

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Elderly patients with hip fractures often receive allogeneic blood transfusions during the perioperative period.12 Studies have shown that 39–70% of elderly patients undergoing hip fracture surgery receive postoperative blood transfusion.345 Aging is associated with impaired control of proinflammatory cytokines, which have a negative effect on hematopoiesis through decreased erythropoietin receptor function or inhibition of erythropoietin production.6 The predictors of postoperative transfusion in patients following hip fracture surgery were preoperative hemoglobin (Hb) levels, female sex, increased age, hypertension, chronic obstructive pulmonary disease, American Society of Anesthesiologists (ASA) classification, and intertrochanteric and subtrochanteric femur fractures.127 Anemia may occur secondary to chronic comorbidities or because of blood loss from hip fractures and surgery.89 Therefore, perioperative allogeneic red blood cell (RBC) transfusion is frequently performed to correct anemia caused by fractures or surgery-related bleeding. Transfusion increases the risk of postoperative complications, including infection, pneumonia, increased length of hospital stay, delirium, and mortality.101112 Therefore, it is necessary to reduce blood transfusions after surgery.
Patient blood management (PBM) is an evidence-based medical concept for maintaining Hb concentrations, optimizing hemostasis, and minimizing blood loss to improve patient outcomes.13 In particular, PBM programs, such as restrictive Hb threshold, the clinical decision support model, and education, have effectively reduced unnecessary RBC utilization perioperatively.1415 The World Health Organization adopted PBM in 2010, supported by the National Blood Transfusion Committee and National Health Service Blood and Transplant in the United Kingdom. However, in Korea, many hospitals have not yet introduced PBM; therefore, the transfusion rate for hip fracture surgery is very high.1617
Elderly patients with hip fractures tend to receive more liberal transfusions than other patients due to the possibility of being susceptible to low Hb levels.18 However, recent studies have reported that restricted transfusion was not inferior to liberal transfusion in elderly patients with hip fractures.181920212223 A total of 77% of patients who underwent hip arthroplasty received RBC transfusion from 2007 to 2015 in a Korean nationwide study.17 This transfusion rate is higher than those reported in other countries.345
The blood shortage has been getting worse due to the low birth rate and aging population. Furthermore, the recent coronavirus disease 2019 (COVID-19) pandemic has resulted in significant declines in blood supply due to the withdrawal of community-based and mobile blood drives in the United States.24 In Korea, the lack of blood supply also has become a social problem due to the COVID-19 pandemic.25 Therefore, efforts to reduce blood transfusion through PBM are essential to prepare for an unstable blood supply crisis.25 Our hospital has been implementing the PBM program through a multidisciplinary clinical community approach for the first time in Asia. Improvement in the appropriateness of RBC transfusion was reported in the medical and surgical patients at our institution.15 However, an analysis based on the surgery type was not performed.
We aimed to analyze the effect of our hospital’s PBM program on the appropriateness of allogeneic RBC transfusion and the postoperative clinical outcomes in elderly patients following hip fracture surgery.
METHODS
Establishment of the blood transfusion management program
The development and implementation of the PBM program at the Korea University Anam Hospital, Seoul, Republic of Korea, began in January 2018. A task force team was established that revised the PBM program with updated recommendations according to the guidelines,26 which supported restrictive transfusion. Awareness and distribution of the updated guideline recommendations by the PBM program was accomplished via educational programs at workshops carried out within the Anam Hospital in 2018. Furthermore, a Bloodless Medicine Center was established in October 2018, and educational programs were successfully incorporated into various conferences of the medical and surgical departments in 2018 and 2019. After the successful administration of the PBM education program in July 2019, a clinical advisory decision support tool was incorporated into the computerized order communication system. This model required a supplementary process before placing an order for blood transfusion, wherein one of the authorized blood transfusion indications in a pop-up window needed to be selected by the prescribing healthcare provider. Additional lectures regarding other educational programs reflecting the updated model in the computerized order communication system were given at conferences within the Anam Hospital during November and December 2019 to increase awareness of the program. Preoperative diagnosis and treatment of anemia had been actively performed in the emergency room or ward because hip fracture patients required emergency or immediate surgery. The 1,000 mg of intravenous (IV) iron was administered the day before surgery in anemic patients. During surgery, anesthesiologists induced controlled hypotension in patients without cardiovascular disease and maintained normothermia, and performed single-unit RBC transfusion in hemodynamically stable patients. The orthopedic surgeon administered the antifibrinolytic drug, tranexamic acid topically to the surgical site to reduce bleeding. Unnecessary laboratory tests should be reduced to decrease phlebotomy blood loss in perioperatively. Based on the key timeline of the implementation, three periods of the PBM program were defined: pre-PBM (January 2017–December 2017), early-PBM (January 2018–June 2019), and late-PBM (July 2019–December 2020). In addition, two periods of the PBM program were defined for the present study: pre-PBM (January 2017–December 2017) and post-PBM (January 2018–December 2020).
Patient population and definitions
This retrospective study was performed at the Korea University Anam Hospital, which offers tertiary care and has 1,048 hospital beds. Elderly patients aged ≥ 65 years who underwent hip fracture surgery from 2017 to 2020 were reviewed and included in the study. Demographics, clinical characteristics, transfusion-related information, such as the number of RBC transfusions in units and Hb levels, types of orthopedic surgery, and clinical outcomes, were collected.
Indications of the authorized RBC transfusion according to the guideline26 were defined as follows: 1) anemia (Hb < 7 g/dL); 2) clinical condition deemed suitable for RBC transfusion with Hb levels of ≥ 7 g/dL to < 10 g/dL: 2-1) infant ≤ 6 months, 2-2) pulmonary disease (arterial oxygen saturation < 90%), 2-3) cardiovascular disease (congestive heart failure, coronary artery disease, and acute myocardial infarction), 2-4) cerebrovascular disease, 2-5) bone marrow dysfunction, 2-6) peripheral vascular disease, and 2-7) sepsis; 3) acute hemorrhage: 3-1) acute blood loss of > 1,500 mL, 3-2) acute blood loss of 750–1,500 mL in patients with a Hb level of < 10 g/dL, 3-3) acute blood loss of 750–1,500 mL in patients with pulmonary disease or cardiovascular disease, and 3-4) acute blood loss during the postpartum period (cesarean delivery: blood loss of ≥ 1,000 mL; vaginal delivery: blood loss of ≥ 500 mL); 4) protocol for massive transfusion; 5) solid organ transplantation: 5-1) pre-deposit transfusion before heart surgery, 5-2) lung transplantation, 5-3) liver transplantation, and 5-4) heart transplantation. RBC transfusion administered to the patients in accordance with the indications above was defined as appropriate RBC transfusion. RBC transfusion performed outside of the approved indications was defined as inappropriate RBC transfusion. Adverse outcomes were defined as in-hospital mortality or readmission to the hospital within 30 days of discharge (30-day readmission).
Statistical analysis
Statistical analysis was performed using SPSS, version 18.0 for Windows (SPSS Inc., Chicago, IL, USA). Continuous variables were compared using the Kruskal–Wallis test. A linear-by-linear association test was employed to detect differences in categorical variables among the three periods of PBM program implementation (pre-PBM, early-PBM, and late-PBM). A comparative analysis of the risk factors for adverse clinical outcomes was performed. The Pearson χ2 test and Fisher’s exact test were used for dichotomous variables. Variables with a P value of < 0.2 on comparison analysis were included in a multivariable logistic regression analysis to determine risk factors associated with adverse clinical outcomes. Odds ratios (ORs) and 95% confidence intervals (CIs) were also calculated. A P value of < 0.05 was considered statistically significant.
RESULTS
In total, 884 patients were included in the analysis. The study population comprised 625 females (70.7%) with a median age of 80 years (interquartile range [IQR], 75–85 years). The patients were classified into three groups according to the period of PBM implementation. The proportions of pre-PBM, early-PBM, and late-PBM were 22.6% (n = 200), 38.9% (n = 344), and 38.5% (n = 340), respectively. There was a trend of decreasing female predominance (74.5%, 72.1%, and 67.1%; P = 0.054) and increased hypertension prevalence (48.0%, 61.0%, and 62.9%; P = 0.001) in the pre-PBM, early-PBM, and late-PBM periods, respectively. The types of orthopedic surgeries were significantly different. The proportions of femur fracture fixation were 53.0%, 48.5%, and 41.5% (P = 0.007), while those of total hip replacement arthroplasty were 21.5%, 26.2%, and 33.5% (P = 0.002), in the pre-PBM, early PBM, and late PBM periods, respectively. There was a significant difference in the ASA Physical Status Classification System.19 The proportion of ASA class II decreased (63.5%, 41.0%, and 40.6%; P < 0.001), while those of ASA class III (36.0%, 54.7%, and 50.0%; P = 0.009) and ASA class IV (0.0%, 4.1%, and 9.1%; P < 0.001) increased in the pre-PBM, early-PBM, and late-PBM periods, respectively. The proportion of patients who received RBC transfusion significantly decreased (43.5%, 40.1%, and 33.2%; P = 0.013), while the appropriateness of RBC transfusion (54.0%, 60.1%, and 94.7%; P < 0.001) significantly increased in the pre-PBM, early-PBM, and late-PBM periods, respectively (Fig. 1). Although there was no significant difference in the in-hospital mortality (0.5%, 2.6%, 2.1%; P = 0.340), the duration of in-hospital stay (median days: 12, 11, and 9; P < 0.001) and the rate of 30-day readmission (12.0%, 7.6%, and 6.8%; P = 0.045) significantly decreased in the pre-PBM, early-PBM, and late-PBM periods, respectively (Table 1, Figs. 2 and 3).
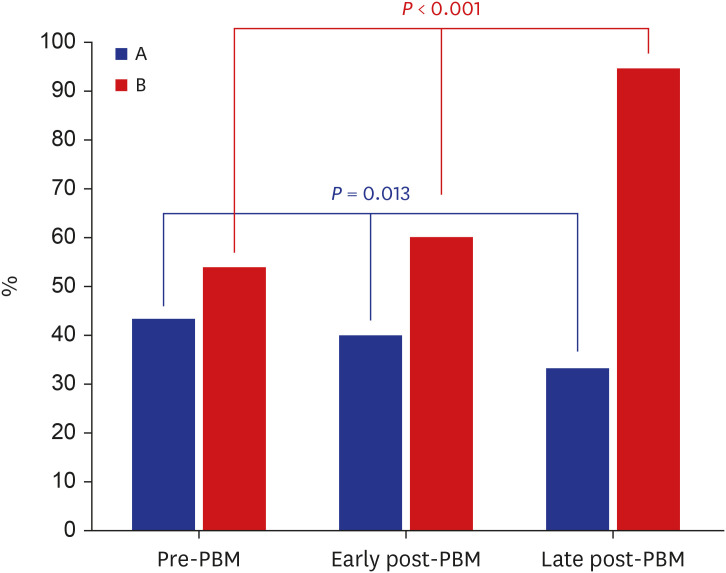
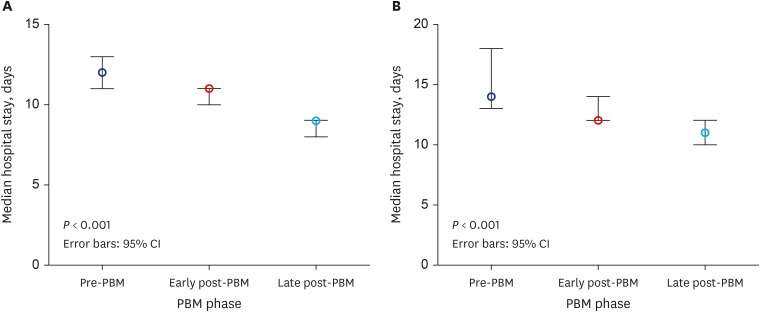
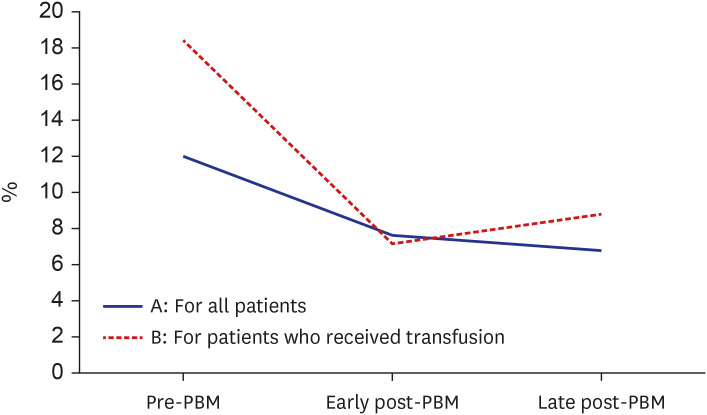
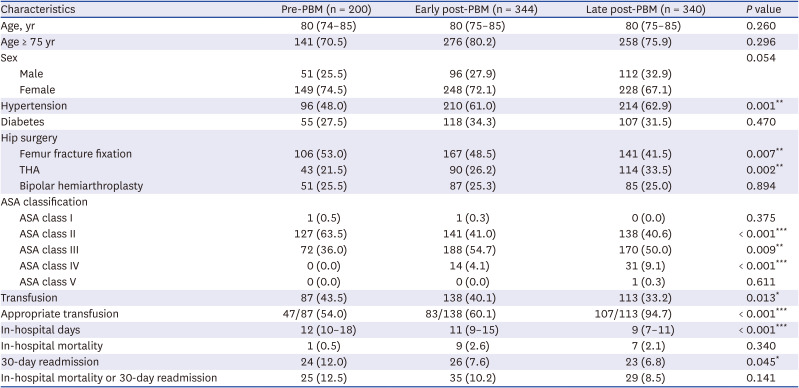
Fig. 1
Comparison of red blood cell transfusion before and after implementation of patient blood management program. (A) The proportion of patients who received RBC transfusion. (B) The appropriateness of RBC transfusion.
PBM = patient blood management, RBC = red blood cell.
![]()
Fig. 2
In-hospital stay (median days) in the pre-PBM, early post-PBM, and late post-PBM periods. (A) All patients. (B) Patients who received transfusion.
PBM = patient blood management, CI = confidence interval.
![]()
Fig. 3
The rate of 30-day readmission in the pre-PBM, early post-PBM, and late post-PBM periods.
PBM = patient blood management.
![]()
Table 1
Characteristics of the elderly patients who underwent hip fracture surgery (N = 884)
Values are presented as median (interquartile range; Q1, Q3) or frequency (%).
PBM = patient blood management, THA = total hip arthroplasty, ASA = American Society of Anesthesiologists.
*P < 0.05, **P < 0.01, ***P < 0.001.
![]()
A subgroup analysis stratified according to the ASA class was performed. For ASA class II, the proportion of patients who received RBC transfusion decreased (36.2%, 27.0%, and 25.4%; P = 0.055), while the appropriateness of RBC transfusion (60.9%, 57.9%, and 97.1%; P = 0.001) significantly increased in the pre-PBM, early-PBM, and late-PBM periods, respectively. While there were no significant differences in terms of in-hospital mortality or 30-day readmission, the duration of the in-hospital stay (median days: 11, 10, and 8; P < 0.001) significantly decreased in the pre-PBM, early-PBM, and late-PBM periods, respectively. For ASA class III, the proportion of patients who received RBC transfusion significantly decreased (55.6%, 48.9%, and 38.8%; P = 0.010), while the appropriateness of RBC transfusion (47.5%, 63.0%, and 93.9%; P < 0.001) significantly increased in the pre-PBM, early-PBM, and late-PBM periods, respectively. Both the duration of in-hospital stay (median days: 14, 12, and 9; P < 0.001) and the 30-day readmission rate (22.2%, 9.0%, and 10.0%; P = 0.029) significantly decreased in the pre-PBM, early-PBM, and late-PBM periods, respectively. For ASA class IV, there was a non-significant tendency of decreasing proportions of patients who received RBC transfusion (57.1% and 38.7%; P = 0.255) in the early-PBM and late-PBM periods, respectively. However, the appropriateness of RBC transfusion (37.5% and 91.7%; P = 0.018) significantly increased in the early-PBM and late-PBM periods, respectively. The duration of in-hospital stay (median days: 16 and 9; P = 0.010) significantly decreased, whereas there were no significant differences in terms of in-hospital mortality and the 30-day readmission rate in the early-PBM and late-PBM periods, respectively. These are presented in the Supplementary Tables 1, 2, 3.
Stratified analysis was conducted for patients who received a transfusion. The proportion of older patients aged ≥ 75 years (78.2%, 89.1%, and 90.3%; P = 0.017) and the appropriateness of RBC transfusion (54.0%, 60.1%, and 94.7%; P < 0.001) significantly increased in the pre-PBM, early-PBM, and late-PBM periods, respectively. Among the patients who were deemed to have received appropriate RBC transfusion, the most common indication for transfusion was a Hb level of ≤ 7 g/dL (78.7%, 85.5%, and 74.8%, respectively). Although there was no significant difference in the number of RBC transfusion units employed (median unit: 2, 2, and 2; P = 0.758), Hb levels prior to RBC transfusion significantly decreased (median Hb [g/dL]: 7.1, 6.9, and 6.5; P < 0.001) in the pre-PBM, early-PBM, and late-PBM periods, respectively. The proportion of patients with Hb levels of < 7 g/dL significantly increased (47.1%, 55.1%, and 74.3%; P < 0.001), while the proportion of patients with Hb levels of 7–10 g/dL significantly decreased (51.7%, 44.2%, and 25.7%; P < 0.001). The duration of in-hospital stay (median days: 14, 12, and 11; P < 0.001) and the 30-day readmission rate (18.4%, 7.2%, and 8.8%; P = 0.044) significantly decreased, while there was no significant difference in in-hospital mortality in the pre-PBM, early-PBM, and late-PBM periods, respectively (Table 2, Figs. 2 and 3).
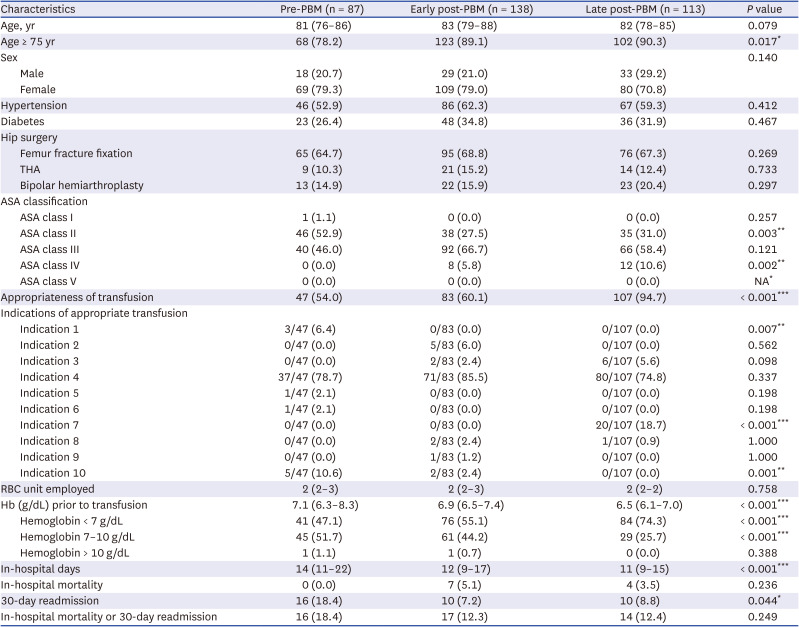
Table 2
Stratified analysis controlled for the patients who received red blood cell transfusion
Values are presented as median (interquartile range; Q1, Q3) or frequency (%).
PBM = patient blood management, THA = total hip arthroplasty, ASA = American Society of Anesthesiologists, Indications of appropriate transfusion = 1) ongoing bleeding, 2) 750–1,000 mL blood loss with anemia, cardiac, or pulmonary disease, 3) ≥ 1,500 mL blood loss, 4) hemoglobin ≤ 7 g/dL, 5) hemoglobin 7–10 g/dL with risk factors of limited oxygenation (e.g., myocardial ischemia, hemodynamic instability), 6) hemoglobin 8–10 g/dL with abnormal cardiac, pulmonary, or cerebrovascular function, 7) hemoglobin < 10 g/dL with bleeding of 750–1,000 mL, 8) cardiovascular disease (e.g., ischemic heart disease, chronic heart failure), 9) clinical condition requiring massive transfusion protocol, and 10) others, RBC = red blood cell, Hb = hemoglobin.
*P < 0.05, **P < 0.01, ***P < 0.001.
![]()
Adverse outcomes were observed in 89 patients (10.1%). In a comparison analysis, the patients with adverse outcomes had significantly older age (≥ 75 years) (86.5% vs. 75.2%; P = 0.017), more patients who received RBC transfusion (52.8% vs. 36.6%; P = 0.003), higher ASA classes (I, II: 23.6% vs. 48.7%, III: 66.3% vs. 46.7%, IV and V: 10.1% vs. 4.7%; P < 0.001), and more bipolar hemiarthroplasty (36.0% vs. 24.0%; P = 0.014) than patients who did not have adverse outcomes (Table 3). In a multivariable logistic regression analysis, RBC transfusion (OR, 1.815; 95% CI, 1.137–2.899; P = 0.013), bipolar hemiarthroplasty (OR, 1.753; 95% CI, 1.073–2.864; P = 0.025), ASA class III (OR, 2.788; 95% CI, 1.622–4.795; P < 0.001), and ASA class IV and V (OR, 4.866; 95% CI, 1.989–11.902; P = 0.001) were significantly associated with adverse outcomes, while post-PBM (OR, 0.557; 95% CI, 0.329–0.944; P = 0.030) was inversely associated with adverse outcomes (Table 4).
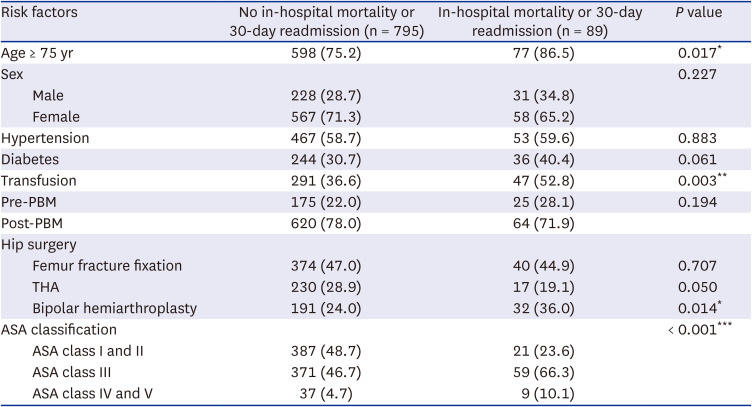
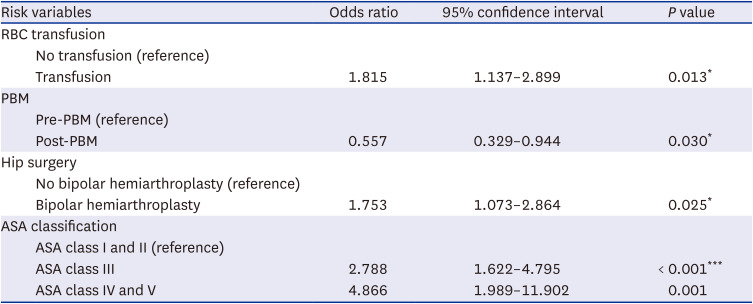
Table 3
Comparison of risk factors for adverse outcomes
Values are presented as frequency (%).
PBM = patient blood management, THA = total hip arthroplasty, ASA = American Society of Anesthesiologists.
*P < 0.05. **P < 0.01, ***P < 0.001.
![]()
Table 4
Multivariable logistic regression analysis of the risk factors associated with adverse outcomes
RBC = red blood cell, PBM = patient blood management, ASA = American Society of Anesthesiologists.
*P < 0.05, **P < 0.01, ***P < 0.001.
![]()
DISCUSSION
This study revealed that the implementing the PBM program for hip fracture surgery decreased perioperative RBC transfusion and significantly increased the appropriateness of RBC transfusion. PBM also significantly decreased the duration of in-hospital stay and the 30-day readmission rate, although there was no significant difference in in-hospital mortality. In particular, the PBM education program and a clinical decision support advisory model to induce restrictive blood transfusion of Hb < 7 g/dL in hemodynamically stable patients with hip fracture are considered to have improved the clinical outcomes.
Restrictive transfusion strategy has played a very important role in the PBM program.1920 This can encourage physicians to audit blood-prescribing practices, which in turn reduces unnecessary blood transfusions. Many studies have reported that restrictive transfusion was not inferior to liberal transfusion in elderly patients with hip fractures.192021 Several studies using the criteria of the American Association of Blood Banks27 have shown that a transfusion threshold of Hb < 8 g/dL is associated with similar or better outcomes than liberal thresholds in patients with hip fractures.2223 Even in elderly patients with high cardiovascular risk, the liberal transfusion strategy did not decrease the inability to walk independently or the mortality at the 60-day follow-up compared with the restricted strategy, nor did it reduce in-hospital morbidity.21 Putot et al.18 reported that transfusion was associated with increased 1-year mortality when the Hb threshold was > 10 g/dL in 3316 consecutive patients aged ≥ 65 years with acute myocardial infarction. However, in patients aged ≥ 80 years with a Hb threshold of < 8 g/dL, transfusion was associated with a 50% reduction in 1-year mortality.18 Amin et al.19 reported that a restrictive threshold of < 7 g/dL Hb in hemodynamically stable patients with hip fractures was associated with less blood utilization and non-inferior perioperative outcomes compared with a threshold of < 8 g/dL. Our study demonstrated that Hb levels prior to RBC transfusion significantly decreased during the PBM periods as a possible consequence of our multifactorial PBM policy. As a result, in a stratified analysis of patients who received blood transfusions, the proportion with Hb levels < 7 g/dL (Hb threshold according to blood transfusion guidelines) increased significantly, while those with Hb levels of 7–10 g/dL decreased significantly. This is considered an important factor in increasing the appropriateness of RBC transfusion in our study.
We found a statistically significant increase in the appropriateness of RBC transfusion in transfused patients. On the contrary, the proportions of the patients who received RBC transfusion significantly decreased. As a possible outcome of our PBM program, the desired result was achieved by increasing the appropriateness of RBC transfusion while decreasing the transfusion rates. Concerning the indications of appropriate transfusion in this study, indication 1 (ongoing bleeding) significantly decreased, and indication 7 (Hb < 10 g/dL with 750–1,000 mL blood loss) increased statistically significantly as PBM progressed. This suggests that, before PBM, transfusions were often performed regardless of the Hb level when bleeding occurred; however, as PBM progressed, transfusion efforts increased only when the Hb level was < 10 g/dL. Educating physicians about the correct indications and potential side effects of transfusion has been shown to reduce the rate of inappropriate transfusions by 40%.282930 In the United States, since 1982, accreditation by the Joint Commission on Accreditation of Hospitals and the College of American Pathologists has required a hospital-based peer-review system to confirm the appropriateness of transfusion therapy.31 However, the National Health Insurance Review and Assessment Service began to evaluate the appropriateness of RBC transfusion for total knee arthroplasty in 2021 for the first time in Korea. Since several studies reported that the multidisciplinary PBM policy improved the appropriateness of RBC transfusion, individual studies according to the type of surgery are likely to be necessary for the future.323334
The current study suggests that the PBM program reduced the adverse outcomes of patients through a decrease in RBC transfusion. The in-hospital stay and 30-day readmission significantly decreased throughout the PBM period. The risk factors for in-hospital mortality or 30-day readmission were age ≥ 75 years, RBC transfusion, bipolar hemiarthroplasty surgery, and a higher ASA class. Multivariable logistic regression analysis demonstrated that RBC transfusion, bipolar hemiarthroplasty, ASA class III, and ASA class IV and V were independent risk factors for adverse outcomes. In this study, the prevalence of ASA class III and IV increased after PBM compared with before PBM because the proportion of severely ill elderly patients increased with the aging of the population. The annual number of hip arthroplasties has increased with the aging of the population worldwide. In Korea, the number of elderly patients undergoing total hip arthroplasty (THA) after a femur fracture has also increased due to an aging population.35 During the 9-year period, the annual incidence of bipolar hemiarthroplasty, primary THA, and revision arthroplasty increased by 47%, 29%, and 3%, respectively.17 Gupta et al.36 reported that after a multifaceted PBM program implementation, the clinical outcomes improved, with decreased 30-day readmissions, morbidity, and composite morbidity or mortality in patients who underwent orthopedic surgery. Amin et al.19 also reported that inpatient cardiac morbidity (from 22.2% to 12.4%) and 30-day readmissions (from 14% to 8.6%) significantly decreased after PBM using restrictive transfusion threshold implementation in 498 patients treated for hip fractures. Carson et al.21 demonstrated that even in 2016 high-risk elderly patients after hip fracture, a liberal transfusion strategy, as compared with a restrictive strategy, did not decrease the death and in-hospital acute coronary syndrome rates on the 60-day follow-up. Therefore, PBM should be actively implemented in elderly patients undergoing hip fracture surgery because appropriate transfusion might improve postoperative outcomes.37
Our study has several limitations. First, because this study was a retrospective analysis, it was challenging to control for issues such as missing data or confounding variables, including cardiovascular risk factors and other potential risk factors associated with bleeding. Although there were no changes in the postoperative venous thromboembolism (VTE) prophylaxis protocol employing low-molecular-weight-heparin prophylaxis along with pneumatic compression mechanical prophylaxis during the study period, underlying diseases of the patients that might affect bleeding or prevent the patients from being placed on the postoperative VTE prophylaxis were not investigated. Therefore, possible confounding effects from unmeasured variables might have influenced our analysis. Second, the rate of single-unit RBC transfusions was not investigated. To reduce unnecessary transfusions, restrictive Hb trigger and single-unit RBC transfusions are recommended if the patients are hemodynamically stable and do not have active bleeding.38 However, in this study, if the transfusion trigger was ≤ 7 at the time of transfusion, it was classified as an appropriate transfusion, even if several RBCs were administered. In the future, it will be necessary to evaluate a more advanced PBM by implementing a “Why give 2 units when 1 unit will do?” campaign to promote single-unit RBC transfusions.
In conclusion, our multidisciplinary PBM implementation improved the appropriateness of RBC transfusions and decreased the RBC transfusion rate in geriatric patients following hip fracture surgery. PBM also improved patient outcomes by reducing the in-hospital stay and 30-day readmission rate. In particular, it is believed that the PBM education program and clinical decision support advisory model to induce restrictive transfusion of Hb < 7 g/dL in hemodynamically stable hip fracture patients improved the PBM effect. In addition, when blood donation has decreased owing to the aging population and the COVID-19 pandemic, PBM may be essential to improve appropriate blood transfusions and patient outcomes by reducing unnecessary blood transfusions.
 XML Download
XML Download