

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Celiac disease is an immune-mediated enteropathy characterized by intolerance to gluten and similar proteins of barley and rye in genetically susceptible individuals. In the past, celiac disease was considered a rare disorder affecting persons mainly of European origin.12 However, in the last decade and a half, the disease has moved from obscurity to a popular spotlight, being one of the most common treatable autoimmune disorders to affect humans. The disease has heterogeneous clinical presentations.34 The classic constellation of symptoms and signs which characterize malabsorption, i.e., chronic diarrhea, abdominal bloating, failure to thrive and so forth are the so-called typical, classical, diarrheal or intestinal forms of disease presentation.5 Other diverse ways in which celiac disease manifests such as fatigue, iron deficiency anemia, short stature, osteomalacia or osteoporosis, cryptogenic liver disease etc. are variously described as atypical, extra intestinal, non-diarrheal or non-classic presentations of celiac disease.6 Other terminologies used are silent group, “at-risk,” “potential celiac disease” and “latent celiac disease.”7 Similarly the age of onset/diagnosis labels a case of celiac disease as pediatric celiac disease or adult celiac disease with varied cutoffs as distinction between the two. This variation in terminologies used to define gluten related disorders invoked interest of international experts who got together to provide simple definition for celiac disease and related terms in their recent “Oslo definitions.”8 The use of terms typical, atypical, silent and latent celiac disease was discouraged. The focus of Oslo group was to clarify the use of terminologies in relation to gluten related disorders and not disease characterization or classification in relation to various parameters.
In clinical practice, just labeling a case of celiac disease according to presentation alone or according to age of diagnosis alone does not give a lucid description of the disease. Hence, we believe that more stringent adoption of consistent, standardized classification of celiac disease according to relevant variables is necessary in the modern era of data collection and disease management. Moreover, a classification system would provide a common language with which professionals can discuss patients, regardless of their geographical location. Celiac disease, though known for decades, still presents a challenge for classifying individuals as no definite classifiers have been recognized and put together in a meaningful fashion. Till date, no phenotypic classification has been used for celiac disease patients. Therefore, an attempt is made in this paper to develop a clinical phenotypic classification system for celiac disease.
METHODS
For the purpose of a simple phenotypic classification aimed at providing a composite diagnosis of celiac disease, our team considered different parameters for disease characterization. Various attributes of the patients that our group agreed for classifying disease phenotype included age at diagnosis, age at onset of symptoms, disease presentation, and complications. The study was approved by the Institutional Review Board (IRB No. 2014-78 DMC/R&D-2015/220), informed consent was not needed.
1. Definitions
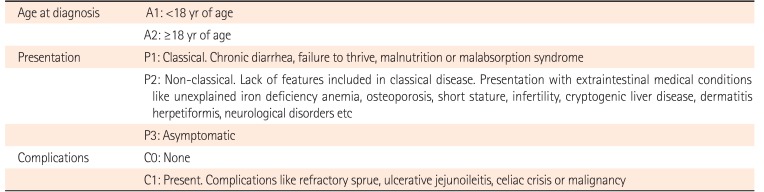
Age at diagnosis was defined as the age at establishment of diagnosis of celiac disease based on modified ESPGAN criteria.9 Age at the time of onset of symptoms was also recorded. The disease presentation was sub-classified as (1) P1 (classical celiac disease)-patients who presented with diarrhea, failure to thrive and features of malnutrition and/or malabsorption syndrome; (2) P2 (non-classical celiac disease)-patients who lacked features included in P1 (classical form) and presented with either or combination of medical conditions like unexplained iron deficiency anemia, osteoporosis, short stature, infertility, cryptogenic liver disease, dermatitis herpetiformis and neurological symptoms, and so forth; (3) P3 (latent celiac disease)-patients with positive celiac disease serology but with normal duodenal histology; and (d) P4 (screen detected)-patients who were detected during screening of “at-risk” population. Patients with both intestinal and extraintestinal manifestations were included in the first group (P1, classical celiac disease). The disease complications were divided as either C0–no complications or C1–with complications like refractory sprue, ulcerative jejunoileitis, celiac crisis or malignancy.
2. Data Analysis
The cutoffs for age for defining pediatric cases (i.e., <18 or <15 years) were analyzed separately. In addition, cross tabulations were used for the verification of both the age at onset of the symptoms and the age at diagnosis of celiac disease. The variables for the proposed classification were applied to our data registry which included 1,664 patients with confirmed diagnosis of celiac disease.
In addition, it was decided to be sent to 30 recognized national and international experts on celiac disease for opinion. The experts included 22 gastroenterologists, 3 pediatricians, 4 physicians and 1 professor of genetics (working on genetics of celiac disease in children and adults). There were areas of consensus and areas where there was need for consideration before a final consensus.
RESULTS
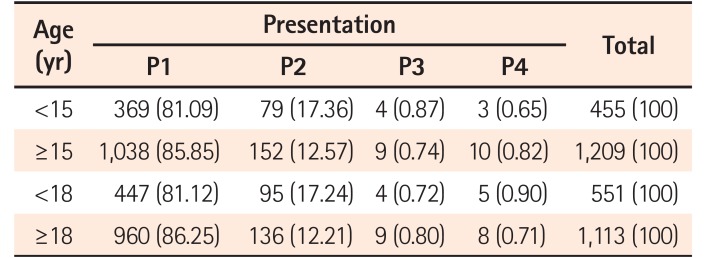
Our dataset of 1,664 patients were classified according to age groups and clinical presentation. First tabulation consisted of 2 variables: the age of diagnosis with 2 categories such as <18 years and ≥18 years by the reference classification variable, disease presentation. Similarly, the second included age groups as <15 years and ≥15 years along with the same reference classification variable. As can be seen in Table 1 below, the row percentages for the corresponding age categories are almost identical implying that it does not make any difference whether the cutoff criteria is ≤15 years or ≤18 for characterization of celiac disease into pediatric and adult onset.
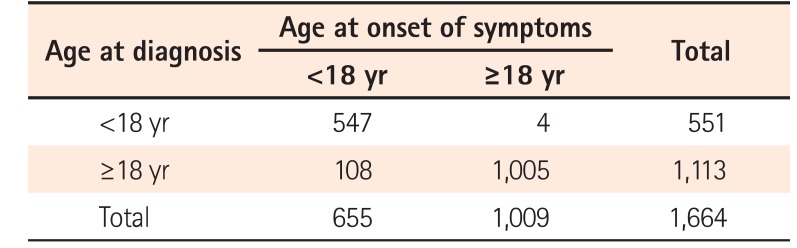
Again, the 2 variables, i.e., age at onset of symptoms and age at diagnosis were analyzed (Table 2). Surprisingly, we found that 93% ([547+1,005]/1,664) of the 1,664 cases were the same between the 2 variables for a given grouping of the age variable suggesting that there is a good concordance between age of onset of symptoms and age of diagnosis.
Hence, it was agreed to use the following classifiers: age at diagnosis of disease, presentation and complications. Of the 20 experts who responded to the e-mail 12 were gastroenterologists, 4 physicians and 3 pediatricians and 1 professor of genetics. Substantive comments from experts included the basis for 18 years as cutoff. In order to incorporate their concern, we have explained at length the rationale for setting 18 years as the cutoff age in the discussion section. The other concerns regarding presentation sub-categories included P3 to be deleted, P1 and P2 overlap and nomenclature of P1 and P2 as diarrheal and non-diarrheal. In addition, one expert had concern about the inclusion of complications in the classification as it needed investigative work-up and occurred in later stages. Majority of the experts provided strong support for the classification. They also indicated in their return reply along with their tabular responses that the classification is simple and elegant and can be very useful for both practitioners and researchers alike.
After taking into consideration the suggestions made by the experts, the classification was modified as shown in Table 3. It was agreed to delete P3 as latent disease and P4 as silent disease or screen detected and in turn, to rename P3 as asymptomatic disease. Using these variables on the database for classification we could identify our patients as A1P1C0 447, A1P2CO 95, A1P3C0 9, A2P1C0 955, A2P1C1 5, A2P2C0 131, A2P2C1 5, and A2P3C0 17. Intestinal complications were identified in 10 patients above the age of 18, were jejunoileitis (n=2), celiac crisis (n=2), refractory sprue (n=1), carcinoma esophagus (n=1), stomach (n=1), ovary (n=1), small bowel (n=1), and nodal lymphoma (n=1).
DISCUSSION
Various factors known to influence the course of celiac disease and its long-term prognosis are: age at diagnosis of disease, disease presentation and complications. The age of diagnosis may reflect the severity of disease and perhaps, associated complications. Disease management and prognosis change vastly once these complications set in. Furthermore, disease presentation can be an easy guide for individualized management and follow-up plan for each patient. For instance, for a patient presenting with osteoporosis, the treating physician would like to follow-up with serial DEXA (dual energy X-ray absorptiometry) scans while serial hemogram monitoring would be required for a patient who had iron deficiency anemia as the presenting feature. Disease presentation also matters as asymptomatic patients may not be very much willing to accept major dietary modifications resulting in poor dietary compliance. With such a wide range of disease presentations having impact on disease behavior, it becomes imperative that disease pattern of each patient needs to be categorized individually. Hence, it is of paramount importance to characterize each patient's disease according to these factors since just writing a diagnosis of celiac disease does not provide required information about the disease. In order to achieve this and ensure a composite diagnosis we are suggesting a phenotypic classification based primarily on 3 variables, i.e., age at diagnosis, presentation and complications (APC classification) (Table 3). For instance, a 30-year-old patient presenting as iron deficiency anemia diagnosed as celiac disease will be classified as A2P2 (iron deficiency anemia) C0. The classification remains open to change in category on serial follow-ups. Similarly, development of intestinal complications would result change in category from C0 to C1.
Based on extensive review of literature and our own clinical experience, age was considered as one of the important parameters. With respect to the “cutoff age” for defining pediatric cases, we argue that it would be appropriate to take children who are less than 18 years of age. However, there is no consensus on this as some researchers argue in favor of age ≤15 years. Moreover, we were guided by the “Convention on the Rights of the Child,” adopted by the United Nations General Assembly on 20 November, 1989. According to article 1 of the convention, “a child means every human being below the age of 18 years unless, under the law applicable to the child, majority is attained earlier.”10 Furthermore, according to Indian Association of Pediatric Policy Statement on Age of Children for Pediatric Care (1999): “For fulfilling the professional obligations of pediatricians to the society at large, the purview of pediatrics commences with the fetus and continues through newborn, infancy, preschool and school age including adolescents up to and including 18 years of age.”11
Another challenge was to choose between the 2 factors, i.e., the age at onset of the disease and the age at diagnosis for the classification exercise. Although it was desirable to choose the age at onset of the symptoms for age characterization but it would have entailed a recall bias, more so among older patients and hence we considered age at diagnosis for classification. Moreover, this corroborates with findings of other researchers.12
We think that this classification provides clinically relevant information with regard to the disease so as to have a composite diagnosis. Overall, useful applications of this classification can be (1) phenotypic characterization of disease for each patient; (2) individualized disease management and follow-up for each patient; (3) more precise monitoring of the disease behavior; (4) highlighting of the disease related complications resulting in a close follow-up of such patients with specific investigations; (5) better identification of disease pattern in different populations or countries with a uniformity in disease classification; (6) easier recognition of changing trends in disease presentation; and (7) characterization of more homogenous subgroups for research purposes.
We have attempted to formulate a disease explanatory simple classification for patients with celiac disease. This classification scheme is not related to disease prognosis and makes no reference to histology or genetics. It is anticipated that as we learn more about the disease and put this classification into practice, further validation by other centers will be useful. All classifications tend to have some inconsistencies or inaccuracies and we believe that the present effort is no exception.
 XML Download
XML Download