

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
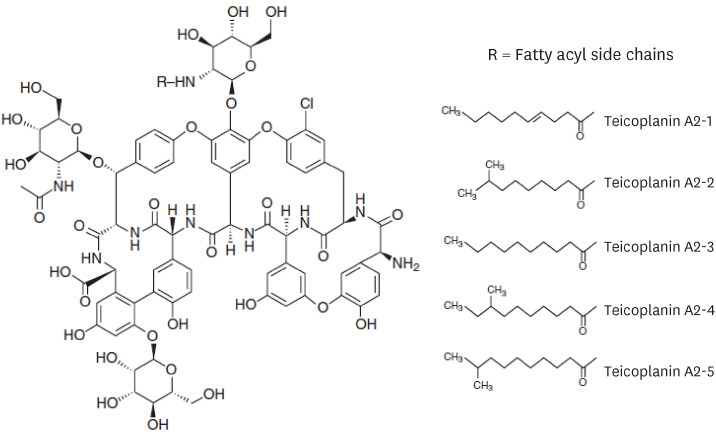
Teicoplanin was produced from Actinoplanes teichomyceticus, isolated in a soil in India in 1978.1 It is available in Europe, Asia, and South America but not in the United States. Teicoplanin is a mixture of glycopeptide analogues with a basic heptapeptide structure consisting of seven aromatic amino acids, the distinct carbohydrates d-mannose and d-glycosamine, and an acyl residue that carries various fatty acids (Fig. 1).2
Fig. 1
Chemical structure of teicoplanin. Source: Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 30, 375-395.
Teicoplanin can be administrated as an intravenous bolus, intermittent infusion, or through the intramuscular route. Similar to vancomycin, teicoplanin is rarely absorbed when administered orally. Approximately 90% of teicoplanin binds to serum albumin, and it is also characterized by its high tissue binding, which may explain its low clearance rate and long half-life, that ranges from 83 to 168 hours. 3 Teicoplanin is renally eliminated, and about 80% of the drug is eliminated in an unchanged form. It is nondialyzable in hemodialysis using high-flux membranes owing to the high protein binding and its large molecular weight (about 1,900 Da); however, significant quantities are removed by continuous venovenous hemodialysis, continuous venovenous hemofiltration, and continuous venovenous hemodiafiltration. 4 The pharmacokinetics (PK) of teicoplanin show a linear dose-serum concentration relationship. The clinical effectiveness associated with the parameter of pharmacodynamic (PD) is associated with the area under the drug concentration-time curve (AUC) during 24 h/minimal inhibitory concentration (MIC). Since it is difficult to obtain multiple serum teicoplanin concentrations to determine the AUC in the clinical setting, trough serum concentration monitoring is used as a surrogate marker for AUC to monitor the teicoplanin levels.5
The guidelines on therapeutic drug level monitoring (TDM) of vancomycin, which belongs to the same glycopeptide category of teicoplanin, for serious methicillin-resistant Staphylococcus aureus (MRSA) have been recently revised.6 The recent guideline recommends using AUC/MIC as a primary PK/PD target for vancomycin, substituting trough-level monitoring which was recommended as a surrogate marker in the former guideline.7 Studies on trough-level monitoring of vancomycin are relatively more abundant compared to teicoplanin, including adverse events or drug reactions related to other antibiotics.8910111213 Due to this relative lack of data, PK/PD monitoring of teicoplanin still relies on trough-level monitoring. The several advantages of teicoplanin compared to vancomycin include longer half-life which allows for once-daily dosing for maintenance therapy, thereby making outpatient parenteral antibiotic therapy possible1415 and lesser adverse events, such as nephrotoxicity, without showing inferiority in terms of clinical efficacy.16 Despite having these advantages, there is no guideline or recommendation for trough-level monitoring of teicoplanin specified to children.
The objective of this study was to review the currently existing studies on teicoplanin PK in pediatric patients, focusing on TDM and clinical efficacy to serve as a guide for clinicians when prescribing teicoplanin during patient care.
METHODS
The systematic review was performed in accordance with the preferred reporting items for systematic reviews.17
Search strategy
We searched PubMed, EMBASE, and Cochrane Library electronic databases using the following terms: (“teicoplanin”) AND (“drug monitoring” OR “drug level” OR “trough” OR “tdm” OR “pharmacokinetics” OR “pharmacodynamics”) AND (“neonate” OR “infant” OR “child” OR “adolescent” OR “pediatric”). We limited the articles to those that were published in English, without any date-wise restrictions. The last search was conducted on August 13, 2021. In addition, the reference lists of included studies and review articles associated with this topic were manually examined to identify any additional relevant articles. The detailed search algorithms used for each database are listed in Supplementary materials.
Eligibility criteria and study selection
Two authors (JSC and SHY) independently assessed the studies retrieved by the search for eligibility. Studies were considered eligible if they reported TDM of teicoplanin in pediatric patients (defined as patients ≤ 18 years of age). Reviews, expert opinions, and animal experiments were excluded. Reports that presented duplicate data and studies with insufficient data were also excluded. If there was a disagreement between the reviewers' assessments, a consensus was reached through discussion.
Data extraction
First, the data on general features included authors’ names, publication year, country of origin, and study design. Second, numbers of participants and their age, gender, body weight, and underlying diseases were extracted. Loading and maintenance dose of teicoplanin, method of TDM (including number and timing), and trough level of teicoplanin were also investigated. Finally, to review clinical aspect, type of infection and identified microorganism, the clinical efficacy (treatment success or failure) of teicoplanin as well as the number of adverse events, such as renal impairment, hepatic impairment and thrombocytopenia from teicoplanin, were determined. Data extraction was conducted and compared by two investigators (JSC and SHY) for consistency.
Assessment of methodologic quality
The validity of the selected studies was independently evaluated by two reviewers (JSC and SHY) using version 2 of Cochrane risk-of-bias tool for randomized trials (RoB 2)18 for the randomized controlled trials, the National Heart, Lung, and Blood Institute Study Quality Assessment Tool19 for case series studies, and the ClinPK Statement20 for the PK studies. Any discrepancies were arbitrated by discussion.
RESULTS
Study characteristics
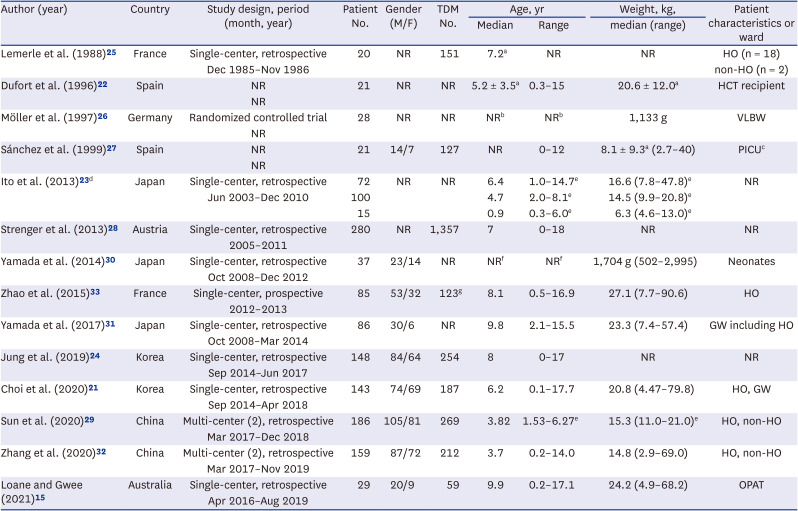
The process of study selection is described in Fig. 2. A total of 226 publications excluding duplicates were extracted from electronic databases. Titles and abstracts were screened, followed by the review of retrieved reports according to the search strategy described above. Sixty-four articles were assessed for eligibility. After a thorough review, 14 articles were finally included for this systematic review.1521222324252627282930313233 Eight studies were single-center-based retrospective studies.1521232425283031 Of the remaining, two were multicenter based retrospective studies,2932 one was single-center-based prospective study,33 and one was controlled trial of which randomization process was not clearly descripted.26 Two studies did not state their study designs.2227 Seven studies were performed in Asia,21232429303132 six were performed in Europe,222526272833 one study was performed in Australia.15 Overall, a total of 1,380 patients from 14 articles were included. TDM was available in 2,739 samples collected in the nine studies.152124252728293233 For patient characteristics, seven studies included hematology/oncology patients. Detailed characteristics of the included studies are described in Table 1.
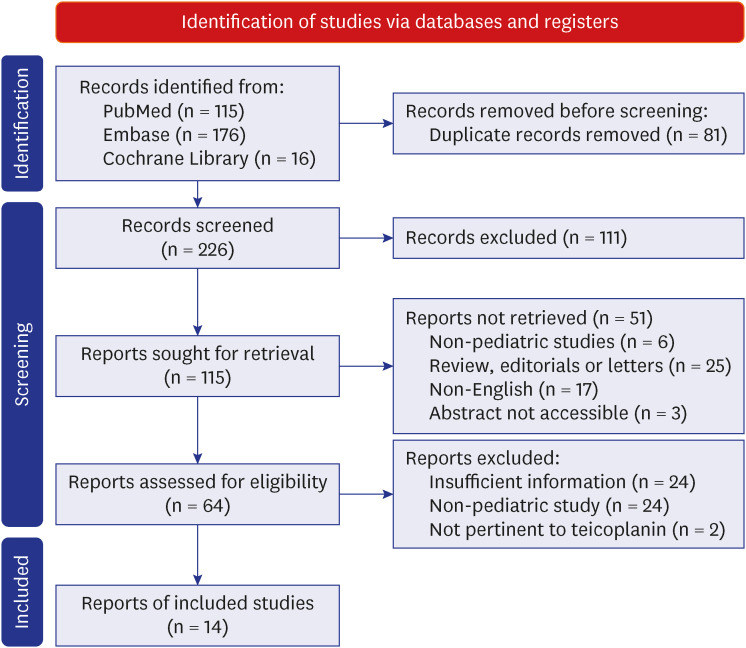
Table 1
General characteristics of studies included
| Author (year) | Country | Study design, period (month, year) | Patient No. | Gender (M/F) | TDM No. | Age, yr | Weight, kg, | Patient characteristics or ward | |
|---|---|---|---|---|---|---|---|---|---|
| Median | Range | median (range) | |||||||
| Lemerle et al. (1988)25 | France | Single-center, retrospective | 20 | NR | 151 | 7.2a | NR | NR | HO (n = 18) |
| Dec 1985–Nov 1986 | non-HO (n = 2) | ||||||||
| Dufort et al. (1996)22 | Spain | NR | 21 | NR | NR | 5.2 ± 3.5a | 0.3–15 | 20.6 ± 12.0a | HCT recipient |
| NR | |||||||||
| Möller et al. (1997)26 | Germany | Randomized controlled trial | 28 | NR | NR | NRb | NRb | 1,133 g | VLBW |
| NR | |||||||||
| Sánchez et al. (1999)27 | Spain | NR | 21 | 14/7 | 127 | NR | 0–12 | 8.1 ± 9.3a (2.7–40) | PICUc |
| NR | |||||||||
| Ito et al. (2013)23 d | Japan | Single-center, retrospective | 72 | NR | NR | 6.4 | 1.0–14.7e | 16.6 (7.8–47.8)e | NR |
| Jun 2003–Dec 2010 | 100 | 4.7 | 2.0–8.1e | 14.5 (9.9–20.8)e | |||||
| 15 | 0.9 | 0.3–6.0e | 6.3 (4.6–13.0)e | ||||||
| Strenger et al. (2013)28 | Austria | Single-center, retrospective | 280 | NR | 1,357 | 7 | 0–18 | NR | NR |
| 2005–2011 | |||||||||
| Yamada et al. (2014)30 | Japan | Single-center, retrospective | 37 | 23/14 | NR | NRf | NRf | 1,704 g (502–2,995) | Neonates |
| Oct 2008–Dec 2012 | |||||||||
| Zhao et al. (2015)33 | France | Single-center, prospective | 85 | 53/32 | 123g | 8.1 | 0.5–16.9 | 27.1 (7.7–90.6) | HO |
| 2012–2013 | |||||||||
| Yamada et al. (2017)31 | Japan | Single-center, retrospective | 86 | 30/6 | NR | 9.8 | 2.1–15.5 | 23.3 (7.4–57.4) | GW including HO |
| Oct 2008–Mar 2014 | |||||||||
| Jung et al. (2019)24 | Korea | Single-center, retrospective | 148 | 84/64 | 254 | 8 | 0–17 | NR | NR |
| Sep 2014–Jun 2017 | |||||||||
| Choi et al. (2020)21 | Korea | Single-center, retrospective | 143 | 74/69 | 187 | 6.2 | 0.1–17.7 | 20.8 (4.47–79.8) | HO, GW |
| Sep 2014–Apr 2018 | |||||||||
| Sun et al. (2020)29 | China | Multi-center (2), retrospective | 186 | 105/81 | 269 | 3.82 | 1.53–6.27e | 15.3 (11.0–21.0)e | HO, non-HO |
| Mar 2017–Dec 2018 | |||||||||
| Zhang et al. (2020)32 | China | Multi-center (2), retrospective | 159 | 87/72 | 212 | 3.7 | 0.2–14.0 | 14.8 (2.9–69.0) | HO, non-HO |
| Mar 2017–Nov 2019 | |||||||||
| Loane and Gwee (2021)15 | Australia | Single-center, retrospective | 29 | 20/9 | 59 | 9.9 | 0.2–17.1 | 24.2 (4.9–68.2) | OPAT |
| Apr 2016–Aug 2019 | |||||||||
M = male, F = female, TDM = therapeutic drug monitoring, HO = hematology or oncology patient, NR = not reported, HCT = hematopoietic cell transplantation, VLBW = very low birth weight, PICU = pediatric intensive care unit, GW = general ward, OPAT = outpatient parenteral antibiotic therapy.
aData reported as mean value only or mean ± standard deviation.
bExact born-age of participants at the point of inclusion was not described in this publication. Mean gestational age was 29.04 weeks with standard deviation of 2.2 weeks.
cCardiac surgery (n = 18), rejection of cardiac transplant (n = 1), heart failure (n = 1), encephalitis (n = 1).
dIn this study, population was divided in three groups (i.e., low, intermediate, high) according to dose of teicoplanin. Overall data were not reported.
eData reported as interquartile range.
fExact born-age of participants at the point of inclusion was not described in this publication. Median gestational age was 30 + 3 weeks, range from 22 + 6 to 40 + 5 weeks.
gA total of 143 teicoplanin concentrations were either drawn for therapeutic drug monitoring (n = 123) or were opportunistic samples (n = 20).
Dose, trough level, and PK
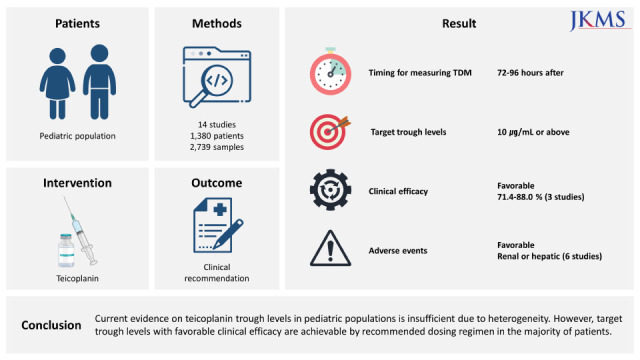
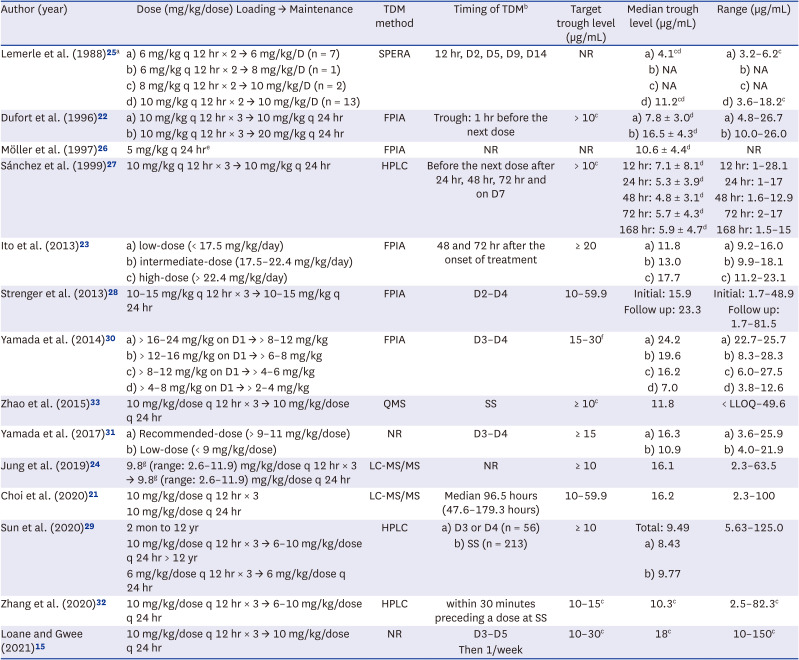
There was a wide range of variety in dosage regimens in included studies, although ten studies had adjusted the generally recommended dosage which consisted of three loading doses every 12 hours and a maintenance dose daily, with each dose of 6 to 10 mg/kg.15212224252728293233 Eight studies adopted recommended dosage for the whole of their study population,1521242728293233 while the other two adopted for the part.2225 The dosage in the remaining studies was divided according to each specific group, and one study arbitrarily chose 5mg/kg/dose as a prophylactic dose.26 The methods used to measure TDM also showed high variability and the most commonly used method was fluorescence polarization immunoassay.2223262830 The timing for measuring TDM also showed variations between the studies, but measured mostly at 72 to 96 hours (steady-state) or longer after the initiation of the first dose.34 The majority of the studies set their target trough levels at 10 µg/mL or higher. Of the ten studies that reported median trough levels, eight reported that teicoplanin levels achieved the pre-defined target. Information on doses and trough levels of teicoplanin is summarized in Table 2.
Table 2
Information on doses and trough levels of teicoplanin in the included studies
| Author (year) | Dose (mg/kg/dose) Loading → Maintenance | TDM method | Timing of TDMb | Target trough level (µg/mL) | Median trough level (µg/mL) | Range (µg/mL) |
|---|---|---|---|---|---|---|
| Lemerle et al. (1988)25 a | a) 6 mg/kg q 12 hr × 2 → 6 mg/kg/D (n = 7) | SPERA | 12 hr, D2, D5, D9, D14 | NR | a) 4.1cd | a) 3.2–6.2c |
| b) 6 mg/kg q 12 hr × 2 → 8 mg/kg/D (n = 1) | b) NA | b) NA | ||||
| c) 8 mg/kg q 12 hr × 2 → 10 mg/kg/D (n = 2) | c) NA | c) NA | ||||
| d) 10 mg/kg q 12 hr × 2 → 10 mg/kg/D (n = 13) | d) 11.2cd | d) 3.6–18.2c | ||||
| Dufort et al. (1996)22 | a) 10 mg/kg q 12 hr × 3 → 10 mg/kg q 24 hr | FPIA | Trough: 1 hr before the next dose | > 10c | a) 7.8 ± 3.0d | a) 4.8–26.7 |
| b) 10 mg/kg q 12 hr × 3 → 20 mg/kg q 24 hr | b) 16.5 ± 4.3d | b) 10.0–26.0 | ||||
| Möller et al. (1997)26 | 5 mg/kg q 24 hre | FPIA | NR | NR | 10.6 ± 4.4d | NR |
| Sánchez et al. (1999)27 | 10 mg/kg q 12 hr × 3 → 10 mg/kg q 24 hr | HPLC | Before the next dose after 24 hr, 48 hr, 72 hr and on D7 | > 10c | 12 hr: 7.1 ± 8.1d | 12 hr: 1–28.1 |
| 24 hr: 5.3 ± 3.9d | 24 hr: 1–17 | |||||
| 48 hr: 4.8 ± 3.1d | 48 hr: 1.6–12.9 | |||||
| 72 hr: 5.7 ± 4.3d | 72 hr: 2–17 | |||||
| 168 hr: 5.9 ± 4.7d | 168 hr: 1.5–15 | |||||
| Ito et al. (2013)23 | a) low-dose (< 17.5 mg/kg/day) | FPIA | 48 and 72 hr after the onset of treatment | ≥ 20 | a) 11.8 | a) 9.2–16.0 |
| b) intermediate-dose (17.5–22.4 mg/kg/day) | b) 13.0 | b) 9.9–18.1 | ||||
| c) high-dose (> 22.4 mg/kg/day) | c) 17.7 | c) 11.2–23.1 | ||||
| Strenger et al. (2013)28 | 10–15 mg/kg q 12 hr × 3 → 10–15 mg/kg q 24 hr | FPIA | D2–D4 | 10–59.9 | Initial: 15.9 | Initial: 1.7–48.9 |
| Follow up: 23.3 | Follow up: 1.7–81.5 | |||||
| Yamada et al. (2014)30 | a) > 16–24 mg/kg on D1 → > 8–12 mg/kg | FPIA | D3–D4 | 15–30f | a) 24.2 | a) 22.7–25.7 |
| b) > 12–16 mg/kg on D1 → > 6–8 mg/kg | b) 19.6 | b) 8.3–28.3 | ||||
| c) > 8–12 mg/kg on D1 → > 4–6 mg/kg | c) 16.2 | c) 6.0–27.5 | ||||
| d) > 4–8 mg/kg on D1 → > 2–4 mg/kg | d) 7.0 | d) 3.8–12.6 | ||||
| Zhao et al. (2015)33 | 10 mg/kg/dose q 12 hr × 3 → 10 mg/kg/dose q 24 hr | QMS | SS | ≥ 10c | 11.8 | < LLOQ–49.6 |
| Yamada et al. (2017)31 | a) Recommended-dose (> 9–11 mg/kg/dose) | NR | D3–D4 | ≥ 15 | a) 16.3 | a) 3.6–25.9 |
| b) Low-dose (< 9 mg/kg/dose) | b) 10.9 | b) 4.0–21.9 | ||||
| Jung et al. (2019)24 | 9.8g (range: 2.6–11.9) mg/kg/dose q 12 hr × 3 → 9.8g (range: 2.6–11.9) mg/kg/dose q 24 hr | LC-MS/MS | NR | ≥ 10 | 16.1 | 2.3–63.5 |
| Choi et al. (2020)21 | 10 mg/kg/dose q 12 hr × 3 | LC-MS/MS | Median 96.5 hours (47.6–179.3 hours) | 10–59.9 | 16.2 | 2.3–100 |
| 10 mg/kg/dose q 24 hr | ||||||
| Sun et al. (2020)29 | 2 mon to 12 yr | HPLC | a) D3 or D4 (n = 56) | ≥ 10 | Total: 9.49 | 5.63–125.0 |
| 10 mg/kg/dose q 12 hr × 3 → 6–10 mg/kg/dose q 24 hr > 12 yr | b) SS (n = 213) | a) 8.43 | ||||
| 6 mg/kg/dose q 12 hr × 3 → 6 mg/kg/dose q 24 hr | b) 9.77 | |||||
| Zhang et al. (2020)32 | 10 mg/kg/dose q 12 hr × 3 → 6–10 mg/kg/dose q 24 hr | HPLC | within 30 minutes preceding a dose at SS | 10–15c | 10.3c | 2.5–82.3c |
| Loane and Gwee (2021)15 | 10 mg/kg/dose q 12 hr × 3 → 10 mg/kg/dose q 24 hr | NR | D3–D5 | 10–30c | 18c | 10–150c |
| Then 1/week |
TDM = therapeutic drug monitoring, q = quaque, SPERA = solid-phase enzyme-receptor assay, D = day, NR = not reported, NA = not analyzed, FPIA = fluorescence polarization immunoassay, HPLC = high-performance liquid chromatography, QMS = quantitative microsphere system, SS = steady state (dosage stable ≥ 72 hours), LLOQ = lower limit of quantification, LC-MS/MS = liquid chromatography-tandem mass spectrometry.
aIn this study, teicoplanin was given twice on the first day then once a day. Arrows refers the change in dose given from the first day of treatment to the second day, not from ‘loading’ to ‘maintenance’, the concept which is widely accepted nowadays.
bDay refers to ‘day of treatment’ in this column.
cData reported as mg/L.
dData reported as mean value only or mean ± standard deviation.
eTeicoplanin was administered as a mean of prophylaxis for sepsis caused by coagulase-negative Staphylococci in this study, not as a treatment of gram positive bacteria.
fAuthors described that it might be possible to set the target trough concentration at ≥ 20 µg/mL for deep-seated infections in neonates.
gData reported as median value.
Clinical efficacy and adverse events
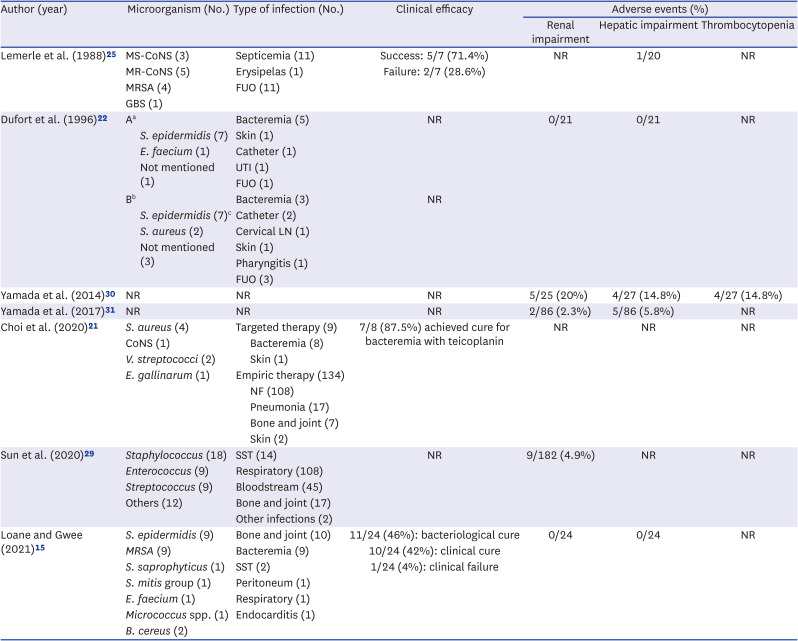
Among 14 studies, seven studies reported clinical efficacy and/or incidence of adverse events (Table 3). Staphylococcus species, including S. aureus and coagulase-negative Staphylococcus (CoNS), was the most cultivated microorganism. Bacteremia was the first or second most common type of infection, where 81 cases of bacteremia were presented in total.
Table 3
Microbiological information and adverse events
| Author (year) | Microorganism (No.) | Type of infection (No.) | Clinical efficacy | Adverse events (%) | ||||
|---|---|---|---|---|---|---|---|---|
| Renal impairment | Hepatic impairment | Thrombocytopenia | ||||||
| Lemerle et al. (1988)25 | MS-CoNS (3) | Septicemia (11) | Success: 5/7 (71.4%) | NR | 1/20 | NR | ||
| MR-CoNS (5) | Erysipelas (1) | Failure: 2/7 (28.6%) | ||||||
| MRSA (4) | FUO (11) | |||||||
| GBS (1) | ||||||||
| Dufort et al. (1996)22 | Aa | Bacteremia (5) | NR | 0/21 | 0/21 | NR | ||
| S. epidermidis (7) | Skin (1) | |||||||
| E. faecium (1) | Catheter (1) | |||||||
| Not mentioned (1) | UTI (1) | |||||||
| FUO (1) | ||||||||
| Bb | Bacteremia (3) | NR | ||||||
| S. epidermidis (7)c | Catheter (2) | |||||||
| S. aureus (2) | Cervical LN (1) | |||||||
| Not mentioned (3) | Skin (1) | |||||||
| Pharyngitis (1) | ||||||||
| FUO (3) | ||||||||
| Yamada et al. (2014)30 | NR | NR | NR | 5/25 (20%) | 4/27 (14.8%) | 4/27 (14.8%) | ||
| Yamada et al. (2017)31 | NR | NR | NR | 2/86 (2.3%) | 5/86 (5.8%) | NR | ||
| Choi et al. (2020)21 | S. aureus (4) | Targeted therapy (9) | 7/8 (87.5%) achieved cure for bacteremia with teicoplanin | NR | NR | NR | ||
| CoNS (1) | Bacteremia (8) | |||||||
| V. streptococci (2) | Skin (1) | |||||||
| E. gallinarum (1) | Empiric therapy (134) | |||||||
| NF (108) | ||||||||
| Pneumonia (17) | ||||||||
| Bone and joint (7) | ||||||||
| Skin (2) | ||||||||
| Sun et al. (2020)29 | Staphylococcus (18) | SST (14) | NR | 9/182 (4.9%) | NR | NR | ||
| Enterococcus (9) | Respiratory (108) | |||||||
| Streptococcus (9) | Bloodstream (45) | |||||||
| Others (12) | Bone and joint (17) | |||||||
| Other infections (2) | ||||||||
| Loane and Gwee (2021)15 | S. epidermidis (9) | Bone and joint (10) | 11/24 (46%): bacteriological cure | 0/24 | 0/24 | NR | ||
| MRSA (9) | Bacteremia (9) | 10/24 (42%): clinical cure | ||||||
| S. saprophyticus (1) | SST (2) | 1/24 (4%): clinical failure | ||||||
| S. mitis group (1) | Peritoneum (1) | |||||||
| E. faecium (1) | Respiratory (1) | |||||||
| Micrococcus spp. (1) | Endocarditis (1) | |||||||
| B. cereus (2) | ||||||||
MS = methicillin-sensitive, MR = methicillin-resistant, CoNS = coagulase negative Staphylococci, MRSA = methicillin-resistant Staphylococcus aureus, GBS = group B Streptococcus, FUO = fever of unknown origin, NR = not reported, S. epidermidis = Staphylococcus epidermidis, E. faecium = Enterococcus faecium, UTI = urinary tract infection, S. aureus = Staphylococcus aureus, LN = lymph node, V. streptococci = Viridans streptococci, E. gallinarum = Enterococcus gallinarum, NF = neutropenic fever, SST = skin and soft tissue, S. saprophyticus = Staphylococcus saprophyticus, S. mitis = Streptococcus mitis, B. cereus = Bacillus cereus, spp. = species.
aA, teicoplanin 10 mg/kg/dose administered as a loading and maintenance dose (n = 9).
bB, teicoplanin 20 mg/kg/dose administered as a loading and maintenance dose (n = 12).
Three studies reported clinical efficacy and the treatment success rates were 71.4%,25 87.5%,21 and 88%,15 respectively. In the study by Lemerle et al.,25 five days were needed to achieve negative blood culture in one patient having septicemia, but this was not designated as treatment failure, and the patient was counted as a success after full recovery.
Adverse events associated with teicoplanin use were described in six studies and focused on renal and/or hepatic impairment.152225293031 No significant relation was noted between the incidence of adverse events and trough concentration in five studies.1522253031 Sun et al. reported that children who were concomitantly treated by amphotericin B or patients with trough level higher than 21.94 mg/L were at high risk for nephrotoxicity.29 A relatively high incidence of adverse events, such as renal impairment, hepatic impairment, and thrombocytopenia, was reported in the study by Yamada et al.30
DISCUSSION
The MRSA infection poses a constant threat in various clinical settings.35363738394041 With the increased incidence of antibiotic resistance and the associated high-risk in pediatric populations, broad-spectrum antibiotics, such as the glycopeptides targeting MRSA, are continuously used in pediatric patients. Therefore, well-summarized PK/PD data for these agents in pediatric patients are highly needed. Our systematic review summarized the TDM of teicoplanin in children and found that among the 1,380 children with teicoplanin target trough levels of 10 µg/mL or above, as reported in the majority of the studies, the average treatment success rate was 82.2%.
Dosing regimen of teicoplanin slightly differs depending on references. For example, summary of product characteristics of teicoplanin by European Medicines Agency recommends that the standard teicoplanin dosing regimen is 10 mg/kg every 12 hours for 3 loading doses followed by a daily maintenance dose of 10 mg/kg in children and 16 mg/kg on day 1, followed by a daily maintenance dose of 8 mg/kg in neonates and infants.42 Generally, three loading doses of 6 to 12 mg/kg/dose every 12 hours and maintenance doses of the same dose as that of each loading dose every 24 hours are recommended in the population older than two months of age. And dosage regimen consisted of a single loading dose of 16 mg/kg on 1st day, followed by a daily single maintenance dose of 8 mg/kg is recommended for neonates and infants up to two months of age. The maximum recommended dose of this drug is 400 mg/dose.43
Among the glycopeptide antibiotics, vancomycin has been widely used for decades to treat MRSA infections in adults and children. Accumulated PK and clinical data rendered vancomycin the treatment of choice for MRSA infection.44 However, its adverse reactions with the associated narrow therapeutic window require careful monitoring of its PK/PD parameters. The first consensus guideline for therapeutic monitoring of vancomycin published in 2009 did not include the pediatric population.7 The revised guideline in 2020 stated that an AUC between 400 and 600 mg × h/L should be the PK/PD target. In addition, trough-only monitoring was no longer recommended in adults and pediatric patients according to the revised guideline.6 Yet, there are ongoing debates on whether this transition to AUC-based monitoring is superior to trough-based monitoring in pediatric patients.945464748
Teicoplanin can be suggested as an effective alternative for vancomycin because of its comparable efficacy and lower adverse event rate.1416 However, the available clinical PK/PD data and recommendations for teicoplanin are relatively fewer than those of vancomycin. Recently, Members of the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring have published clinical practice guidelines for TDM of teicoplanin,49 based on their preceding systematic review and meta-analysis, which included four adult studies.5 The guidelines have suggested practical and useful statements for several clinical issues on teicoplanin TDM. Trough concentration was recommended as a surrogate for AUC/MIC, and initial TDM was recommended to be performed on the fourth day of treatment. Trough concentrations of 15–30 mg/L are recommended for non-complicated MRSA infections, while 20–40 mg/L are recommended for difficult-to-treat complicated infections. Optimizing the dosage regimen to achieve target drug concentration, especially in patients with renal dysfunction, hypoalbuminemia, or continuous venovenous hemodialysis, was also suggested. Most of the reviewed papers in this article deal with adult patients. Pediatric populations were mentioned as candidates for TDM in teicoplanin therapy due to their clinical characteristics, such as their high renal clearance; however, there were no more statements specific to the pediatric patients.
Our study reviewed 14 clinical studies which demonstrated the data on TDM of teicoplanin in the pediatric population. Dosage regimens, method of measuring TDM, time of performing TDM, and target trough levels of teicoplanin showed high variability. Ten studies described a recommended dosage regimen consisting of three loading doses of 6–10 mg/kg over two days and a daily maintenance dose thereafter.15212224252728293233 Six of them achieved the pre-defined target concentrations.152124283233 Additionally, 13 patients who received a dose of 10 mg/kg achieved a mean trough level of 11.2 mg/L.25 Notably, Sánchez et al.27 suggest that the standard dosage of 10 mg/kg/dose might be insufficient for critically ill children. The same issues were raised in adults and the effect of five loading doses (600 mg/dose or 12 mg/kg/dose) on achieving higher trough concentration was reported in this population.5051 However, there is no available data on this regimen in the pediatric population yet. A study to assess a higher loading dose (15 mg/kg/dose) in pediatric patients is registered on Cochrane Central Register of Controlled Trials (https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01888147/full). It is anticipated that this high-loading dose could achieve higher trough concentration, which could also be a target trough level for complicated MRSA infections.
Recent Japanese guidelines recommend performing the initial TDM on the fourth day of treatment before reaching steady state.49 Generally, trough concentration is proposed to be measured after achieving steady-state concentration.34 Because of its long half-life, teicoplanin requires longer time to achieve steady state than vancomycin. This would be a demerit of teicoplanin in serious and complicated infections that might need urgent dosage optimization. Easy-to-access system or rapid on-site equipment which allows frequent TDM could be a countermeasure for the delay in dose optimization. Moreover, model-informed precision dosing could be another alternative.
Our study discloses that teicoplanin is widely used in the various settings of infections caused by gram-positive bacteria other than MRSA. Although teicoplanin was most frequently used in S. aureus infections, it was also used in infections by CoNS, Enterococcus, or Viridans streptococci. Clinical efficacy of teicoplanin was reported in three studies.152125 Amongst them, a regimen of 10 mg/kg/dose achieved nearly 90% of bacterial or clinical cure.1521 Overall adverse reactions of teicoplanin, including nephrotoxicity, hepatotoxicity, thrombocytopenia, were reported as 4.7% (16/338), 5.6% (10/178), and 14.8 (4/27), respectively. Thrombocytopenia was reported only in the study by Yamada et al.30 In a neonatal study, the incidence of reported adverse reactions seemed higher, but the authors considered that the safety of teicoplanin in neonates was comparable with that in adult patients based on references.5253 Together, these data support that teicoplanin could be a good alternative to vancomycin.
Our study has several limitations. First, most of the studies included in this article were observational. Only one study was a controlled trial that evaluated the effect of prophylactic use of teicoplanin for CoNS infection in very-low-birth-weight patients. As prophylaxis using teicoplanin is not a widely accepted practice, and due to its restricted population, the representative nature of this trial for the general pediatric population would be low. Second, due to the wide variability of the treatment regimens, target trough concentration, and reported formats, we could not perform meta-analysis to assess the relationship between dosage and TDM. Third, it was not possible to precisely discriminate between the non-complicated and complicated infections, which might affect the clinical efficacy.
In this systematic review, we have demonstrated that the majority of the study population achieved target trough level with recommended dosage regimen consisting of 3 loading doses and a once-daily maintenance dose, and they also showed good treatment response. Future prospective studies or well-designed randomized controlled trials are needed to address the wide variability and relative lack of data.
 XML Download
XML Download