

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic inflammatory demyelinating polyneuropathy (CIDP) is a relapsing-remitting or progressive immune-mediated acquired neuropathy classified as an autoimmune disorder. CIDP is characterized by a slow and progressive course, with relapsing symptoms and gradual worsening over a period of more than eight weeks.1 CIDP is diagnosed based on clinical features and neurological examination with the help of electrophysiological studies and other supportive findings (Table 1).2 On the other hand, acute inflammatory demyelinating polyneuropathy, also called Guillain-Barré syndrome (GBS), is characterized by a monophasic course, with a clinical peak within four weeks of disease onset.3
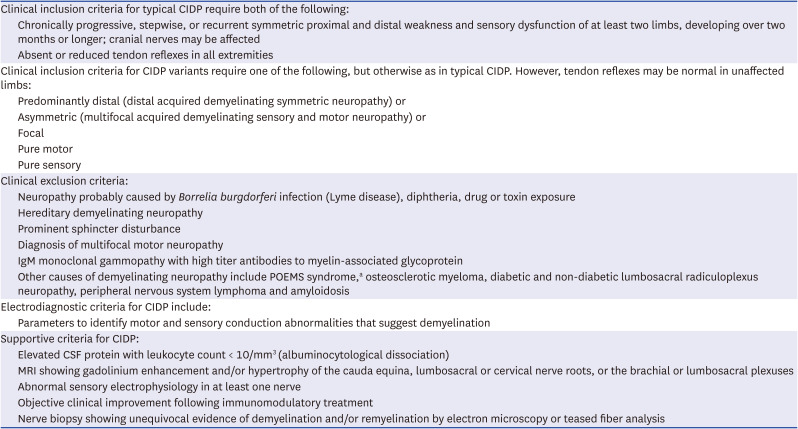
Table 1
European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis of CIDP
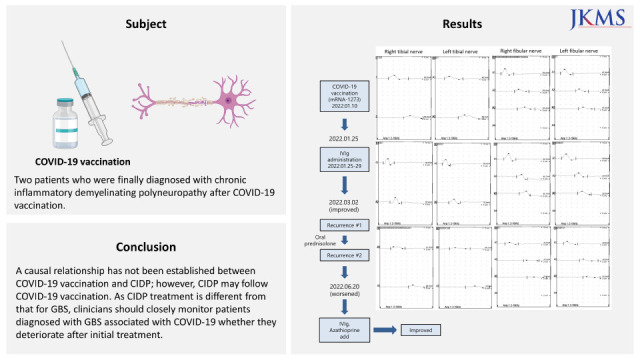
Several immune-mediated neurological diseases have been reported in close temporal relationship with coronavirus disease 2019 (COVID-19) infection or following vaccination against COVID-19.4 The immune-mediated neuropathies related to COVID-19 include GBS, recurrence of GBS, and exacerbation of pre-existing CIDP.5 Although GBS was officially recognized as a complication of COVID-19 vaccines, the causal relationship between new occurrence of CIDP and vaccination against COVID-19 is not yet clear. However, as the pandemic continues, several cases related to these have been reported. In this report, we describe two patients diagnosed with CIDP after COVID-19 vaccination.
CASE DESCRIPTION
Case 1
A 72-year-old man presented with a progressive tingling sensation and weakness below both knees for two weeks. He was vaccinated against COVID-19 with the mRNA-1273 vaccine a month before. As the symptoms progressed, the patient could not walk independently and had difficulty using chopsticks. He had no underlying diseases or recent infection history. He had received the first and the second doses of the BNT162b2 vaccine, which caused no adverse effects. Neurological examinations identified distal dominant limb weakness, deficits of light touch and vibration sensation in the bilateral fingertips and below both knees, and areflexia in all four limbs. Blood tests for polyneuropathy evaluation including complete blood cell counts, liver function tests, renal function tests, serum electrophoresis, thyroid function tests, vitamin B12/folate levels, vitamin D levels, hepatitis marker, anti-Ro/La antibodies, anti-neutrophilic cytoplasmic antibodies, anti-myelin-associated glycoprotein antibody, anti-ganglioside antibodies, and urine tests including urinalysis and electrophoresis revealed no abnormalities. Cerebrospinal fluid (CSF) examination revealed albuminocytological dissociation (white blood cell [WBC] < 5 mm3 [normal range < 5 mm3]; total protein [TP] 72 mg/dL [normal range < 45 mg/dL]). Nerve conduction studies (NCS) revealed demyelinating polyneuropathy (Tables 2 and 36
Fig. 1A-D). Limb weakness and sensory deficits improved after intravenous immunoglobulin (IVIg) treatment, and subsequent NCS showed improved demyelinating polyneuropathy (Tables 2 and 36
Fig. 1E-H). Approximately ten weeks after the onset, he experienced worsened tingling sensation on the feet with gait disturbance, and the following NCS results were aggravated compared with the previous result (Tables 2 and 36
Fig. 1I-L). Under the tentative diagnosis of acute onset chronic inflammatory demyelinating polyneuropathy (A-CIDP), oral prednisolone (30 mg/day) was started, and he felt improvement in the tingling sensation and gait disturbance. However, he complained of aggravated gait disturbance and sensory changes in both feet with the tapering of oral steroids (15 mg/day). Subsequent NCS showed aggravated demyelinating polyneuropathy (Tables 2 and 36
Fig. 1M-P). IVIg and azathioprine were administered with oral prednisolone, which improved his symptoms, except for the mild gait disturbance. The clinical features of this case were recurrent symmetric distal limb weakness, sensory dysfunction, and areflexia at all limbs lasting more than eight weeks. Although GBS was considered as initial diagnosis, we finally considered chronic demyelinating polyneuropathy rather than treatment related fluctuation of GBS because the symptoms progressed for more than 8 weeks and recurred more than 3 times. In addition, other etiologies for chronic polyneuropathy including infection, inflammation, paraneoplastic, metabolic, and toxic causes were excluded, and the symptoms were improved by immune-modulating therapy. The case met the clinical criteria for typical CIDP according to the European Academy of Neurology/Peripheral Nerve Society (EAN/PNS) guideline. The NCS met the demyelinating criteria of motor and sensory nerves, and therefore we diagnosed him as having typical CIDP according to EAN/PNS guideline.
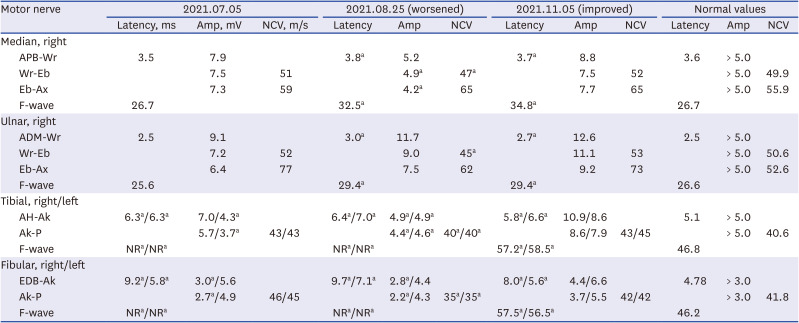
Table 2
Serial nerve conduction studies for case 1: motor nerve (height: 164 cm)
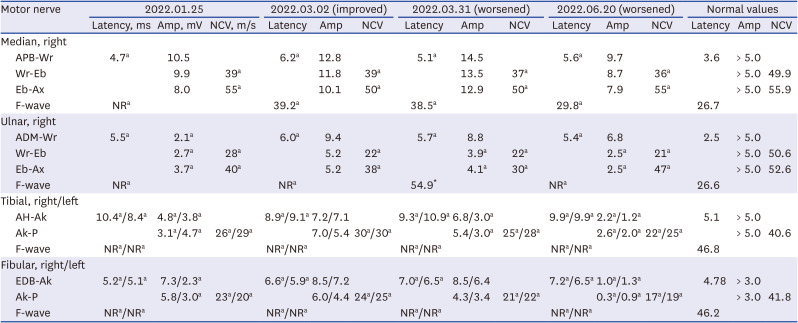
ADM = abductor digiti minimi, AH = abductor halluces, Ak = ankle, Amp = amplitude, APB = abductor pollicis brevis, Ax = axillar, Eb = elbow, EDB = extensor digitorum brevis, NCV = nerve conduction velocity, P = popliteal fossa, Wr = wrist, NR = not recorded.
aIndicates abnormal values.6
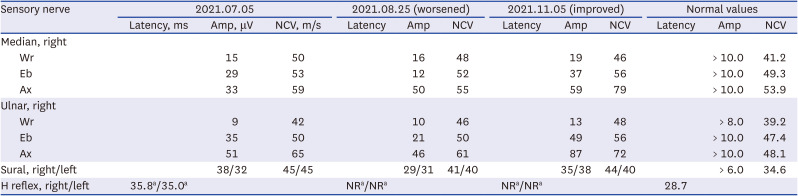
Table 3
Serial nerve conduction studies for case 1: sensory nerve (height: 164 cm)
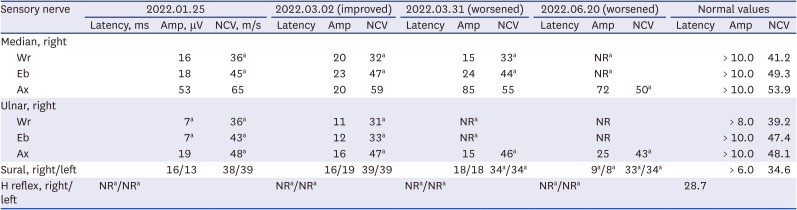
Ax = axillar, Eb = elbow, NCV = nerve conduction velocity, Wr = wrist, NR = not recorded.
aIndicates abnormal values.6
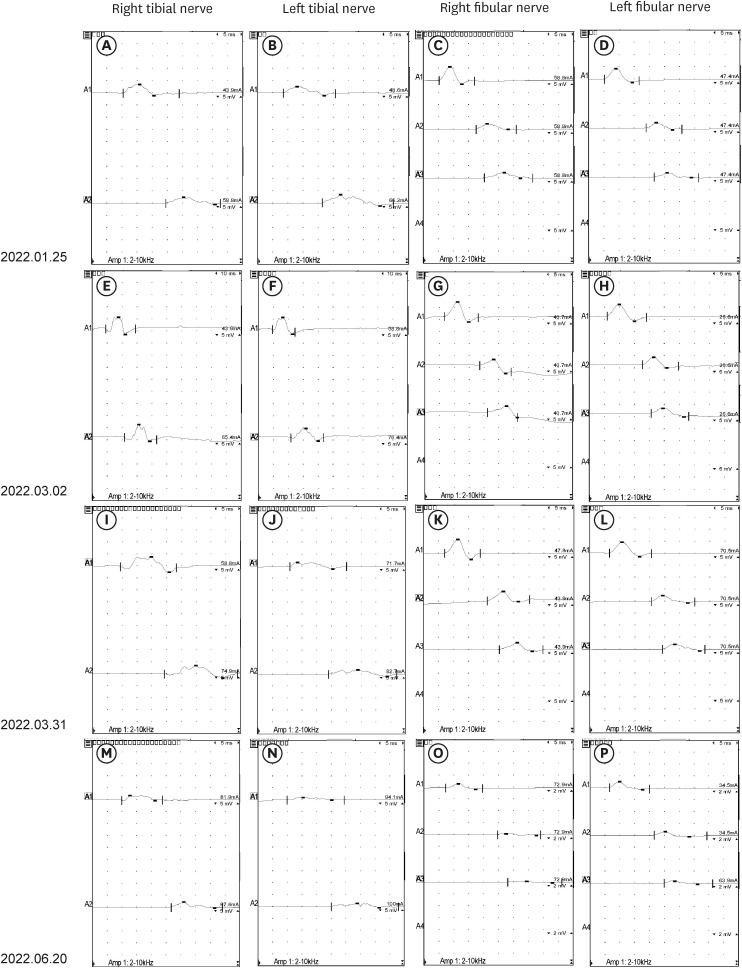
Fig. 1
Waveform of NCS of case 1. (A-D) Initial NCS of bilateral lower extremities: (A) right tibial nerve; (B) left tibial nerve; (C) right fibular nerve; (D) left fibular nerve. (E-H) Second NCS. The demyelinating polyneuropathy were improved after intravenous immunoglobulin administration: (E) right tibial nerve; (F) left tibial nerve; (G) right fibular nerve; (H) left fibular nerve. (I-L) Third NCS. The recurrence occurred: (I) right tibial nerve; (J) left tibial nerve; (K) right fibular nerve; (L) left fibular nerve. (M-P) Fourth NCS. The demyelinating polyneuropathy aggravated after tapering of oral prednisolone (30 → 15 mg): (M) right tibial nerve; (N) left tibial nerve; (O) right fibular nerve; (P) left fibular nerve.
NCS = nerve conduction studies.
Case 2
A 50-year-old man received the first dose of the Ad26.COV2.S vaccine against COVID-19 five weeks prior and experienced a tingling sensation in both legs after a week and gait disturbance three weeks after that. He had hypertension and no recent history of infection. Neurological examinations identified vibration sensation deficits below the ankles, bilateral distal dominant motor weakness on the lower extremities, areflexia, and positive results in the Romberg test. Blood tests including complete blood cell counts, liver function tests, renal function tests, HbA1C, thyroid function tests, hepatitis marker, anti-human immunodeficiency virus antibodies, anti-ganglioside antibodies, antibodies for rheumatologic diseases, vitamin B12/folate levels, serum electrophoresis, tumor marker, paraneoplastic antibodies, and urine tests including urinalysis and electrophoresis revealed no abnormalities. Magnetic resonance imaging (MRI) of brain and whole spinal cord, and positron emission tomography-computed tomography showed no specific findings. Albuminocytological dissociation (WBC < 5 mm3; TP 158 mg/dL) was observed in the CSF analysis, and motor demyelinating polyneuropathy was confirmed in the initial NCS (Tables 4 and 56
Fig. 2A-D). We suspected a case of CIDP because of the progressive symptoms lasting more than four weeks. High-dose oral prednisolone (60 mg/day) was started according to Korean medical insurance guidelines. However, this led to severe tremors and palpitations without improvement. We reduced the dose of oral prednisolone to 15 mg/day and added azathioprine, which partially improved the patient’s symptoms. He complained of persistent gait disturbance and worsened bilateral hand weakness, and serial NCS revealed aggravated demyelinating polyneuropathy 12 weeks after the onset (Tables 4 and 56
Fig. 2E-H). IVIg was administered for two days along with oral prednisolone and azathioprine. His symptoms improved, the motor power and Romberg test results were normalized; and the last NCS showed improvement (Tables 4 and 56
Fig. 2I-L). In this case, the patient had chronic progressive symmetric distal limb weakness, sensory deficits and areflexia in all limbs lasting more than eight weeks, and the results of motor NCS were compatible with demyelinating neuropathy according to EAN/PNS criteria. Although he complained of tingling sensation and sensory ataxia, the NCS of sensory nerves were within normal range. However, the results of the CSF analysis and the response to treatment (especially to corticosteroids) supported a diagnosis of possible typical CIDP. In addition, because no specific findings were observed on the lumbosacral spinal MRI, multiple lumbosacral radiculopathies were excluded as a diagnosis. And the demyelinating features were more clearly identified in NCS performed at the time of recurrence than in initial NCS, which led to the consideration of possible typical CIDP as a diagnosis.
Table 4
Serial nerve conduction studies for case 2: motor nerve (height: 167 cm)
ADM = abductor digiti minimi, AH = abductor halluces, Ak = ankle, Amp = amplitude, APB = abductor pollicis brevis, Ax = axillar, Eb= elbow, EDB = extensor digitorum brevis, NCV = nerve conduction velocity, P = popliteal fossa, Wr = wrist, NR = not recorded.
aIndicates abnormal values.6
Table 5
Serial nerve conduction studies for case 2: sensory nerve (height: 167 cm)
Ax = axillar, Eb = elbow, NCV = nerve conduction velocity, Wr = wrist, NR = not recorded.
aIndicates abnormal values.6
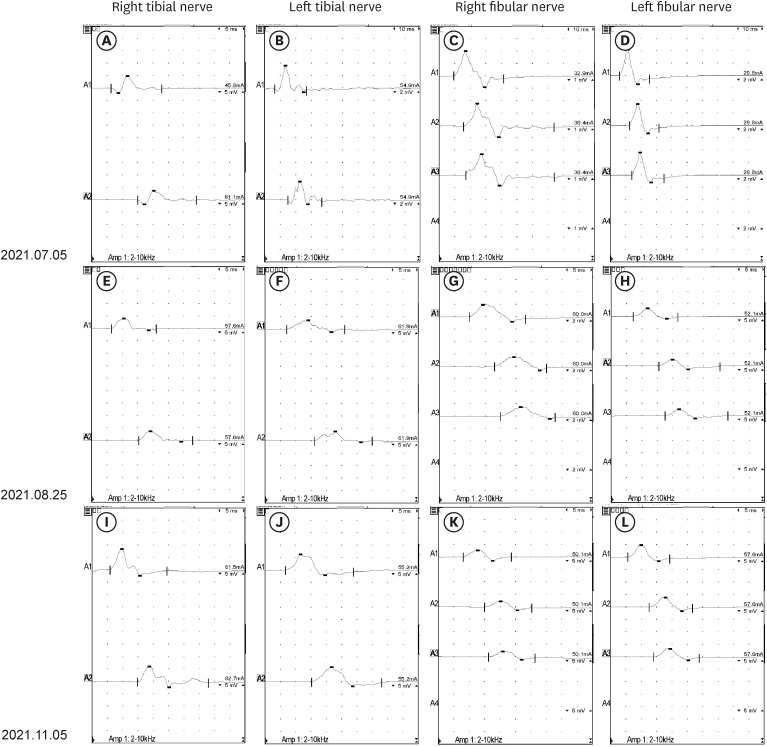
Fig. 2
Waveform of NCS of case 2. (A-D) Initial NCS of bilateral lower extremities: (A) right tibial nerve; (B) left tibial nerve; (C) right fibular nerve; (D) left fibular nerve. (E-H) Second NCS. The demyelinating polyneuropathy aggravated despite of high-dose oral prednisolone: (E) right tibial nerve; (F) left tibial nerve; (G) right fibular nerve; (H) left fibular nerve. (I-L) Third NCS. The demyelinating polyneuropathy were improved after oral prednisolone (15 mg/day), azathioprine, and intravenous immunoglobulin administration: (I) right tibial nerve; (J) left tibial nerve; (K) right fibular nerve; (L) left fibular nerve.
NCS = nerve conduction studies
DISCUSSION
As the pandemic persists, cases of inflammatory neuropathies associated with COVID-19 vaccination are increasingly being reported, and large-scale studies are underway.7 GBS cases have occurred after COVID-19 vaccinations regardless of the type of vaccine (ChAdOx1 nCoV-19 and BNT162b2) in South Korea,8 and GBS was officially recognized as a complication of COVID-19 vaccines in July 2021. The pathomechanism of GBS is associated with the immune response to a preceding infection, which leads to a cross-reaction and causes the production of auto-antibodies directed to epitopes of the myelin sheath or to peripheral nerves and roots.9 The molecular mimicry between microbial proteins or proteins produced by vaccination and the nerve cell surface has been one of the suggested pathophysiologies of GBS associated with COVID-19.
CIDP, which is a type of immune-mediated demyelinating polyneuropathy, has potential to be induced by COVID-19 vaccination, just like GBS. Several cases of CIDP after COVID-19 vaccination have been reported recently. Suri et al.10 reported the case of a 47-year-old male patient diagnosed with CIDP who presented with bilateral limb weakness and facial diplegia after ChAdOx1 nCoV-19 vaccination. Abo-zed et al.11 reported a case of GBS that developed shortly after administration of the mRNA-1273 vaccine and subsequently evolved into CIDP. In Australia, a case series of four patients diagnosed with CIDP was reported by de Souza et al.12 All four patients had received the ChAdOx1 nCoV-19 vaccine before the onset of symptoms. However, there has not yet been multicenter research on the incidence of CIDP after vaccination against COVID-19, or on the association between types of vaccines and CIDP. Also, there have been no reports of the occurrence of CIDP after COVID-19 vaccination in South Korea.
CIDP is an idiopathic condition in which a primarily T cell-mediated immune response is directed against myelin components of peripheral nerves.13 CIDP may be triggered by viruses and vaccines, through mechanisms triggering self-reactive T cell and cytokine upregulation that may induce MHC class II expression.14 The cases reported here had been vaccinated with two types of vaccine with different mechanisms. mRNA-1273 is an mRNA vaccine containing instructions for expressing a SARS-CoV-2 protein, but it does not contain the virus and prepares the body to defend itself against COVID-19.15 On the other hand, vaccines such as Ad26.COV2.S and ChAdOx1 nCoV-19 are modified adenovirus vector vaccines. Virus vector vaccines have a higher transmission rate of genes within the cell than mRNA vaccines, and they cause natural infection and require a stronger immune response compared to an mRNA vaccine. Many neurological diseases such as GBS have been reported after administration of adenovirus vector vaccines.10121617 However, the mRNA vaccine may also cause various neurological diseases, including immune-mediated neuropathies. There have been 383 reports of GBS in the UK following vaccination with ChAdOx1 nCoV-19, and 42 reports following the BNT162b2 vaccine.15 In South Korea, a series of 13 GBS cases following COVID-19 vaccination was reported. Of the 13 patients, eight had received ChAdOx1 nCoV-19, and five had received the BNT162b2 vaccine.8 In addition to GBS, a case of CIDP after vaccination with mRNA-1273 vaccine was reported.18 The pathomechanisms underlying the association between CIDP and specific vaccines against COVID-19 are not well known, but CIDP seems to occur in response to various types of COVID-19 vaccines.
The treatments for GBS and CIDP are quite different. Therefore, it is important to distinguishing CIDP from other demyelinating neuropathies, including GBS. In GBS, IVIg is administered for a short period, without maintenance treatment. On the other hand, oral corticosteroids or steroid-sparing immunosuppressants have been used as treatment for CIDP. However, A-CIDP is difficult to distinguish from GBS. If symptoms improve after IVIg administration and then worsen for more than eight weeks, the possibility of A-CIDP should be considered. Maintenance treatment for CIDP should be initiated without delay in A-CIDP. The first of the cases was considered A-CIDP, because the patient had been experiencing recurrences three times, with more than eight weeks from the onset of symptoms.
Herein, we summarize the first reported cases of a new occurrence of CIDP following vaccination against COVID-19 in South Korea. These cases indicate that COVID-19 vaccination may be a possible trigger factor for CIDP as well as for GBS. Although a causal relationship has not been established between COVID-19 vaccination and CIDP, CIDP may follow COVID-19 vaccination, regardless of different mechanisms of action. As CIDP treatment is different from that of GBS, clinicians should closely monitor patients with GBS associated with COVID-19 whenever they deteriorate after initial treatment.
 XML Download
XML Download