

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ulcerative colitis (UC) is an idiopathic condition of the large intestine, in which inflammatory damage extends continuously from the rectum with variable extension to more proximal portions of the colon. Persistent inflammation and mucosal ulceration can lead to the recognized acute complications of UC including toxic megacolon, perforation and bleeding.1 Although genetic factors have demonstrated a role in the pathogenesis of UC, various environmental factors have been implicated in the rising incidence of UC.2 Enteric infections have been hypothesized to trigger an altered immune response leading to chronic inflammation.3 However, previous studies have also suggested a detection bias in the isolation of traditional enteric pathogens in IBD.3 Here we present the case of a newly diagnosed patient with UC presenting with multiple confounding enteric infections.
Go to : 
CASE REPORT
A 24 year-old male with no significant past medical history and no history of smoking was transferred to our facility for evaluation of refractory colitis. Four weeks prior to transfer, the patient underwent a dental bone graft procedure and was administered antibiotics to include amoxicillin and clindamycin. Within 1 week the patient developed watery diarrhea up to 10–12 times daily. The patient was initially administered a 5-day course of metronidazole empirically, and initial Clostridium difficile PCR toxin assay while on metronidazole returned negative. The patient had no improvement in clinical symptoms on metronidazole.
Two weeks prior to transfer, the patient was evaluated by a gastroenterologist and second C. difficile PCR toxin assay returned positive. Treatment was initiated with vancomycin without clinical improvement. The patient was subsequently admitted to an outside facility 1 week prior to transfer with a CT scan of the abdomen demonstrating pancolitis (Fig. 1). The patient had no clinical improvement with oral vancomycin and intravenous metronidazole. He further described persistent abdominal pain, night sweats and a 11 kg weight loss.

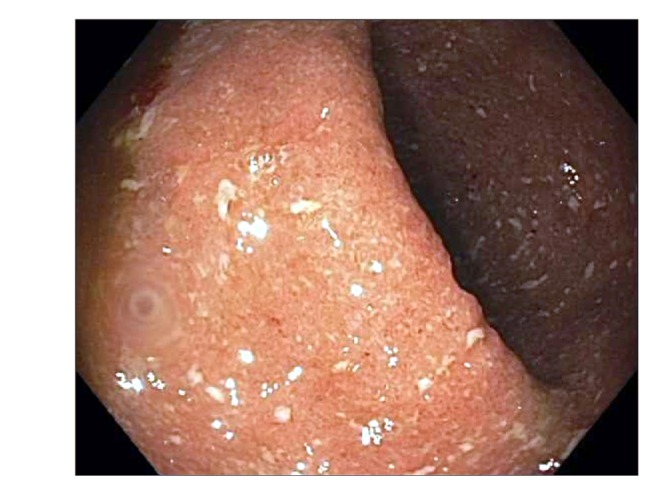
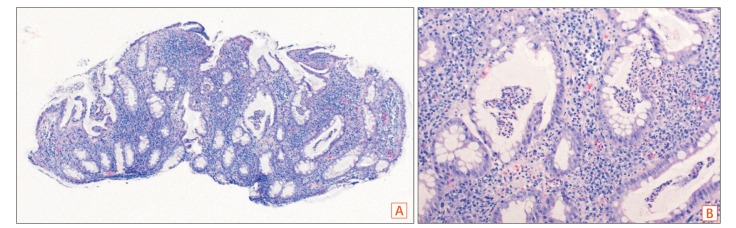
On transfer to our facility, the patient had persistent bloody diarrhea. On physical examination the patient was afebrile and had diffuse abdominal discomfort. Initial laboratory studies revealed an elevated CRP, 41 mg/L, with a decreased albumin, 2.5 g/dL. Flexible sigmoidoscopy was performed demonstrating active colitis, without rectal sparing, and containing granular mucosa with a complete loss of vascular pattern (Fig. 2). Pathology revealed active colitis without changes of chronic colitis and without evidence for cytomegalovirus infection (Fig. 3). Stool culture on admission returned positive for Klebsiella oxytoca while repeat C. difficile PCR toxin assay following transfer was negative.
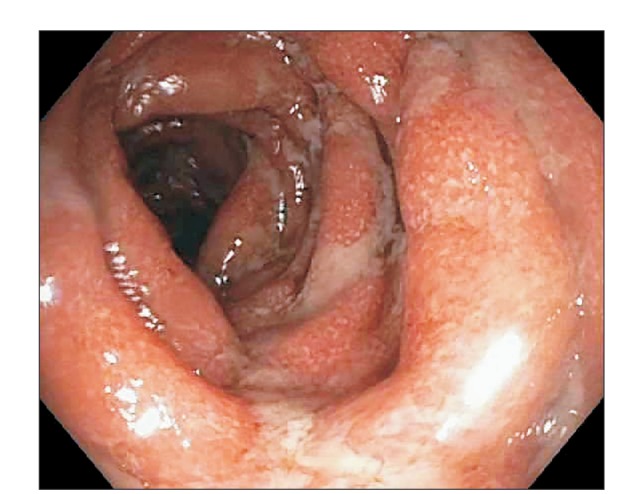
Given the presence of acute colitis and concern for antibiotic-associated hemorrhagic colitis secondary to K. oxytoca, antibiotics were withdrawn with clinical improvement in stool frequency. The patient was discharged with 1-week follow-up, at which time he continued to report symptoms of persistent colitis and weight loss. Repeat stool studies were performed to include a negative stool culture and positive C. difficile PCR toxin assay. Without formal diagnostic criteria present for UC, and in concern for recurrent C. difficile infection (CDI), the patient underwent a fecal microbiota transplantation (FMT) utilizing a third party source and instillation via colonoscopy, although no demonstrated clinical benefit was achieved. Colonoscopy at the time of FMT demonstrated persistent active colitis with a Mayo endoscopic subscore of 2 extending from the anal verge to the cecum (Fig. 4). Biopsies revealed moderately active chronic colitis, now consistent with a diagnosis of UC.
Given lack of response to therapies for antibiotic-associated hemorrhagic colitis and CDI, and with biopsies now favoring UC 3 weeks after initial presentation, the patient was hospitalized due to persistent colitis, weight loss and abdominal discomfort. Therapy was initiated for severe UC to include intravenous corticosteroids and cyclosporine.4 The patient was discharged on oral tapering doses of prednisone and cyclosporine with transition to oral azathioprine. Subsequently, salvage therapies to include infliximab, vedolizumab and tofacitinib were trialed without clinical or endoscopic response despite targeting recommended drug levels resulting in the performance of a total colectomy fifteen months after initial presentation. Pathology from the colectomy specimen was consistent with severely active chronic colitis consistent with a final diagnosis of UC (Fig. 5). Informed consent was obtained from the patient for description of this case.
 | Fig. 5(A) Representative image from colectomy specimen showing severe UC with extensive mucosal denudation (H&E, ×10). (B) Medium (H&E, ×40) and (C) high power (H&E, ×100) showing features of severe (mucosal denudation) to moderately active (crypt abscesses) UC with prominent basal lymphoplasmacytosis.
|
Go to :
DISCUSSION
This is the first case report of K. oxytoca and C. difficile complicating a new diagnosis and management of UC. The role of enteric infections in the development of IBD has been postulated since the original disease descriptions, although a current accepted hypothesis is that commensal enteric bacteria provide constant antigenic stimulation to activate pathogenic T cells to cause chronic inflammation.5 As an altered microbial composition in IBD can result in increased immune stimulation and epithelial dysfunction, it is interesting to hypothesize the role of antibiotics triggering alterations in microbial composition.5 Recent studies in mouse models have demonstrated intergenerational transfer of antibiotic disturbances in the microbiota to the development of colitis in predisposed offspring.6 Extension of studies to the human demonstrated an increased risk of IBD among individuals exposed antibiotics, although exposure was only significant for the development of CD.7
K. oxytoca is a Gram-negative cytotoxin producing bacteria which has been previously described as the causative organism of antibiotic-associated hemorrhagic colitis, with only a single previous co-occurrence with C. difficile.89 In the initial report of 22 patients with antibiotic-associated colitis, 6 patients had findings on colonoscopy to include hemorrhagic colitis, of which 5 had isolated K. oxytoca. The primary associated antibiotics included penicillin derivatives and colonoscopy demonstrated a segmental colitis with rectal sparing.8 A subsequent case report associated K. oxytoca with the development of diffuse pseudomembranous colitis in the setting of perioperative antibiotic use and stool studies negative for alternative causes of pseudomembranous colitis to include cytomegalovirus, Shigella dysenteriae, Escherichia coli O157:H7. With withdrawal of empiric antibiotic therapy, diarrhea resolved within 4 days.10 A single case report has described K. ocytoca complicating a diagnosis of CD,11 while stool samples from 235 patients with IBD identified 11 (4.7%) harboring K. ocytoca, among which 2 strains were toxigenic.12
This case report highlights the potential detection bias of enteric infections complicating a new diagnosis of UC. A study assessing the risks of Salmonella or Campylobacter isolation in stool culture demonstrated increased risks of both CD and UC following isolation of the enteric pathogens. However, risk of IBD was also increased with negative stool cultures, thus questioning the causality of the individual enteric infections and suggesting a detection bias related to increased testing for pathogens in IBD.3
Although there is no evidence to support an etiologic role for CDI in IBD, it appears to be responsible for exacerbations of disease activity, leading to increased rates of hospitalization and colectomy.1314 Early studies focused on the isolation of C. difficile toxin in the stool of relapsed patients demonstrating isolation rates of 4% to 19% in patients with symptomatic relapsed IBD.1516 However, asymptomatic carriage of C. difficile has also been reported at an increased frequency compared to the general population with 8% of individuals with asymptomatic IBD carrying strains with a diversity pattern reflecting community acquisition.1718
Previously established reference standards for the diagnosis of CDI including cell cytotoxin assay and cytotoxigenic culture have been largely replaced with more cost-effective enzyme immunoassays and highly sensitive rapid PCR assays. However, changes in the test characteristics must be applied to clinical patient outcomes. In a recent study comparing PCR testing for toxin with molecular toxin immunoassays, individuals diagnosed with CDI by only PCR had shorter rates of diarrhea and no CDI-related complications, concluding that over-diagnosis leads to unnecessary treatment and increased health care costs.19
This case report highlights the detection bias related to increased testing for stool pathogens in IBD as well as the potential etiologic role of microbiota disturbances in the development of IBD. While individual pathogens or antibiotics have not been demonstrated to be a causative factor in IBD, the shifts in the bacterial, fungal and viral environments in the intestinal track may play a role in the development of inflammation in genetically predisposed individuals. With the initial development of antibiotic-associated acute colitis in this case, strategies targeting enteric pathogens did not lead to resolution of clinical symptoms. Following the onset of chronic colitis demonstrated on histology, evidence-based strategies for UC were employed in an attempt to achieve clinical remission without benefit and leading to total colectomy. Therefore, this case highlights both the potential role of disturbances in the microbiota leading to the onset of IBD as well as the need for a high index of suspicion for underlying IBD among individuals presenting with enteric infections without previously identified risk factors, allowing for the prompt recognition and treatment of severe IBD.
Go to :
 XML Download
XML Download