

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Intracranial teratoma is an extremely rare disease that accounts for approximately 0.3%–0.6% of all primary intracranial tumors [1]. Moreover, intracranial immature teratomas are much rarer, malignant, and have a poor prognosis, requiring complicated treatments [123456]. Due to its histologic nature, it is mostly located in the deep midline of the intracranial hemisphere from the pineal gland to the suprasellar area [1345789]. Therefore, the tumor may cause various complications, and the deep location of the tumor makes surgery challenging, resulting in incomplete resection in many cases, and requiring multimodal treatments [10].
We present our experience with a fast-growing pineal gland immature teratoma in a 4-year-old child, who presented with obstructive hydrocephalus, which was treated with total surgical resection of the tumor. In addition, we aimed to determine the appropriate treatment modality for intracranial immature teratomas by reviewing the literature and investigating the prognosis.
Go to : 
CASE REPORT
A 4-year-old boy, who presented with drowsiness after a general tonic-clonic seizure, was admitted to the emergency department of our institute. Brain CT showed acute obstructive hydrocephalus and associated diffuse interstitial edema caused by a tumor in the pineal gland region, blocking the cerebral aqueduct (Fig. 1A). The patient showed drowsy mentality with lateral gaze impairment of right eye, indicating abducens nerve palsy. An emergency extra-ventricular drainage catheter insertion surgery was performed as a temporary measure due to the persistent drowsiness. The patient’s mental status recovered after drainage but the abducens nerve palsy did not. A brain MRI was performed to identify the tumor and it demonstrated a 2.5-cm-sized pineal gland tumor consisting of heterogeneous enhancement with calcific foci and cysts (Fig. 1B-D). There were no remarkable changes in serum alpha-fetoprotein (AFP) and beta human chorionic gonadotrophin (bHCG) levels.
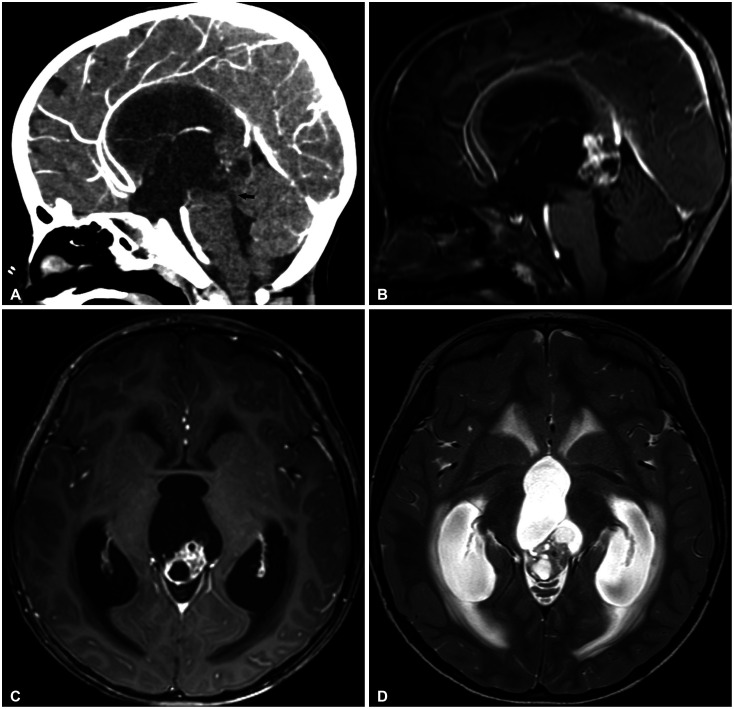 | Fig. 1Initial CT and MRI findings of the patient. A: Sagittal view of initial enhanced CT scan of the patient. A 2.5-cm-sized pineal gland tumor blocking the cerebral aqueduct and obstructive hydrocephalus were seen. B and C: Axial and sagittal views of the enhanced MRI scan after extra-ventricular drainage, showing the pineal gland tumor with heterogeneous enhancement and mixed signals due to different tissues. D: Axial view of T2-weighted image scan after extra-ventricular drainage, showing intratumoral cysts and calcification.
|
The patient underwent an endoscopic third ventriculostomy with tumor biopsy. Histopathological examination revealed a mature teratoma with cystic epithelium surrounded by mesenchymal fibrotic tissue.
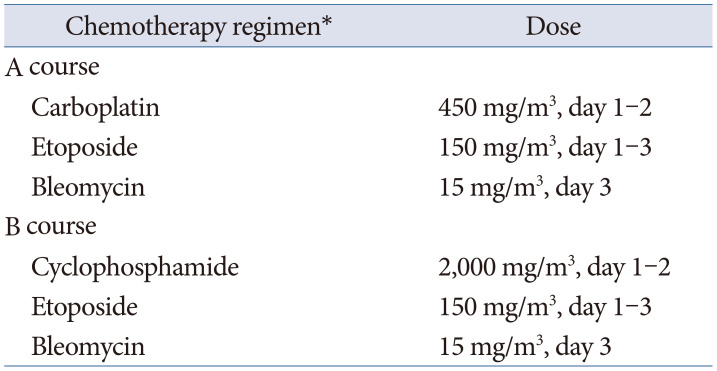
The patient was determined to undergo surgical resection of the tumor. A repeated MRI for preoperative evaluation revealed improved hydrocephalus, but a much increased solid portion of the tumor, which was 3.5 cm in size, compared to 2.5 cm at the initial scan 2 weeks prior, indicating a faster than expected growth (Fig. 2). The patient underwent surgery using the occipital transtentorial approach, and gross total resection of the tumor was performed (Fig. 3). The symptoms including seizure and abducens nerve palsy resolved after the total removal of the tumor (Fig. 4). The final histopathological diagnosis revealed primitive neuronal epithelial tissue, indicating immature teratoma (Fig. 5). Standard chemotherapy was subsequently initiated (Table 1) [10], and no recurrence was observed on the 6-month postoperative MRI scan.
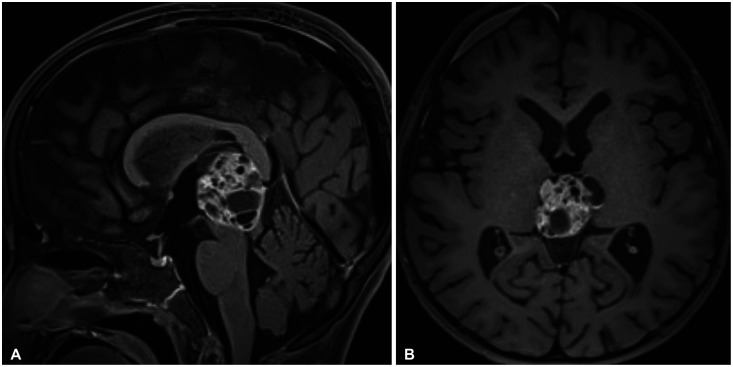 | Fig. 2Preoperative sagittal (A) and axial (B) MRI showing improved hydrocephalus after endoscopic third ventriculostomy but much increased solid portion of the tumor.
|
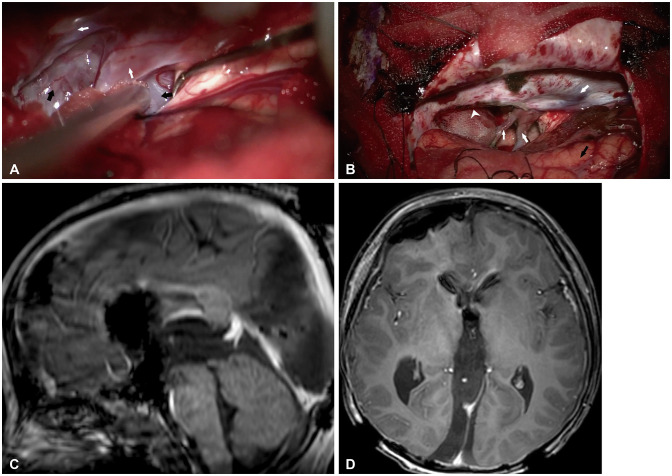 | Fig. 3Intraoperative microscopic view and postoperative MRI. A: Intraoperative microscopic image after retracting the right occipital lobe. The tumor (black arrow) anterior to deep venous system (white arrow) was noted. B: Microscopic view after gross total removal of the tumor. Right occipital lobe (black arrow), deep venous system (white arrow), and incised tentorium (white arrowhead). C and D: Postoperative MRI demonstrating no residual tumor.
|
 | Fig. 4Pre- and postoperative eyeball motion of the patient. A: Preoperative eyeball motion of the patient presenting right abducens nerve palsy. B: Postoperative eyeball motion presenting resolution of the palsy.
|
 | Fig. 5Histologic findings of the tumor (H&E stain, ×100). A: Immature cartilage with high cellularity is seen. B: Primitive neuronal epithelial tissue and multilayered neural crest forming tissue are seen, suggesting immature teratoma.
|
Table 1
Details of the chemotherapy applied [10]
![]()
Go to :
DISCUSSION
Intracranial teratoma is a rare type of non-germinomatous germ cell tumor (GCT), usually found in young patients, accounting for about 0.3%–0.6% of all primary intracranial tumor and 0.5%–1.5% of all childhood brain tumors [8]. Among the three histological types of intracranial teratoma (mature, immature, and teratoma with somatic-type malignancy), immature teratoma is known as the highly malignant, fast-growing intracranial tumor, thus presenting poor outcome and challenging for clinical diagnosis and treatment [13458910]. The tumor is usually located at the midline of the intracranial hemisphere, similar to other GCTs, and MRI findings of heterogeneous enhancement, mixed signals due to different tissues, intratumoral cyst, calcifications, and fat signals may indicate teratoma. There are some rare case reports of teratomas found in non-midline locations such as the lateral ventricles, posterior fossa, basal ganglia, and cavernous sinus [811121314]. Serum AFP and bHCG are the most commonly used tumor markers in GCTs. Although it may not be accurate, elevated serum AFP may suggest a higher likelihood of immature teratomas than mature teratomas [8911].
It is a well-known fact that the most important feature for predicting prognosis is the histological type of the malignant GCT [456915]. Open surgery is important for all suspected teratoma since they frequently have mixed portion on different histologic tumors [10]. The endoscopic approach may be a great option due to the ability to achieve tissue access under good visual control and the option to perform additional third ventriculostomy to resolve obstructive hydrocephalus caused by the tumor [9].
Many pathological conditions may be complicated by the deep midline location of the tumor. Obstructive hydrocephalus and increased intracranial pressure due to obstruction of the cerebrospinal fluid (CSF) tract, such as the foramen of Monro and cerebral aqueduct, cranial nerve palsies, hearing or visual problems due to compression of the tectum of the midbrain or optic chiasm, and endocrine problems due to hypothalamic or hypophysis dysfunction may be consequences of the tumor location. Interestingly, our case presented with a very fast growing tumor, which enlarged from 2.5 cm to 3.5 cm over 2 weeks. The patient had abducens nerve palsy, which did not resolve after drainage of CSF but resolved after the total resection of the tumor. The cause may be the pathologic stretching of the nerve as a result of the linear force of the mass effect due to the rapidly growing tumor above the midbrain, and not from the hydrocephalus [16]. Although the complications can be treated by surgical decompression and resection of the tumor, the overall 5-year survival rate of immature teratomas is poor according to the published literature [145615]. This is thought to be the result of the malignant histologic nature of the tumor, high recurrence rate, and poor complete resection rate of the surgery due to the tumor’s deep and vascular-rich location [45615]. Complete resection of tumors and adjuvant chemoradiotherapy are known to have the highest 5-year survival rate, as presented in numerous previous case series and reports [46911]. Huang et al. [4] demonstrated a significant increase in the survival curve of patients who underwent gamma knife surgery after partial removal of immature teratomas. The details of the reported cases in the published literatures are summarized in Table 2. However, these results involved only a small number of cases and some are included as a part of studies on intracranial GCT, since immature teratomas are extremely rare. Moreover, some case reports and case series have reported relatively higher survival rates (70%–100%) when total surgical resection of the tumor is performed [69]. Larger studies should be performed to determine the exact outcome and most effective treatment of the pathology.
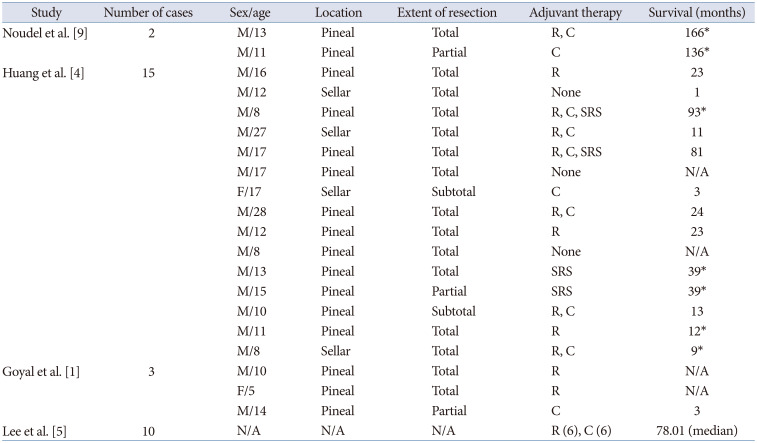
Table 2
Details of the patients with intracranial immature teratoma in the literatures
| Study | Number of cases | Sex/age | Location | Extent of resection | Adjuvant therapy | Survival (months) |
|---|---|---|---|---|---|---|
| Noudel et al. [9] | 2 | M/13 | Pineal | Total | R, C | 166* |
| M/11 | Pineal | Partial | C | 136* | ||
| Huang et al. [4] | 15 | M/16 | Pineal | Total | R | 23 |
| M/12 | Sellar | Total | None | 1 | ||
| M/8 | Pineal | Total | R, C, SRS | 93* | ||
| M/27 | Sellar | Total | R, C | 11 | ||
| M/17 | Pineal | Total | R, C, SRS | 81 | ||
| M/17 | Pineal | Total | None | N/A | ||
| F/17 | Sellar | Subtotal | C | 3 | ||
| M/28 | Pineal | Total | R, C | 24 | ||
| M/12 | Pineal | Total | R | 23 | ||
| M/8 | Pineal | Total | None | N/A | ||
| M/13 | Pineal | Total | SRS | 39* | ||
| M/15 | Pineal | Partial | SRS | 39* | ||
| M/10 | Pineal | Subtotal | R, C | 13 | ||
| M/11 | Pineal | Total | R | 12* | ||
| M/8 | Sellar | Total | R, C | 9* | ||
| Goyal et al. [1] | 3 | M/10 | Pineal | Total | R | N/A |
| F/5 | Pineal | Total | R | N/A | ||
| M/14 | Pineal | Partial | C | 3 | ||
| Lee et al. [5] | 10 | N/A | N/A | N/A | R (6), C (6) | 78.01 (median) |
![]()
In conclusion, we present a rare case of a fast-growing pineal gland immature teratoma in a 4-year-old child, which was successfully treated with complete surgical resection of the tumor through an occipital transtentorial approach. Intracranial immature teratomas may present with various serious pathological symptoms and are difficult to treat due to the deep location and highly malignant nature of the tumor. Complete surgical removal and adjuvant chemoradiotherapy are the effective treatments of choice for this pathology.
Go to :
 XML Download
XML Download