

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic is ongoing. The high transmissibility of current dominant variants of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the complications of severe illness in the high-risk population remain major concerns. Antiviral agents are an important therapeutic option against severe COVID-19 in addition to vaccination. Remdesivir is the first antiviral approved for SARS-CoV-2 therapy.1 However, the intravenous infusion of remdesivir is a barrier against easy access and widespread use. Due to the increased health care burden posed by COVID-19, some countries have suffered medical collapse and collateral damage from diseases other than COVID-19.23 Effective oral antiviral agents may allow improved access to specific treatments and better clinical outcomes. Recently, two oral antiviral agents, nirmatrelvir/ritonavir and molnupiravir, began to be used for treatment. In addition to their reported clinical efficacy, antiviral agents are expected to decrease the viable viral burden from the respiratory tract and thus lower transmission.
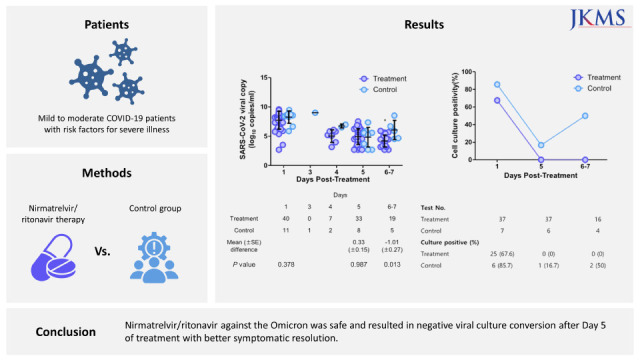
Nirmatrelvir is an oral antiviral agent that can inhibit 3-chymotrypsin-like cysteine protease enzyme, which is essential for the replication of SARS-CoV-2.4 Coadministration with ritonavir, a cytochrome P3A4 inhibitor, enhances nirmatrelvir pharmacokinetics. Nirmatrelvir/ritonavir (Paxlovid) showed an 89% lower risk or progression to severe COVID-19 than a placebo without major safety concerns and reduced the viral load by 0.868 log10 copies per milliliter compared with the placebo group at Day 5 of treatment.5 Recent retrospective studies showed clinical effectiveness of nirmatrelvir/ritonavir for reducing severe COVID-19 and mortality especially in high-risk patients such as aged 65 years or older.6789 Nirmatrelvir/ritonavir has also been approved in Korea for emergency use within five days of COVID-19 symptom onset, and the clinical indication is mild to moderate COVID-19 patients with risk factors for severe illness.10 This study assessed the clinical and virologic responses to oral nirmatrelvir/ritonavir in mild to moderate COVID-19 patients with risk factors for severe illness in a real-world setting.
METHODS
Study design
This was a prospective observational study conducted for mild to moderate COVID-19 patients without oxygen demand who presented within five days of illness onset, were aged ≥ 19 years and had one or more risk factors for severe illness. SARS-CoV-2 infection was confirmed with reverse transcription polymerase chain reaction (RT-PCR) and patients were recruited from the biocontainment units of four hospitals (Seoul Metropolitan Government-Seoul National University Boramae Medical Center, National Medical Center, Seoul Medical Center, and Seoul Veterans Hospital Medical Center) in Korea from February to April 2022. Patients who needed oxygen therapy at presentation, had a history of antiviral treatment targeting COVID-19 or had the first dose of nirmatrelvir/ritonavir over eight hours prior were excluded. The risk factors for severe illness included aged 60 years or older; immunocompromised status such as active chemotherapy for malignancy, hematopoietic stem cell transplantation, primary immunodeficiency, solid organ transplantation, human immunodeficiency virus infection, autoimmune diseases requiring disease-modifying anti-rheumatic drugs, functional or anatomical asplenia, or immunosuppressive therapy including high dose corticosteroids, tumor-necrosis factor blockers and biologic agents; aged 40 years or older combined with chronic underlying diseases such as diabetes mellitus, cardiovascular diseases, chronic kidney diseases, chronic lung diseases, obesity with body mass index over 30 kg/m2 or neurodevelopment diseases.
The subjects were divided into treatment and control groups. The treatment group was treated with oral nirmatrelvir/ritonavir, which was administered based on the clinical decision of attending physicians.11 Although the investigators also played a role as the physician, the physician in charge was not always the investigator of this study. In such cases, interventions regarding the medication or laboratory tests were minimized. The control group included patients who were indicated for but not treated with nirmatrelvir/ritonavir. Patients with clinical improvement could be discharged before the obligatory isolation period of seven days from the initial diagnostic test, and the need for further hospitalization was determined based only on the clinical decision. The primary outcomes were the difference in viral load and the proportion of negative culture conversion between Days 1 and 5 following nirmatrelvir/ritonavir administration. The secondary outcomes were the proportion of adverse reactions and clinical responses such as symptom resolution overall or during hospitalization and new oxygen requirement within 28 days.
Clinical effectiveness
The treatment group received nirmatrelvir/ritonavir every 12 hours for five days in addition to symptomatic supportive care. The baseline characteristics of patients, including age, sex, body mass index (BMI), underlying comorbidities, COVID-19 vaccination status, time of symptom onset, and confirmed date of COVID-19, were recorded. We defined ‘fully vaccinated’ as a condition of the three doses (two doses in the case of the Janssen vaccine) or status within two weeks after the second dose (first dose in the case of the Janssen vaccine). Clinical severity was measured using the National Early Warning Score 2 (NEWS2).12 The worst value on Day 1 was used to estimate the scoring variables. Clinical symptoms for effectiveness were assessed every day during hospitalization and 28 days after beginning nirmatrelvir/ritonavir. On Day 28, patients were contacted via telephone and interviewed regarding their clinical symptoms and the need for additional hospital visits after discharge. Clinical symptoms were categorized as respiratory and non-respiratory symptoms. If the patient was asymptomatic during the study period, the first day when all symptoms were resolved was collected. Clinical signs, such as noninvasive oxygen saturation and body temperature, were checked daily during the isolation period. Fever was defined as a body temperature of 37.8°C or higher. Clinical outcomes, including oxygen requirement and mortality, were also observed. Prescriptions of other medications for COVID-19, such as monoclonal antibodies, remdesivir, corticosteroids, and antibiotic agents, were recorded if relevant.
Adverse reactions
The occurrence of adverse reactions, which was described according to the Common Terminology Criteria for Adverse Events version 6.0, was assessed daily during the nirmatrelvir/ritonavir treatment period.13 In case of an adverse reaction event, the treatment method for the adverse reaction and the decision to discontinue nirmatrelvir/ritonavir were recorded. Laboratory values for complete blood tests, liver function tests, renal function tests, coagulation profiles and inflammatory markers were collected on Days 1 and 5 (± 2 days), if necessary, in response to a suspicion of adverse effect or clinical changes.
Viral load and culture positivity
Serial nasopharyngeal (NP) swabs from both sides were collected at three time points as follows: Day 1 before taking nirmatrelvir/ritonavir or within 8 hours after taking the first dose, Day 5, and Day 7 (± 1 day). The second of third samples were independently performed of the first swab time on a daily basis. If the patient was discharged earlier, the samples from Day 5 or Day 7 were collected earlier and the last sample was collected on the day of discharge. The detection and quantification of SARS-CoV-2 were performed using a real-time reverse transcription polymerase chain reaction assay (rRT-PCR) of the E and ORF1ab genes (PowerCheck™ SARS-CoV-2 RT-PCR; KogenBiotech, Seoul, Korea). The RNA genome copies were calculated based on cyclic threshold values using calibration standard curves from quantified ORF1ab or E gene-generated SARS-CoV-2 RNAs. Viral genotypes of SARS-CoV-2 variants were determined using the PowerCheck™ SARS-CoV-2 S-gene Mutation Detection Kit version 3.0 (KogenBiotech).
The viral culture was performed in a biosafety level-3 laboratory of the Korea National Institute of Health (Osong, Korea). Briefly, filtered swab samples were inoculated into a monolayer of Vero E6 cells (1.5 × 105 cells per well) in 24-well plates that were prepared one day earlier, and the inoculated cells were maintained for one hour at 37°C and 5% CO2 with rocking every 15 minutes. After removal of the inoculum, cells were incubated with 1 mL of Dulbecco’s modified Eagle’s medium supplemented with 2% fetal bovine serum and penicillin-streptomycin. The cytopathic effect (CPE) of the inoculated cells was observed daily using a light microscope for seven days after inoculation. The CPE-positive cells were investigated for viral replication using rRT-PCR targeting the ORF1ab and E genes on the day of observation, and the CPE-negative cells were assessed at seven days post-inoculation. The supernatants of all CPE-positive and CPE-negative inoculated cells were passaged and investigated for viral replication using the rRT-PCR method.
Statistical analysis
A χ2 test, Fisher’s exact test, and Student’s t-test were performed to compare the clinical data from the treatment and control groups. The proportion of subjects with symptom resolution or oxygen requirement during hospitalization was calculated. Viral quantification was compared using a one-way analysis of variance (ANOVA). The viral load of the 2nd specimen included only those of Day 5 and those assessed on Day 3 or Day 4 were excluded from the analysis. However, if the culture result was negative each day, the results were reflected as negative on Day 5. The proportion of positive to negative conversion in SARS-CoV-2 viral culture between the two groups was compared using the Kaplan-Meier method. Statistical significance was set at P < 0.05. All statistical analyses were performed using SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA).
Ethics statement
All study participants provided informed consent. This study was approved by the Institutional Review Board (IRB) of Seoul Metropolitan Government-Seoul National University Boramae Medical Center (IRB No. 30-2022-11). The study was performed in accordance with the ethical standards of the Declaration of Helsinki.
RESULTS
Baseline characteristics
During the study period 2,629 patients with confirmed COVID-19 were admitted to the study sites. Fifty-three patients who were clinically indicated for nirmatrelvir/ritonavir and consented to participate in the study were enrolled. Two participants who collected only one sample were excluded from the analysis. The major reasons for non-eligibility for the initial screening were severe illness at presentation, disability to consent, non-high-risk group and symptom onset over five days. A total of 40 patients in the treatment group and 11 patients in the control group were subjected to the final analysis (Table 1, Fig. 1). The control group were not administered the nirmatrelvir/ritonavir due to mild symptoms (6 patients), underlying conditions such as hepatic dysfunction (4 patients) and possible drug interaction (1 patient) by patient’s own or physician's decision. However, one patient with maintenance hemodialysis was administered the nirmatrelvir/ritonavir by a physician’s clinical decision and registered in the study without final clinical aggravation or adverse event. On average, patients were 68 years old in the treatment group and 69 years in the control group. The proportion of male patients was 50.0% in the treatment group. Ninety-six percent of the patients had at least one underlying disease. The proportion of patients with hypertension was higher in the treatment group than in the control group (52.5% vs. 9.1%, P = 0.015). The median Charlson Comorbidity Index was three in both groups. In the treatment and control groups, the proportions of fully vaccinated patients were 75.0% and 81.8%, while three and one patients were never vaccinated, respectively. The median durations from symptom onset to Day 1 of nirmatrelvir/ritonavir treatment or supportive care were two and three days, respectively, while the median NEWS2 scores were 0.5 and 0.0 (P = 0.399), respectively.
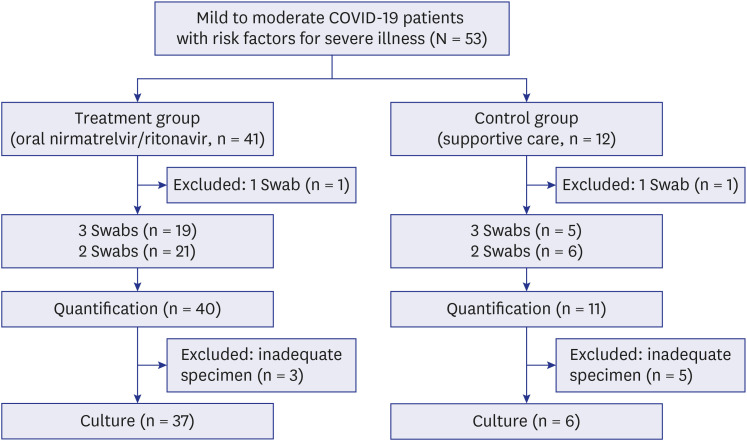
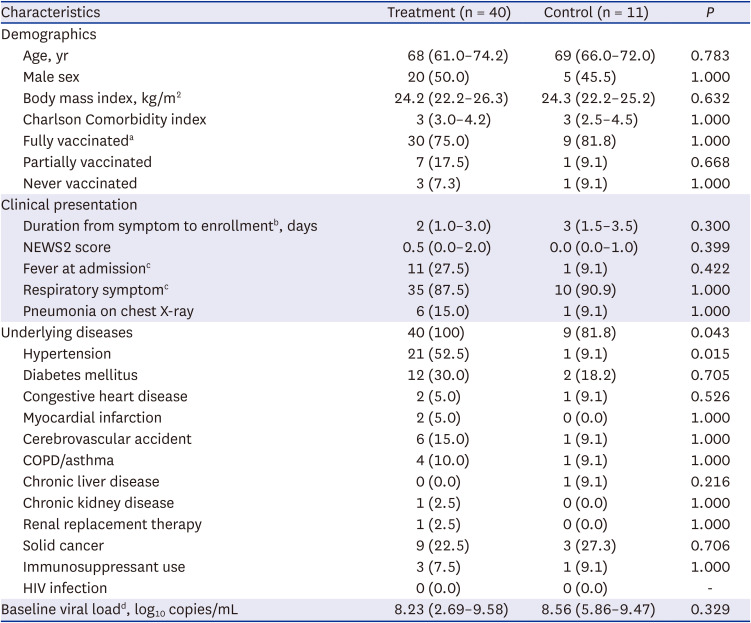
Fig. 1
Study design. The subjects were recruited and allocated into treatment and control groups in four hospitals from February to April 2022.
COVID-19 = coronavirus disease 2019.
![]()
Table 1
Baseline characteristics of the study participants receiving oral nirmatrelvir/ritonavir (treatment group) and supportive care only (control group)
Values are presented as median (interquartile range) or number of patients (%).
NEWS = National Early Warning Score, HIV = human immunodeficiency virus, COPD = chronic obstructive pulmonary disease.
aFully vaccinated indicates a condition of the 3rd booster dose or status within two weeks after the 2nd dose of vaccine against COVID-19 (the 2nd and 1st dose for Janssen vaccine, respectively).
bEnrollment indicates the first day of nirmatrelvir/ritonavir administration or the first day of control group allocation.
cFever is defined as a body temperature of 37.8°C or higher. Respiratory symptoms included sore throat, cough, increased sputum, and shortness of breath.
dValues are expressed as median (range).
![]()
Clinical response to oral nirmatrelvir/ritonavir
Fever was observed in 27.5% and 9.1% of patients (P = 0.422), and 87.5% and 90.9% of patients reported respiratory symptoms in the treatment and control groups, respectively. All patients except one in the treatment group who discontinued nirmatrelvir/ritonavir on Day 5 due to potential drug interaction with the current tacrolimus treatment completed the five-day medication schedule. The proportion of patients with symptom resolution within 28 days was 51.3% vs. 36.4% (P = 0.501) in the treatment and control groups, respectively (Table 2). However, the proportion of patients with complete symptom resolution during the admission period was higher in the treatment group than in the control group (30.0% vs. 0%, P = 0.048). Oxygen supply was required in one patient in each group at 2.5% vs. 9.1% (P = 0.388). No mortality was observed in either group. The proportion of patients using corticosteroids or antibiotics was the same for both groups, and none of the patients used monoclonal antibody therapy or tocilizumab. Remdesivir was used in two patients in the control group, and both patients were treated for five days starting on Day 3 and Day 2, respectively, as symptoms persisted during supportive care.
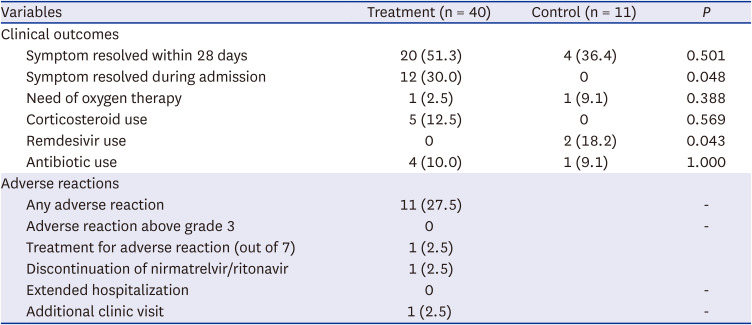
Table 2
Clinical outcomes and adverse reactions in the treatment and control groups
![]()
A total of 11 patients (27.5%) in the treatment group experienced adverse reactions as follows: gastrointestinal symptoms, including nausea, vomiting, diarrhea, constipation and greenish stool (5 patients), dysgeusia (7 patients), chest discomfort (1 patient), and leukocytosis (1 patient). However, no patient reported grade 3 or 4 adverse reactions. Most patients were followed-up without specific treatment for adverse reactions, and none of the subjects discontinued nirmatrelvir/ritonavir. Laboratory test data were collected from 27 patients (21/40 in the treatment group and 6/11 in the control group). One patient in the treatment group reported leukocytosis (20,300/mm3) on Day 5, which was caused by Klebsiella pneumoniae bacteremia.
Viral load and culture positivity
The genotyping of the samples from 51 patients of both groups revealed all omicron subvariants with 12 of BA.1 and 38 of BA.2 except one untypable sample. The serial viral loads were measured in 40 patients in the treatment group (21 patients with 2 time-point specimens and 19 patients with 3 time-point specimens) and in 11 patients in the control group (6 patients with 2 time-point specimens and 5 patients with 3 time-point specimens). The mean viral load at Day 5 by the E gene was reduced by 2.80 log10 copies/mL (from 7.73 to 4.93 log10 copies/mL) in the treatment group. It was further reduced to 4.19 log10 copies/mL on Day 7, which was significantly lower than that of the control group (P = 0.013) (Fig. 2). The ORF1ab gene change showed similar trends (P = 0.118).
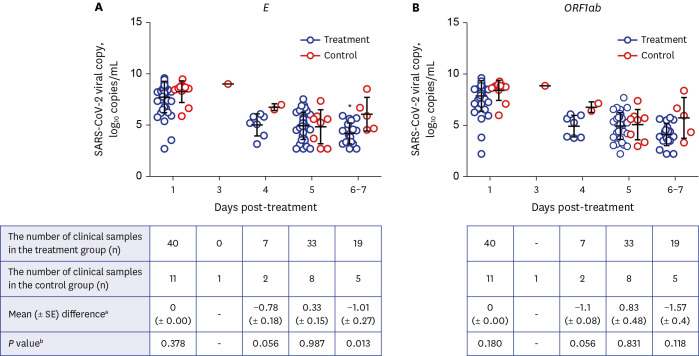
Fig. 2
Distribution of SARS-CoV-2 viral load in the treatment and control groups. (A) SARS-CoV-2 E gene, (B) SARS-CoV-2 ORF1ab gene. The number of patients who had nasopharyngeal swabs by day after the start of treatment in the treatment and control groups is indicated respectively. The cyclic threshold value for SARS-CoV-2 on each day was statistically compared between the treatment and the control groups.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
aThe differences between the mean values of viral RNA copies of the treatment group samples and the control group samples.
bStatistical significance of the viral RNA copies measured from the treatment group samples, compared with those measured from the control group samples at each designated day after treatment.
![]()
Viral culture was performed in 37 of 40 patients in the treatment group and 6 of 11 patients in the control group. In the treatment group, the conversion rate from the initial positive culture to a negative culture was 100% on Day 5 (25/25). The other 12 patients all showed persistent negative culture results from baseline Day 1 to the last serial samples. In the control group, only three patients (3/6, 50.0%) exhibited final negative culture conversions until Day 7, and 2 patients were culture negative on Day 5 and reverted to culture-positive again on Day 7. Positive reversion was not observed in the treatment group. When the survival analysis was performed only for the patients whose culture was positive on baseline Day 1, the nirmatrelvir/ritonavir treatment significantly increased the culture negative conversion of SARS-CoV-2 from the upper respiratory tract during the seven-day period after medication (P = 0.004) (Supplementary Fig. 1).
In the subgroup analysis for the 30 fully vaccinated patients in the treatment group and nine in the control group, the difference in the viral load decrease for the E gene (P = 0.629 on Day 1, P = 0.927 on Day 5, and P = 0.020 on Day 7) and ORF1ab gene (P = 0.433 on Day 1, P = 0.927 on Day 5, and P = 0.038 on Day 7) was significant on Day 7 (Fig. 3). The proportion of initial positive cultures in the treatment group (21/27) was converted to zero (100%, 21/21) on Day 5. However, it was 50.0% (3/6) in the control group. The relative risk of negative conversion was significantly different after adjusting for the vaccination status (P = 0.001).
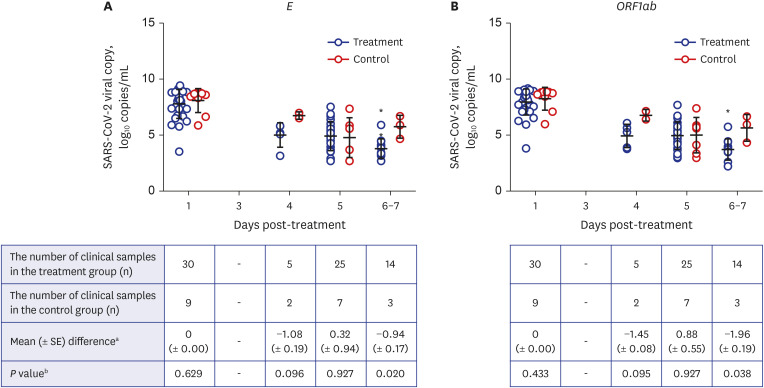
Fig. 3
Distribution of SARS-CoV-2 viral load of fully vaccinated patients in the treatment and control groups. (A) SARS-CoV-2 E gene, (B) SARS-CoV-2 ORF1ab gene.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
aThe differences between the mean values of viral RNA copies of the treatment group samples and the control group samples.
bStatistical significance of the viral RNA copies measured from the treatment group samples, compared with those measured from the control group samples at each designated day after treatment.
![]()
DISCUSSION
Our study showed that oral nirmatrelvir/ritonavir therapy against the omicron variant of SARS-CoV-2 in a real-world setting exhibited tolerable safety profiles and comparable clinical effectiveness with the EPIC-HR study5 and changed the viral kinetics to shorten the duration of viable viral shedding from the upper respiratory tract. The decrease in viral load on Day 5 after five days of oral nirmatrelvir/ritonavir did not differ, however, this was lower in the treatment group on Day 7 (P = 0.002). The proportions of viral culture positivity were 67.6% (25/37) vs. 85.7% (6/7) on Day 1, 0% (0/37) vs. 16.7% (1/6) on Day 5, and 0% (0/16) vs. 50.0% (2/4) on Day 7 in the treatment and control groups, respectively. The nirmatrelvir/ritonavir decreased the viral load of SARS-CoV-2 faster and the viable virus was undetectable after Day 5.
Several studies reported that the duration of culturable viral shedding of SARS-CoV-2 shedding from the upper respiratory tract and the related variables differed in terms of dominant genotypic variants, clinical severity of patients, status of COVID-19 vaccination, types of upper respiratory specimens, and immune status.1415161718 Generally, the number of subjects was small (18 to 66 patients) and antiviral therapy was not used. The median duration of culturable viral shedding in the untreated patients was four to seven days from the onset of symptoms or date of laboratory diagnosis. Although it was reported that the period of viral shedding was shorter in vaccinated individuals than in never or only partial vaccines.17 Another study reported shedding of omicron variants in vaccinated individuals for six to nine days after symptom onset.18 In our study, subgroup analysis with only fully vaccinated patients indicated that the vaccination did not make any significant difference in viral shedding in the omicron variant. However, as the proportion of not fully vaccinated patients was 25.0% (10/40) vs. 18.2% (2/11) in the treatment and control groups, the small number might limit the interpretation considering a previous report that suggested differences between vaccinated and unvaccinated patients. 19 Our study showed that culture results from 32.4% (12/37) of baseline specimens with a median of two days from the onset of symptoms were negative. Another study reported negative culture results in 29% (4/14) of baseline upper respiratory specimens.14 This agrees with the US CDC guideline citing the short major transmission period around the onset of symptoms.20
The detection of replication-competent SARS-CoV-2 is the most reliable indicator of contagiousness.21 However, it is still unclear whether the identification of culturable SARS-CoV-2 is consistent with transmittable disease; therefore, the collection of more clinical data is necessary. Evidence has shown that PCR assays can detect SARS-CoV-2 much longer after the short period of viable SARS-CoV-2 shedding, the isolation period has been shortened to five to seven days according to the policy of each country.2022 If antiviral therapy can further shorten the period of active viral shedding, the isolation period may also be changed. Since antiviral therapy for COVID-19 in Korea is indicated for high-risk groups, including immunocompromised patients, the duration of isolation may be more individualized. Viable SARS-CoV-2 could be observed even after two months or more in immunocompromised patients, such as those who received allogeneic hemopoietic stem-cell transplants, therefore, the host factor must be considered for individualization.23
The basic characteristics of the two groups in our study were similar except for a higher proportion of hypertension (52.5% vs. 9.1%, P = 0.015), and the symptoms during hospitalization resolved faster (30.0% vs. 0%, P = 0.048) in the treatment group. The need for oxygen therapy and mortality did not differ between the two groups. Adverse reactions to oral nirmatrelvir/ritonavir were reported in 27.5% of patients. Nirmatrelvir/ritonavir demonstrated effective clinical responses along with the absence of major safety concerns in the EPIC-HR trial.5 The viral genotype infecting all subjects in our study was confirmed to be the omicron variant. The omicron variant has been reported to be highly sensitive to nirmatrelvir in vitro.24 Moreover, nirmatrelvir retained its effect in vitro for the omicron sublineage.25 The Delta variant was primarily observed in the participants of the EPIC-HR trial, therefore, our results provide further evidence that nirmatrelvir demonstrated efficacy against the omicron variant in vivo. The viral rebound phenomenon needs to be mentioned; viral rebound during or shortly after nirmatrelvir/ritonavir therapy in vaccinated immunocompetent individuals was previously suggested.26 Although its definition is not yet clear and the frequency of the rebound phenomenon does not seem to be a frequent occurrence, further data are needed to better understand this process. This may be an indicator of the incomplete effectiveness of five-day nirmatrelvir/ritonavir therapy, which warrants longer therapy.
Our study has several strengths. This was a prospective study that assessed the viral decay kinetics in terms of PCR-based viral quantification and culture methods. We used bilateral NP swabs to stably collect upper respiratory tract specimens. Few studies have assessed viable viral shedding after nirmatrelvir/ritonavir therapy, and the confounding of results by mixture or uncertainty of viral variants was minimized by only using the omicron variant. Our study also has limitations. First, this study was conducted with a small sample size, which limits precision. Second, we could not obtain the baseline serology for SARS-CoV-2 at the time of infection. As the epidemic curve of COVID-19 had been small in Korea before 2022, the possibility of reinfection in the study subjects was estimated to be low. Third, the first NP swabs at Day 1 were collected after the first dose of nirmatrelvir/ritonavir in 17 patients, which may influence the baseline Day 1 result in the treatment group. The initial culture positivity might be underestimated due to the effect of first dose in those patients. However, the baseline viral load did not differ between the two groups (Fig. 2), the time lapse after the first dose was a median three hours (interquartile range, 1.6–4.0), and a second or third NP swab was performed independently of the first swab time. Thus, the first dose of nirmatrelvir/ritonavir could not influence the later swabs and main results. Finally, although the NP swabs were planned on Days 1, 5, and 7, there were some deviations for earlier sampling. The clinical improvement of patients before Day 5 after oral nirmatrelvir/ritonavir treatment led to earlier discharge, resulting in an earlier NP swab for the last sample. To minimize the bias, we separately analyzed Days 4 and 5, and the main comparative analysis was performed for Day 5. Day 6 and 7 samples were analyzed together as one point because those time points occurred shortly after the completion of nirmatrelvir/ritonavir and the earlier discharge of patients was not infrequent as stated above.
In conclusion, oral nirmatrelvir/ritonavir therapy against the omicron variant was safe and resulted in negative viral culture conversion from Day 5 with better symptomatic resolution in mild- to moderate-high-risk COVID-19 patients. This may have implications for the isolation period of nirmatrelvir/ritonavir-treated COVID-19 patients.
 XML Download
XML Download