxis [1]. Therefore, it commonly occurs at the sacrococcygeal region (50%) or base of the skull (35%) and rarely occurs at the mobile spine (15%) or the lumbar spine (6%) [23]. As a primary bone tumor in the spine is very rare, chordoma could be one of the most frequent primary tumors of the mobile spine [3]. Thus, a chordoma should be one of differential diagnoses for destructing vertebral body tumors.
En bloc excision of the chordoma is recommended to cure or obtain long-term progression-free survival [4]. However, en bloc margin-free excisions are not appropriate for all skull base or mobile spinal segment chordomas [3]. Thus, local recurrence of chordoma is very common following intralesional or margin-involved excisions. Not only from the initial presentation but also in recurrence, chordoma, a tumor known-to-be from an extradural origin, frequently invades into the intradural space [56]. Additionally, surgical spillage or seeding along the wound has been reported [78]. In addition to typical local recurrences, 30%–40% of recurrent patients experience tumor metastasis to the lungs, liver, bones, or lymph nodes [191011].
In our L3 chordoma case, which later progressed to distant metastasis of the fascia lata and intradural extramedullary (IDEM) lesion, discussion about the prevalence of mobile segment spine chordoma progress to local invasion as an IDEM mass and distant metastasis over several years would be worthwhile.
CASE REPORT
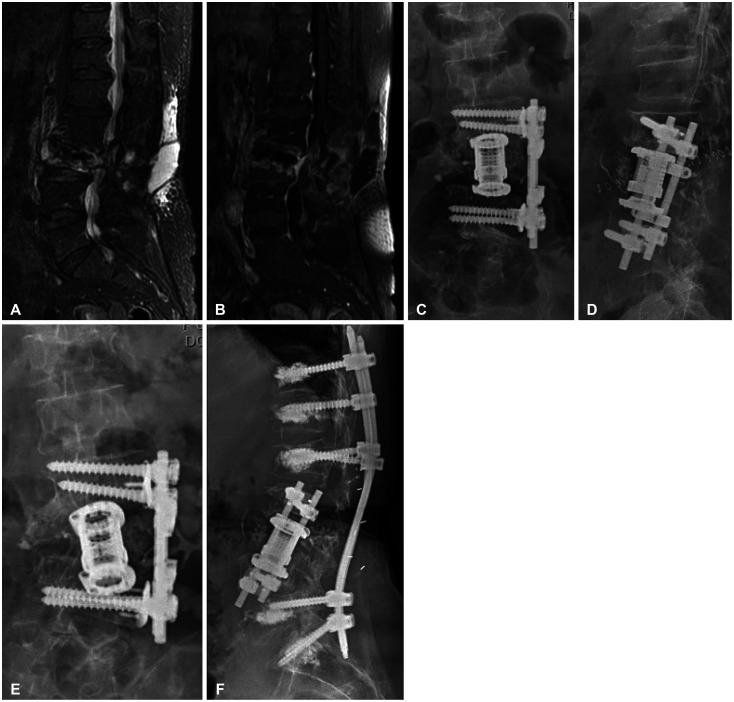
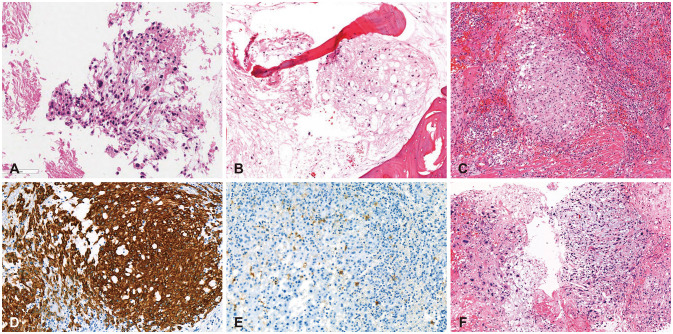
A 64-year old female patient visited our center for a second opinion and further evaluation of a L3 solitary mass. Her past medical history revealed that she had presented to the university hospital with lower back pain after a fall-down injury. Based on the medical record of that hospital, MRI revealed a destructive mass involving the L3 vertebral body with low signal intensity on a T1-weighted image and a mixed signal on a T2-weighted image with gadolinium enhancement, suggesting a metastatic lesion (Fig. 1A-C). Because positron emission tomography and computed tomography (PET-CT) showed no other abnormal hypermetabolic lesions, except hot uptake of the L3 vertebral body (Fig. 1D and E), the attending physician decided to perform an open biopsy in the Department of Neurosurgery. They performed a hemilaminectomy including a partial excision of the mass and vertebroplasty with bone cement. Under the diagnosis of ‘malignancy of unknown origin,’ radiation was given to the involved field around the L3 body (6,600 cGy/24 fractions). During the course of radiation therapy, she suffered from headache and wound fluctuation. MRI at that time revealed cerebrospinal fluid (CSF) leakage with a residual tumor (Fig. 2A and B). She received wound revision and lumbar drainage, then finished radiation therapy. After she came to visit our outpatient clinic 3 months after the first excisional biopsy, pathological review of the outside open-biopsy slide revealed a malignant tumor with epithelioid cell morphology and myxoid stroma, suggestive of chordoma (Fig. 3A). Wholebody PET was taken 6 months from the radiation therapy to investigate the tumor extent and viability, and it revealed hypermetabolic lesion in the L3 vertebral body with bony destruction, otherwise, no abnormal hypermetabolic lesion in the imaged body. After discussion in multi-disciplinary tumor board, surgical extirpation of irradiated chordoma and interbody fusion was recommended via lateral approach. However, her osteoporosis was so poor (T-score of -4.6) that we could not adopt the fusion at that time. We prescribed a weekly bone absorption inhibitor and as much as possible of bed rest to correct her osteoporosis before conducting the planned surgical intervention to relieve her lower back pain. However, she was admitted to our hospital due to low back and pelvic pain after a fall-down injury at home one year after radiation therapy. Medical and radiological examination verified progression of the L3 compression due to the chordoma and a pelvic bone fracture. Although her osteoporosis was not corrected to an acceptable level, we planned the L3 corpectomy with instrumentation. Although en bloc excision was not possible due to adhesion from the previous operation and radiation, we completely removed L3 vertebral body with clear resection margin and the lateral fusion with cage was successful (Fig. 2C and D). Biopsy specimens were reviewed as a chordoma, post-radiation therapy status (Fig. 3B). However, as soon as she tried ambulation for toileting at postoperative one week, the fusion was collapsed (Fig. 2E). Upon the decision of failed back syndrome, we additionally performed T12, L1-L5, and S1 percutaneous posterior fixation with intraoperative bone cement application to prevent the screw slippage (Fig. 2F).
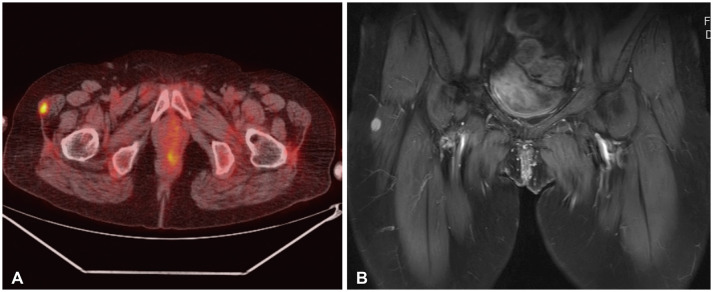
After the second operation, patient underwent several major and minor surgeries due to wound dehiscence. One year after the second operation, PET-CT revealed a round hypermetabolic lesion on the right tensor fascia lata (Fig. 4A). After consulting an orthopedic surgeon and conducting an MRI (Fig. 4B), an excisional biopsy was done widely with a proper free margin. Pathologic examination with immunohistochemical staining positive for cytokeratin and negative for S-100 protein (Fig. 3C-E) confirmed metastatic chordoma. One and a half years after the L3 corpectomy (almost 3 years after the first excisional biopsy and CSF leakage repair at other hospital), she complained of worsening radiating pain at the L2 dermatome. On routine PET-CT, hyperuptake was found in the spinal canal at the L2-3 level (Fig. 5A). To confirm this hot uptake to be an intraspinal lesion, we performed CT myelogram (MRI was not readable due to metallic artefact of previous fusion material), and it revealed a block of injected dye at the L2–L3 level, suggesting intraspinal mass lesion (Fig. 5B). As we did not bleach any CSF pathways/dura mater during the L3 corpectomy, posterior fusion and wound revisions, we assumed that this spinal drop metastasis might came from the initial operation of excisional biopsy and CSF leakage repair at other hospital. A L2 laminectomy was performed, and after dural incision, a pure IDEM mass without any connection to paravertebral structure was seen and excised completely. As we did not violate dura mater at the L3 corpectomy, we assumed that this drop metastasis could occur at the 1st excisional biopsy and CSF leakage repair procedure at the other hospital. After pathologic confirmation of chordoma with high grade features (Fig. 3F), we evaluated CSF cytology for the possibility of leptomeningeal metastasis, but leptomeningeal spread did not occur for a year either on serial cytology follow-up or on clinical examination.
The patient was treated for a L2 paravertebral recurrence using surgical excision and stereotactic spinal radiosurgery (Cyberknife, Accuray, Sunnyvale, CA, USA) two years later. The patient is currently bed-ridden and under supportive care due to radiation-induced radiculopathy with an intrathecal drug infusion pump and epidural electric stimulator. Recently, on routine PET-CT, increased size and metabolisms of both inguinal, external iliac, para-aortic lymph nodes and lung nodules were found and were suspected of metastasis radiologically. However, conducted sonography-guided gun biopsy was not sufficient to make a confirmative diagnosis due to the small amount of atypical cells. Ongoing follow-up is advised for the screening of additional metastasis for this patient.
DISCUSSION
Incidence and clinical features of mid vertebral segment chordoma
A chordoma originates from a notochord remnant; thus, the cephalic and caudal end of the spine is the usual location. The tumor presents mostly at the spheno-occipital or sacral region. However, up to 15% of chordomas occur in the mid vertebral segment [1012]. As the primary bone tumor is very rare, chordoma could be the most frequent among primary tumors of the mobile spine [3]. Thus, it is recommended to include chordoma as one of the differential diagnoses for tumors involving the mobile spine segment.
Boriani et al. [3] reported a consecutive series of 52 chordomas of the mobile spine. Interestingly, L3 (as in our case) was the most frequent location (10/52 cases), followed by C2 and L2 (9 cases each). This study suggested margin-free en
bloc resection of the involved spinal segment was preferred to an intralesional excision in order to achieve long-term progression-free survival. However, only 18 out of 48 (38%) patients were able to undergo an en bloc resection. Additionally, 100% of all patients (n=6) who showed recurrence after en
bloc excision had contaminated margins after excision.
Zou et al. [12] analyzed prognostic factors in spinal chordoma via a systematic review using 8 out of 65 available papers from MEDLINE and Embase. They suggested upper cervical location, worse preoperative Frankel score, intralesional surgery, greater extent of invasion, and revision surgery were independent factors associated with poor clinical outcomes. In our case, the first operation was intralesional biopsy, followed by local radiation therapy under the impression of malignancy of unknown origin, and the tumor recurred 1.5 years later, presenting as progression of L3 vertebral body destruction causing patient’s immobilization. The second operation was a L3 corpectomy with cage and plate reconstruction in a not en
bloc but piecemeal resection, which resulted in paravertebral recurrence.
Recurrence pattern of chordoma
As en bloc excision of chordoma is frequently not feasible, local recurrence is quite common following intralesional excision. Surgical spillage or seeding along the wound has been reported [8]. Metastases of chordoma to other organs, including lung, skin, brain, and contiguous spine, are rare but have been reported [2791113]. In our case, the description of pathologist about histologic grade were not changed from the in situ tumor to recurrent/metastatic tumors. Several studies tried to characterize the molecular biology of chordoma, and searched for biological markers such as microRNA, aberrant proteins/gene expression. However, the results were negative or remain controversial [12].
Chordoma is usually an extradural tumor, but intradural invasion of primary chordoma has been reported either as primary or recurrent chordoma [56714]. Surgical seeding of chordomas was analyzed in a single institution series by Arnautović and Al-Mefty [8]. Six out of 82 consecutive chordomas showed surgical seeding along the operative route, and the mean time to diagnosis ranged from 5–15 months after surgery.
Distant metastasis of a clival chordoma to the thoracic spine five years later was reported by Aydin et al. [11]. However, they did not have a baseline whole spine MRI evaluation at the first surgery for the clival chordoma. Additionally, the patient had another metastatic lesion at the C1–C2 extradural space. As there have been reports of epidural chordoma without bony involvement (extraosseous) or intradural chordoma at the presentation [61415], it is unclear whether a metastatic chordoma without bony involvement is purely metastatic or a contagious local progression invading dura mater. Steenberghs et al. [14] reported a similar case to the present study, in that the chordoma presented with IDEM extension, which resulted in multiple spinal drop metastases and metastasis to paravertebral muscles over time. Unlike our case, the case presented by Steenberghs et al. [14] included multiple chordomas at presentation. In our current study, it is unclear whether the IDEM chordomas were primarily intradural invasion or surgical seeding after the first excisional biopsy. As her past medical history revealed CSF leakage after the first excisional biopsy during adjuvant radiation, and considering the time interval between the operation and seeding, the IDEM chordoma was most likely seeded at the first operation.


 XML Download
XML Download