

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Glioblastoma (GBM) is the most common malignant primary brain tumor, accounting for nearly half of all adult primary brain cancer cases [1]. Unfortunately, the median survival (MS) of patients diagnosed with GBM is less than one year, while the 5-year overall survival (OS) rate is approximately 5%–10% [1]. Characteristically, there is a detrimental correlation between increasing age and survival in GBM, even though half of the affected patients are aged >65 years [12345]. Furthermore, patients aged >70 years were not eligible for the landmark trial by Stupp et al. [6], which excluded elderly patients from possibly attaining the reported OS benefit of temozolomide (TMZ) in combination with radiotherapy (RT).
There are several inherent challenges regarding the treatment of elderly patients with GBM (GBM-e). Although GBM-e are fit enough to undergo standard TMZ-based radiochemotherapy, they do not do well as younger patients, with an MS of 9–14 months, and 16 months at most for highly selected patients [789101112]. Furthermore, older patients often present with worse performance status and multiple comorbidities than their younger counterparts. They are also vulnerable to treatment-related toxicities due to the fragility of aged brain tissues, which is very difficult to accurately evaluate before initiating treatment [1314] and may ultimately lead to undertreatment of elderly patients, resulting in suboptimal outcomes [1516]. Using the National Cancer Database (2004–2016), Nunna et al. [15] reported that there is twice the chance for GBM-e aged ≥65 years of not receiving surgery, RT, or chemotherapy. However, RT significantly prolonged OS in these elderly patients, even if they had a poor performance status or did not undergo surgical resection [15]. Finally, defining the cut-off age for ‘elderly’ individuals is a complicated process, as the life expectancy of individuals has increased over time [17].
In this review, current evidence regarding RT for GBM-e is summarized based on published literature. Furthermore, important issues that need to be addressed are also highlighted.
PROGNOSTIC FACTORS IN ELDERLY PATIENTS WITH NEWLY DIAGNOSED GBM
One of the major steps in treating patients with cancer is the precise measurement of expected prognosis and balancing the risk-to-benefit ratio of certain treatments, especially in patients who are expected to demonstrate limited survival, which is the case with GBM-e.
The reported prognostic factors for GBM-e did not differ from those reported for younger patients. The extent of resection stands as a major prognostic factor for GBM-e [1218192021]. Supratotal (hazard ratio [HR] 0.65; p<0.0001) and gross total resection (HR 0.61; p<0.0001) were shown to significantly lower the risk of death in GBM-e aged ≥65 years compared to biopsy or local excision, which was a consistent finding across all age groups, except for GBM-e aged ≥90 years, based on data from the Surveillance, Epidemiology, and End Results Program [18]. In a recent meta-analysis involving 13 retrospective studies, gross total resection significantly improved OS in GBM-e compared with subtotal resection (HR 0.70; p<0.001) [19]. Performance status also significantly affected OS in newly diagnosed GBM-e, as in younger patients [41221]. Methylation of the O6-methylguanine-DNA methyltransferase (MGMT) promoter is a favorable prognostic factor that particularly predicts response to TMZ in GBM-e treated by either TMZ or TMZ-based radiochemotherapy [122223242526], as reported by secondary analyses of randomized trials and retrospective series. In contrast, promoter methylation of the MGMT gene (MGMT+) does not appear to impact OS in GBM-e treated by RT alone [222324]. The presence of lymphopenia has also recently become identified as an unfavorable prognostic factor [2126].
It should be borne in mind that patients who have good prognostic factors and are expected to survive longer are not necessarily also those who would benefit from certain treatments. Although more aggressive and intense treatments may be considered for these patients, whether a specific subgroup benefits from the treatment is a different issue.
BIOLOGICAL ASPECTS OF STANDARD RADIOTHERAPY DOSE FOR PATIENTS WITH GBM
Estimation of the biologically effective dose (BED) of RT in tumor cells and normal tissue is based on the intrinsic radiosensitivity of the target tumor cells, which is briefly summarized as the ‘α/β ratio (Gy)’ according to a linear-quadratic dose-response model, in radiobiology [27]. The BED for GBM is calculated as follows: total dose × [1 + daily dose/(α/β ratio)]. GBM cells are estimated to have an α/β ratio of 8 Gy (range, 5.0–10.8 Gy) [28], which is higher than that of the normal tissues within the central nervous system (2 Gy). A BED of 60 Gy in 30 fractions and 40.05 Gy in 15 fractions was calculated as 75 Gy and 53.42 Gy using an α/β ratio of 8 Gy. Therefore, theoretically, the former RT regimen would result in superior GBM cell killing and tumor control. However, the BED in normal brain tissue was higher in the former regimen (120 Gy vs. 93.52 Gy). Theoretically, this would increase the risk of complications, such as radionecrosis or brain edema, especially in elderly patients with more fragile brain tissues.
For several decades, the optimal radiotherapy dose for high-grade gliomas has been established by two major studies [2930]. The Brain Tumor Study Group pooled 621 patients with malignant glioma from their protocols between 1966 and 1975 and reported a dose-survival relationship favoring 60 Gy over lower dose schemes or no RT [29]. Compared to no RT, ≤45 Gy and 50 Gy, patients treated with 60 Gy (6 weeks) demonstrated a significant absolute MS benefit of 24 weeks (p=0.001), 28.5 weeks (p=0.001), and 14 weeks (p=0.004), respectively. The Medical Research Council Brain Tumour Working Party performed a prospective randomized trial comparing 60 Gy in 6 weeks vs. 45 Gy in 4 weeks following surgery in grade 3–4 astrocytomas [30]. One-third of 474 patients were aged ≥60 years. Compared with patients treated with a lower dose of 45 Gy, an absolute survival benefit of 2 months was observed in patients treated with 60 Gy (p=0.04). Significant survival benefit of a higher RT dose was maintained even in patients with the poorest prognostic indicators, based on age, performance, extent of surgery, and history of fits [30]. Taken together, a standard RT dose of 60 Gy in 6 weeks has been established for high-grade gliomas and this has not changed for several decades [5631323334].
RADIOTHERAPY ALONE FOLLOWING SURGERY IN ELDERLY PATIENTS WITH GBM
Major prospective randomized trials investigating RT alone are summarized in Table 1. The pivotal role of RT in GBM-e aged ≥70 years was defined in a prospective randomized study by Keime-Guibert et al. [35] from the Association des Neuro-OnCologues d’Expression Francaise. A conventionally fractionated RT (CFRT) regimen of 50 Gy (1.8 Gy per fraction) demonstrated an absolute MS benefit of 3 months compared with best supportive care (29 weeks vs. 17 weeks; p=0.002; HR for death, 0.47) following surgery in GBM-e. In this study, progression-free survival was also significantly prolonged in the RT arm, whereas performance status, health-related quality of life, and neurocognition did not differ significantly between the two arms.
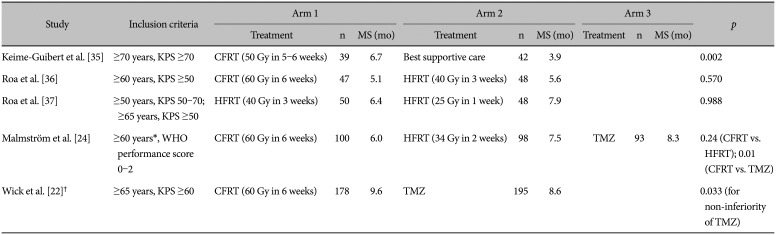
Table 1
Prospective randomized trials assessing radiotherapy alone in elderly patients with newly diagnosed glioblastoma
| Study | Inclusion criteria | Arm 1 | Arm 2 | Arm 3 | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment | n | MS (mo) | Treatment | n | MS (mo) | Treatment | n | MS (mo) | |||
| Keime-Guibert et al. [35] | ≥70 years, KPS ≥70 | CFRT (50 Gy in 5–6 weeks) | 39 | 6.7 | Best supportive care | 42 | 3.9 | 0.002 | |||
| Roa et al. [36] | ≥60 years, KPS ≥50 | CFRT (60 Gy in 6 weeks) | 47 | 5.1 | HFRT (40 Gy in 3 weeks) | 48 | 5.6 | 0.570 | |||
| Roa et al. [37] | ≥50 years, KPS 50–70; ≥65 years, KPS ≥50 | HFRT (40 Gy in 3 weeks) | 50 | 6.4 | HFRT (25 Gy in 1 week) | 48 | 7.9 | 0.988 | |||
| Malmström et al. [24] | ≥60 years*, WHO performance score 0–2 | CFRT (60 Gy in 6 weeks) | 100 | 6.0 | HFRT (34 Gy in 2 weeks) | 98 | 7.5 | TMZ | 93 | 8.3 | 0.24 (CFRT vs. HFRT); 0.01 (CFRT vs. TMZ) |
| Wick et al. [22]† | ≥65 years, KPS ≥60 | CFRT (60 Gy in 6 weeks) | 178 | 9.6 | TMZ | 195 | 8.6 | 0.033 (for non-inferiority of TMZ) | |||
![]()
Despite the significantly prolonged survival with RT, the necessity of an inconvenient and potentially morbid RT schedule of 6 weeks (60 Gy) has been questioned regarding its use in GBM-e since most GBM-e patients show very poor survival. Subsequently, efforts have been made to abbreviate the RT schedule in GBM-e. Roa et al. [36] prospectively compared a CFRT regimen of 60 Gy over 6 weeks with a hypofractionated RT (HFRT) schedule of 40 Gy in 15 fractions over 3 weeks in GBM-e aged ≥60 years. The median Karnofsky Performance Scale score was 70. In this trial, involving 50 patients in each arm, there was no difference in survival between the 60 Gy and 40 Gy groups (MS, 5.1 months vs. 5.6 months; p=0.57). However, the proportion of patients requiring an increased dosage of post-RT corticosteroids was doubled in the CFRT arm compared to the HFRT arm (49% vs. 23%; p=0.02) [36]. The Nordic Clinical Brain Tumour Study Group also performed a 3-arm prospective randomized trial comparing CFRT (60 Gy in 30 fractions) vs. HFRT (34 Gy in 10 fractions) vs. six cycles of TMZ alone in fairly performing GBM-e aged ≥60 years [24]. In this study, there was no difference in MS between GBM-e treated with 60 Gy and 34 Gy (p=0.24). Notably, 34 Gy provided a longer MS than 60 Gy for patients aged ≥70 years (MS, 7.0 months vs. 5.2 months, p=0.02). Furthermore, GBM-e patients treated with 6 cycles of TMZ alone demonstrated significantly prolonged survival compared to CFRT of 60 Gy (MS, 8.3 months vs. 6.0 months, p=0.01), although this survival benefit was limited in MGMT+ patients [24].
Roa et al. [37] further abbreviated the RT schedule for elderly or frail GBM patients and compared two HFRT regimens of 40 Gy in 15 fractions over 3 weeks and 25 Gy in five fractions over 1 week in a trial by the International Atomic Energy Agency. Patients were eligible for this trial if they met either of the following criteria: 1) ≥50 years old with a KPS of 50–70 or 2) ≥65 years old with a KPS of 50–100. Once again, there was no difference in MS between the two arms with an MS of 6.4 months and 7.9 months for patients treated with 40 Gy and 25 Gy, respectively (p=0.988). Global health-related quality of life at 4 and 8 weeks post-RT was also similar between the two arms [37].
In the German NOA-08 trial for malignant astrocytomas, where approximately 90% were GBMs, Wick et al [22]. compared CFRT of 60 Gy over 6 weeks to TMZ alone following surgery in patients aged ≥65 years with KPS ≥60. There is no difference in survival between both arms, with an MS of 9.6 months and 8.6 months for CFRT and TMZ (pnon-inferiority=0.033), respectively, indicating non-inferiority of TMZ alone. The median event-free survival likewise did not differ between both arms. MGMT promoter methylation is an indicator of the expected response to treatment. After a long-term follow-up of 7.5 years, MGMT+ patients treated with TMZ alone demonstrated the best MS (18.4 months) followed by MGMT+/MGMT-treated with CFRT (MS, 9.6/10.2 months), and then by MGMT-treated with TMZ (MS, 6.7 months) [23].
Taken together (Table 1), RT significantly improved MS in fairly performing GBM-e compared to best supportive care [34], and HFRT provided comparable outcomes to CFRT of 60 Gy when treated by RT alone [243536], with higher convenience. When delivering HFRT, there is a consensus among experts that 40 Gy in 15 fractions over 3 weeks might be a better option because there is limited experience with the regimen of 25 Gy in five fractions in general, and the regimen would be more appropriate for relatively small tumors [38]. Furthermore, physicians should keep in mind that in GBM-e MGMT+ patients treated by adjuvant monotherapy following surgery TMZ alone is a reasonable option [2223] (Table 1).
TEMOZOLOMIDE-BASED RADIOCHEMOTHERAPY IN ELDERLY PATIENTS: PROSPECTIVE EVIDENCE
Since the landmark trial published in 2005 by Stupp et al. [6], CFRT of 60 Gy plus concurrent and adjuvant TMZ (CFRT/TMZ→TMZ) has been the standard treatment for GBM patients aged <70 years, with a WHO performance status of 0–2. Although the overall survival benefit of TMZ was originally reported to be limited in MGMT+ patients [39], long-term follow-up revealed a significantly higher number of long-term survivors when TMZ was added to CFRT in MGMT- patients [40]. TMZ not only affects GBM tumor cell survival by itself but also functions as a well-acknowledged radiosensitizer by inhibiting RT-induced DNA double-strand break repair, eventually leading to increased mitotic catastrophe [41]. MGMT+ patients aged <70 years can also benefit further with the addition of lomustine to RT/TMZ→TMZ [42].
Continuous efforts to combine TMZ with various RT regimens for the treatment of GBM-e have been undertaken since 2005 (Table 2). Several prospective single-arm studies have reported superior MS results with RT/TMZ→TMZ in GBM-e [78910] compared to the aforementioned prospective studies evaluating RT alone [2224353637]. Minniti et al. [7] and Brandes et al. [8] have reported an MS of 10.6–13.7 months in GBM-e aged over 65–70 years treated with CFRT/TMZ→TMZ using 60 Gy in 30 fractions. Although neurotoxicity and mental status deterioration, which was mostly stabilized with steroids, were observed in a significant proportion of patients and direct comparison may not be appropriate, this CFRT/TMZ→TMZ regimen prolonged MS by 5–7 months compared to studies of RT alone [24353637]. Minniti et al. [910] also reported an MS of 9.3–12.4 months in GBM-e treated with HFRT/TMZ→TMZ using HFRT regimens of 30 Gy in six fractions and 40 Gy in three fractions in subsequent prospective single-arm studies.
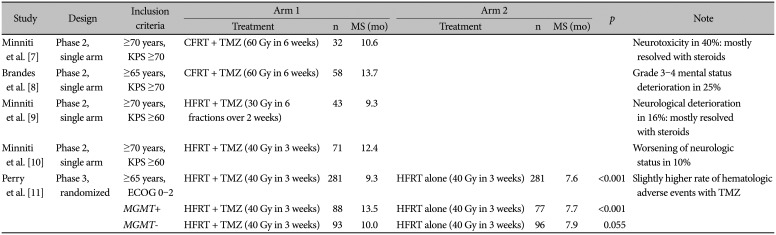
Table 2
Prospective trials assessing radiotherapy combined with TMZ in elderly patients with newly diagnosed glioblastoma
| Study | Design | Inclusion criteria | Arm 1 | Arm 2 | p | Note | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Treatment | n | MS (mo) | Treatment | n | MS (mo) | |||||
| Minniti et al. [7] | Phase 2, single arm | ≥70 years, KPS ≥70 | CFRT + TMZ (60 Gy in 6 weeks) | 32 | 10.6 | Neurotoxicity in 40%: mostly resolved with steroids | ||||
| Brandes et al. [8] | Phase 2, single arm | ≥65 years, KPS ≥70 | CFRT + TMZ (60 Gy in 6 weeks) | 58 | 13.7 | Grade 3–4 mental status deterioration in 25% | ||||
| Minniti et al. [9] | Phase 2, single arm | ≥70 years, KPS ≥60 | HFRT + TMZ (30 Gy in 6 fractions over 2 weeks) | 43 | 9.3 | Neurological deterioration in 16%: mostly resolved with steroids | ||||
| Minniti et al. [10] | Phase 2, single arm | ≥70 years, KPS ≥60 | HFRT + TMZ (40 Gy in 3 weeks) | 71 | 12.4 | Worsening of neurologic status in 10% | ||||
| Perry et al. [11] | Phase 3, randomized | ≥65 years, ECOG 0–2 | HFRT + TMZ (40 Gy in 3 weeks) | 281 | 9.3 | HFRT alone (40 Gy in 3 weeks) | 281 | 7.6 | <0.001 | Slightly higher rate of hematologic adverse events with TMZ |
| MGMT+ | HFRT + TMZ (40 Gy in 3 weeks) | 88 | 13.5 | HFRT alone (40 Gy in 3 weeks) | 77 | 7.7 | <0.001 | |||
| MGMT- | HFRT + TMZ (40 Gy in 3 weeks) | 93 | 10.0 | HFRT alone (40 Gy in 3 weeks) | 96 | 7.9 | 0.055 | |||
![]()
Perry et al. [11] confirmed the survival benefit of TMZ combined with HFRT for GBM-e in a phase 3 prospective randomized trial. A total of 562 patients aged ≥65 years with a WHO performance status of 0–2 were randomized to either HFRT/TMZ followed by 12 cycles of TMZ or HFRT alone, using 40 Gy in 15 fractions over 3 weeks as the HFRT regimen. MS was significantly improved from 7.6 months to 9.3 months with the addition of TMZ (p<0.001), although a slightly higher rate of hematologic adverse events was observed in the TMZ arm. Median progression-free survival was significantly improved in the HFRT/TMZ→TMZ arm from 3.9 months to 5.3 months (p<0.001). As in younger patients [39], the benefit of adding TMZ was pronounced in MGMT+ GBM-e, with an absolute MS benefit of 6 months (7.7→13.5 months; p<0.001) [11]. Notably, although statistical significance was not reached, MGMT- GBM-e also demonstrated a modest but clinically meaningful MS improvement of 2 months with TMZ (7.9→10.0 months, p=0.055). Of note, the eligibility criteria of this trial stated that only patients‘who were deemed by their physicians not to be suitable to receive CFRT (60 Gy in 30 fractions over 6 weeks) in combination with TMZ’ were eligible. To date, there is no gold standard for deciding which RT regimen (CFRT vs. HFRT) would be appropriate in GBM-e patients with a WHO performance score of 0–2, and this is an issue that needs to be addressed urgently.
A small subgroup analysis (n=42) of GBM-e patients aged ≥70 years from the Project of Emilia-Romagna Region in Neuro-Oncology (PERNO) reported a survival benefit of TMZ limited to MGMT+ patients when added to RT [43]. Notably, RT regimens varied among patients. In MGMT+ patients (n=17), the MS was 17.2 months and 8.8 months in the RT plus TMZ and RT alone groups, respectively. In contrast, for MGMT- patients (n=25), the MS for RT plus TMZ and RT alone groups were 8.5 months and 8.0 months, respectively [43]. Therefore, one can argue that, in GBM-e, TMZ should be used only for MGMT+ patients when combined with RT.
One randomized phase 3 trial is ongoing in Japan to confirm the non-inferiority of 25 Gy in five fractions compared to 40 Gy in 15 fractions in the context of RT/TMZ→TMZ for GBM-e aged ≥70 years [44]. A total of 270 patients with ECOG performance status of 0–3 are planned for accrual. Conversely, the Korean Radiation Oncology Group recently approved a multi-institutional phase 3 prospective randomized trial (unpublished; KROG 21-11, http://www.krog.or.kr/ing/bbs/board.php?bo_table=protocols&sca) comparing 60 Gy in 30 fractions to 40 Gy in 15 fractions in GBM-e aged ≥70 years with a fair performance status of KPS ≥60. The stratification factors will include institution, performance status, methylation profile of the MGMT gene promoter, extent of surgical resection, and the G-8 geriatric screening score. As the results of this trial will not be available for several years, the choice of RT regimen combined with TMZ in GBM-e should mostly rely on retrospective evidence and the radiation oncologist’s intuition.
TEMOZOLOMIDE-BASED RADIOCHEMOTHERAPY IN ELDERLY PATIENTS: RETROSPECTIVE EVIDENCE
What is the most adequate RT dose fractionation for GBM-e that is deemed suitable for TMZ-based radiochemotherapy? Would an abbreviated course of HFRT fit all patients treated with TMZ? Several small-to large-scale retrospective studies have attempted to answer these questions [1245464748].
A small retrospective series from Dana-Farber/Brigham and Women’s Cancer Center compared HFRT (n=34; 40 Gy in 15 fractions) and CFRT (n=57; 59.4 Gy in 33 fractions or 60 Gy in 30 fractions) in the setting of TMZ in GBM-e aged ≥65 years [45]. No difference in survival was observed with or without propensity score matching, although MS was slightly longer with CFRT plus TMZ (11.1 months vs. 9.6 months). In Italy, Navarria et al. [46] compared GBM-e patients aged 65–69 years who were treated with 60 Gy in 30 fractions with those aged ≥70 years who were treated with 40.5 Gy in 15 fractions. All the patients were treated with concurrent and adjuvant TMZ therapy. After propensity score matching, the MS for the 65- to 69-year group (n=86) and ≥70-year group (n=86) were 14 months and 12 months, respectively, without a statistical difference (p=0.357). Based on these results, the authors suggested that HFRT combined with TMZ should be considered even in younger elderly patients with GBM [46].
In contrast, Gzell et al. [47] reported a significant survival benefit of CFRT (60 Gy) over HFRT (40 Gy) in 48 GBM-e patients aged 65–75 years who were treated with RT combined with concurrent TMZ, concurrent plus adjuvant TMZ, or adjuvant TMZ (Table 3). The MS for patients receiving 40 Gy and 60 Gy were 11 and 15 months (p<0.0001), respectively. Using the National Cancer Database, Mak et al. [48] have also reported a significant MS benefit in GBM-e patients aged ≥70 years when treated with CFRT (58–63 Gy in 1.8–2.0 Gy fractions) compared to HFRT (34–42 Gy in 2.5–3.4 Gy fractions). Notably, although there is no high-level evidence supporting the superiority of CFRT over HFRT in GBM-e to date, 93.4% of the 4,598 patients received CFRT. With a median follow-up of 21.0 months for survivors, the MS for CFRT and HFRT were 8.9 months and 4.9 months (p<0.0001), respectively. Significance was confirmed using multivariate analysis. Furthermore, in patients (76.9%) who were treated with RT plus chemotherapy, the survival benefit of CFRT compared to HFRT was persistent (MS, 9.7 months vs. 5.6 months; p<0.0001) [48].
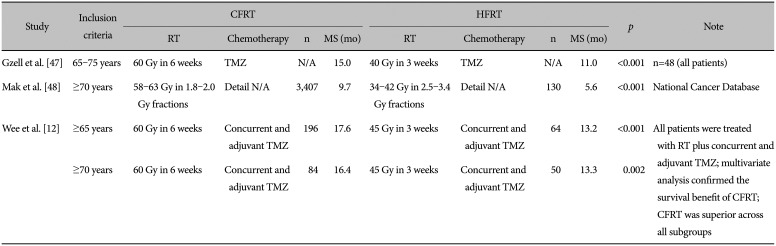
Table 3
Selected retrospective studies demonstrating the benefit of conventionally fractionated radiotherapy compared to hypofractionated radiotherapy when combined with chemotherapy
| Study | Inclusion criteria | CFRT | HFRT | p | Note | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| RT | Chemotherapy | n | MS (mo) | RT | Chemotherapy | n | MS (mo) | ||||
| Gzell et al. [47] | 65–75 years | 60 Gy in 6 weeks | TMZ | N/A | 15.0 | 40 Gy in 3 weeks | TMZ | N/A | 11.0 | <0.001 | n=48 (all patients) |
| Mak et al. [48] | ≥70 years | 58–63 Gy in 1.8–2.0 Gy fractions | Detail N/A | 3,407 | 9.7 | 34–42 Gy in 2.5–3.4 Gy fractions | Detail N/A | 130 | 5.6 | <0.001 | National Cancer Database |
| Wee et al. [12] | ≥65 years | 60 Gy in 6 weeks | Concurrent and adjuvant TMZ | 196 | 17.6 | 45 Gy in 3 weeks | Concurrent and adjuvant TMZ | 64 | 13.2 | <0.001 | All patients were treated with RT plus concurrent and adjuvant TMZ; multivariate analysis confirmed the survival benefit of CFRT; CFRT was superior across all subgroups |
| ≥70 years | 60 Gy in 6 weeks | Concurrent and adjuvant TMZ | 84 | 16.4 | 45 Gy in 3 weeks | Concurrent and adjuvant TMZ | 50 | 13.3 | 0.002 | ||
![]()
To the best of our knowledge, the largest retrospective study comparing CFRT and HFRT in GBM-e patients who were treated with RT/TMZ→TMZ was reported by Wee et al. [12] from Korea (Table 3). This multi-institutional study included 260 and 134 GBM-e patients aged ≥65 years and ≥70 years, respectively, with known promoter methylation profiles of the MGMT gene. The median RT dose was 60 Gy in 30 fractions (interquartile range, 60–61.2 Gy) and 45 Gy in 15 fractions (interquartile range, 42.5–45 Gy) in the CFRT and HFRT groups, respectively. Compared to HFRT, CFRT significantly improved the MS from 13.2 months to 17.6 months in patients aged ≥65 years (p<0.001). In patients aged ≥70 years, the MS were 16.4 months and 13.3 months for the CFRT and HFRT groups (p=0.002), respectively. Although patients treated with CFRT were younger, had better performance scores, and more gross total resection, multivariate analysis adjusting for these factors and methylation of the MGMT gene promoter still demonstrated a survival benefit of CFRT over HFRT (p=0.002). Since this study included patients between 2006 and 2016, which was the pre-TMZ era in GBM-e, it should be noted that only elderly patients who were deemed suitable for TMZ-based chemoradiation might have been included in this study. This study is hypothesis-generating, but interpretation should be carried out with caution. From the aforementioned three retrospective studies [124748], we can hypothesize that when combined with TMZ, CFRT can afford a 3–4-month MS benefit compared to HFRT in selected GBM-e patients.
SUMMARY OF CURRENT GUIDELINES
Evidence-based practice guidelines for the treatment of GBM have been published by several groups. The European Association of Neuro-Oncology recommends HFRT alone for patients with MGMT GBM-e aged ≥70 years, whereas TMZ-based radiochemotherapy or TMZ alone is recommended for those who are MGMT+ [31]. For patients with unfavorable prognostic factors, defined by age and/or performance, consideration of HFRT as the RT regimen is recommended. In the intergroup consensus review by the Society for Neuro-Oncology and European Society of Neuro-Oncology, if the patient is deemed able to tolerate multimodality therapy, RT/TMZ→TMZ ± tumor treating fields (TTF) with either CFRT or HFRT is recommended [5]. For patients not suitable for multimodality therapy, TMZ monotherapy (±TTF) and HFRT are recommended for those who are MGMT+ and MGMT-, respectively.
According to the National Comprehensive Cancer Network guidelines, recommendations vary depending on the KPS and methylation profile of the MGMT gene promoter in GBM-e aged ≥70 years, although the selection of a specific treatment strategy may be very difficult for physicians [33]. In patients with a KPS ≥60 and MGMT+ status, both HFRT/TMZ→TMZ and CFRT/TMZ→TMZ plus TTF are recommended as category 1. CFRT/TMZ→TMZ and TMZ alone can be considered as category 2A. HFRT alone can also be considered category 2B in these patients. For patients with KPS ≥60 and MGMT-, CFRT/TMZ→TMZ plus TTF is recommended as category 1, whereas three different options (CFRT/TMZ→TMZ, HFRT/TMZ→TMZ, and HFRT alone) can also be considered as category 2A. GBM-e patients with a KPS <60 can be treated with HFRT alone, TMZ alone, or best supportive care (all category 2A). Guidelines for newly diagnosed GBM-e from the Korean Society for Neuro-Oncology are similar to the National Comprehensive Cancer Network guidelines but include fewer treatment options because TTF is not available in Korea [32].
Although published in the pre-TMZ era for GBM-e, the American Society for Radiation Oncology guidelines made an emphatic statement in that “there is no evidence that CFRT (60 Gy in 30 fractions over 6 weeks) is more efficacious than HFRT (e.g., 40 Gy in 15 fractions over 3 weeks)” [34]. This expert panel also suggested that HFRT was more appropriate, even for GBM-e with good performance status.
GERIATRIC ASSESSMENT IN ELDERLY PATIENTS
“Old” does not necessarily mean “bad.” Chronological age and performance scores, which are routinely measured parameters in oncology practice, might not necessarily reflect the exact frailty of elderly patients with cancer in certain treatments. The American Society of Clinical Oncology recommends the routine use of geriatric assessment (GA) in cancer patients aged ≥65 years receiving chemotherapy to identify the vulnerabilities of individuals and that GA results should be integrated for individualized planning of treatment selection [49]. Multiple studies have shown that GA-based interventions and modification of dosages, in chemotherapy regimens for example, successfully reduce toxicity in elderly patients with solid tumors or lymphoma while retaining acceptable oncologic outcomes [50515253]. Comprehensive GA might be time-consuming; therefore, the selection of an optimal assessment tool requiring a shorter administration time might be necessary for daily clinical practice [49].
Frailty in patients with GBM-e aged ≥65 years, measured by the Canadian Study of Health and Aging modified frailty index, has also been reported to correlate with lesser resection, longer hospitalization, increased complication risk, and decreased survival [13]. The G-8 screening tool, derived from the Mini Nutritional Assessment, which only takes approximately five minutes, is known for its correlation with mortality, even when controlling for cancer stage and performance status. Deluche et al. [54] showed that G-8 scores correlated with survival in GBM-e aged ≥65 years, even after adjusting for age, resection, chemotherapy, and RT. Geriatric assessment using various screening tools might be one strategy to identify GBM-e patients who would benefit from a more intensified RT schedule of CFRT (6 weeks) over HFRT (3 weeks) when combined with TMZ.
RADIATION ONCOLOGIST’S PERSPECTIVE AND CONCLUSION
Since 70%–90% of GBM recurrences after RT are local recurrences in the primary RT field or around the tumor bed, there is an urgent need for strategies to enhance the efficacy of local RT in GBM. Two simple strategies include increasing the physical dose of RT and using novel RT radiosensitizers. The latter is also an interesting field under active investigation, which includes agents such as epidermal growth factor receptor inhibitors, DNA damage repair pathway inhibitors, antiangiogenic therapies, and histone deacetylase inhibitors [5556]; however, this will not be further discussed in this review.
To date, brachytherapy, hypofractionation, accelerated hyperfractionation, and stereotactic radiotherapy boost have failed to significantly improve overall survival in GBM compared to CFRT of 60 Gy in a phase 3 prospective randomized trial. Although a recent meta-analysis revealed that dose-escalated RT demonstrated a survival benefit compared with standard RT of 60 Gy, the difference in survival diminished in patients treated with RT plus TMZ [57]. Furthermore, the multicenter phase 3 SPECTRO-GLIO trial comparing standard CFRT of 60 Gy (30 fractions) and simultaneous integrated boost of up to 72 Gy (30 fractions) for regions of high choline to N-acetyl aspartate ratios identified by magnetic resonance spectroscopy in GBM treated with RT/TMZ→TMZ was recently presented at the European Society Radiation Oncology 2021 Meeting [5859]. However, no difference in overall or progression-free survival was observed between both arms (MS, 22.6 months vs. 22.2 months; p=0.55). For GBM-e, a small retrospective study comparing two 3-week HFRT regimens of 40 Gy (n=39) vs. 52.5 Gy (dose-escalated arm, n=27) in GBM-e patients aged ≥60 years treated with HFRT/TMZ→TMZ was presented in the 2021 American Society for Radiation Oncology Annual Meeting [60]. MS was significantly prolonged with dose escalation in univariate and multivariate analyses. However, dose escalation in HFRT needs to be evaluated prospectively in the future. Currently, 40 Gy in 15 fractions should remain the standard HFRT regimen.
What should not be overlooked is the fact that a direct comparison between TMZ alone and RT/TMZ→TMZ in MGMT+ GBM-e patients has not yet been performed. Since both regimens offered an improved MS of 18.4 months [23] and 13.5 months [11] in MGMT+ GBM-e individuals when compared to historical controls, we should keep in mind that TMZ alone is a reasonable treatment strategy in these patients. However, treatment with TMZ alone for newly diagnosed GBM is not reimbursed by the National Health Insurance in Korea, which warrants modification.
In summary, since TMZ prolongs survival in combination RT for GBM-e patients, the optimal RT dose-fractionation in GBM-e patients suitable for RT/TMZ→TMZ needs to be addressed urgently in the near future. Furthermore, a single RT schedule, either CFRT or HFRT, would probably not fit all GBM-e; therefore, methods for appropriate patient selection based on the risk-benefits of CFRT and HFRT in combination with TMZ need to be established. We also should not be confused that GBM-e patients harboring favorable prognosticators, such as MGMT+ or gross total resection, do not qualify as the best candidates for a longer course of CFRT rather than abbreviated HFRT. The results, as well as the detailed data of subgroup analyses of ongoing prospective phase 3 trials comparing 40 Gy (3 weeks) to 25 Gy (1 week) and 60 Gy (6 weeks) in the context of TMZ-based radiochemotherapy for GBM-e, are eagerly awaited.
 XML Download
XML Download