

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the first case of it was reported in Wuhan, China, in December 2019, coronavirus disease 2019 (COVID-19) spread rapidly worldwide, and on March 11, 2020, the World Health Organization (WHO) declared it a pandemic.1 According to the WHO, COVID-19 affected 227 countries and caused more than 500 million confirmed cases and 6 million deaths as of April 2020.2 Since the first case of COVID-19 in South Korea (hereafter referred to as “Korea”) was reported on January 19, 2020, four waves have appeared in the country (as of April 2022), with over 16 million cumulative confirmed cases, which account for about 31% of the entire population (51.6 million).
To combat COVID-19, the Korean government installed the Central Disaster and Safety Countermeasures Headquarters and implemented coping strategies, such as social distancing measures of different levels, restrictions on the number of people allowed at private gatherings, the introduction of the vaccine pass, a mandatory self-quarantine for close contactors, and the monitoring of arrivals from abroad. However, the persistent COVID-19 crisis has had a disruptive economic impact, which has increased fatigue among the population, affecting their mental health and leading to, for example, post-traumatic stress disorder and increased levels of stress, depression, and fear, among another conditions.34
According to the Community Health Survey in Korea, in 2019 and 2020, the prevalence of depression in the Korean population has decreased from 6.0% in 2019 (pre-COVID-19) to 5.8% in 2020.5 However, a previous study conducted in Korea during the COVID-19 pandemic found that 34.2% and 28.8% of 1,000 respondents experienced symptoms of at least mild depression and anxiety, respectively, thereby, demonstrating an increase in the rates of depression and other mental health disorders compared with the pre-COVID-19 levels.6 According to a U.S. study, 40.9% of respondents reported at least one adverse mood symptom due to the COVID-19 pandemic.7 A deterioration in mental health is likely to cause fear, in addition to stress and depression, which can in turn affect mental and physical activity leading to sleep disturbances, reduced physical activity, and loss of motivation.8 According to a previous study conducted in Korea, physical activity decreased (49.6%), sleep time decreased (9.4%), and intake of junk food increased (17.0%) in daily life of participants owing to COVID-19.9
Following are some of the main causes of the increased fear of contracting COVID-19: an increase in the number of confirmed cases, reduced trust in the government, and stringent policy measures such as lock-downs.10111213 Korea has been heading towards a record-high peak since the COVID-19 outbreak began, with more than 600,000 new cases reported each day in the first quarter of 2022. In this situation, the fear of COVID-19 infection (hereafter referred to as “COVID-19 phobia”) will inevitably increase.14 In 2020, the Korean government began to implement various policies to ease restrictions associated with COVID-19, such as “with COVID-19,” “relaxation of social distancing measures,” and “abolition of vaccine passes”.15 Under these circumstances, a fifth wave of COVID-19 is expected to sweep the country in the second half of 2022 along with further deterioration of the mental health of the entire population.16
The Korean government is moving towards a gradual easing of COVID-19-related restrictions to return to pre-COVID-19 life. One of the relaxation measures that is being gradually implemented is the normal operation of schools at the primary, secondary, and post-secondary levels. Most Korean universities provide online classes that comply with the social distancing directives. However, with the prospect of the normal operation of schools, starting from the second half of 2022, a negative impact on students’ COVID-19 phobia is to be expected. A study found that students’ COVID-19 phobia was associated with commuting to school and spending time with others at school.17 Consequently, the need-of-the-hour for the Korean government is to identify factors affecting COVID-19 phobias among university students and to take these factors into account to strategize new policy directives for the ongoing process of returning to normalcy in university education.
This study aimed to identify the current state of COVID-19 phobia among Korean undergraduate and graduate students and the factors affecting it. Specifically, four objectives were pursued: 1) identifying the current state of Korean university students’ COVID-19 phobia; 2) identifying factors affecting COVID-19 phobia.
METHODS
Study design
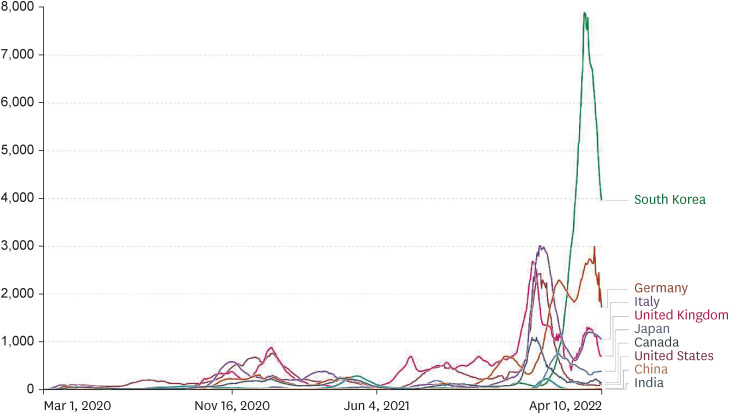
This cross-sectional survey was conducted to identify the factors affecting COVID-19 phobia among Korean undergraduate and graduate students. The survey was conducted from April 5 to April 16, 2022, and the targeted respondents were undergraduate and graduate students enrolled in Korean universities. During the survey period, the average number of newly confirmed cases of COVID-19 in Korea 5,500 per million people, which was higher than that in any other country in the world (Fig. 1).
Data sample and data collection
The minimum sample size required for this study was calculated using G*Power 3.1. F-test statistics were calculated from hypothesis testing, and a multilinear regression model with nine independent variables was used for the statistical analysis, which was performed at a 95% confidence interval and ± 5% error range. Therefore, the minimum sample size required for this study was 172. The target area of the survey was the entire country, and care was taken to ensure that a balanced number of respondents were included from all regions.
The survey was conducted online to avail geographic, temporal, and economic advantages, as well as to ensure infection prevention, considering that it was during the fourth wave of the COVID-19 outbreak. One university each in Gangwon-do, Daejeon, Busan, and Jeonju were selected as joint research universities to have a balanced distribution of respondents from across Korea and, undergraduate and graduate students attending the above universities were surveyed. Survey participants in each university were selected using non-probability random sampling because of the nature of the online survey. More specifically, respondents were recruited first by convenience sampling, and then, they completed an online survey. A non-face-to-face online survey was conducted under the supervision of a professor and a co-researcher in each department using the Google survey tool, through which a URL link to an online questionnaire was delivered to the respondents. A written consent form was included on the first page of the online questionnaire, and respondents could sign and select “I agree” to proceed if they consented. They could then share the URL link with the next set of target respondents according to the sampling design.
Study instrument
The questionnaire used in this study was the COVID-19 Phobia Scale (C19P-S) modified to suit the research purpose (Supplementary Table 1).18 The C19P-S consists of 25 items rated on a 5-point Likert scale, totaling 100 points. The 25 items were grouped into four subscales: psychological (6 items, 30 points), psychosomatic (5 items, 25 points), social (5 items, 25 points), and economic (4 items, 20 points). The validity and reliability of the C19P-S as a psychometric instrument have been established in Korea.1920
To identify the factors affecting COVID-19 phobia, respondents’ characteristics were examined in from four aspects: general characteristics, COVID-19 infection, COVID-19 policy, and COVID-19 prevention behaviors.
We examined sex (male/female), region of residence (Seoul, Gyeonggi, Incheon, Gangwon-do, Gyeongsang-do/Busan, Jeolla-do/Gwangju, and Chungcheong-do/Daejeon), and household type (living alone/living with family/friends). COVID-19 infection was examined by assessing the experience of COVID-19 infection symptoms (yes/no).
In this study, the independent variables “efficiency of social distancing” and “personal opinion on COVID-19 mitigation policy” were selected to understand the impact of opinions regarding COVID-19 policies on fear. The variable—“efficiency of social distancing”—was evaluated with the question, “Do you think the current government-led social distancing policy is efficient?” and the respondents could answer with “inefficient” or “efficient.” The variable—“personal opinion on COVID-19 mitigation policy” —was evaluated with the question, “Do you agree with the current government announcement on country-level mitigation policies on with COVID-19?” and the respondents could respond with “agree” or “disagree.”
“Avoidance of crowded places,” “mandatory mask wearing,” “adherence to social distancing,” and “adherence to indoor ventilation” were selected as independent variables in order to understand the degree of influence for the level of COVID-19 prevention on fear of COVID-19. The characteristics of COVID-19 preventive behaviors were the avoidance of crowded places (no/yes), mandatory mask wearing (no/yes), adherence to social distancing (no/yes), and adherence to indoor ventilation (no/yes). The final version of the questionnaire was completed after its reliability and validity were validated through a preliminary survey of 36 students.
Statistical analysis
This study aimed to identify the factors affecting COVID-19 phobia among Korean undergraduate and graduate students. To this end, the following analyses were performed. First, an independent-samples t-test was used to determine the differences in the levels of COVID-19 phobia depending on the independent variables. Second, an independent-samples t-test was used to evaluate the differences among the independent variables in the four subscales of the C19P-S. Third, to identify the factors affecting COVID-19 phobia, multiple linear regression was performed with five models constructed by classifying the dependent variable into five components: the total C19P-S score (Model 1) and the psychological (Model 2), psychosomatic (Model 3), social (Model 4), and economic (Model 5) subscores. The correlations between the independent variables, goodness of fit, and explanatory power of these five models were analyzed and validated using a multicollinearity analysis, F-test, and adjusted R2, respectively. The statistical analyses were conducted using IBM SPSS 26.0 (IBM Corp., Armonk, NY, USA), and the data were visualized using the GraphPad PRISM 9 software (GraphPad Software, Boston, MA, USA).
Ethics statement
All components of this survey were approved by the Institutional Review Board (IRB) of Yonsei University in Korea (IRB document number: 1041849-202204-SB-078-01). Written informed consent was obtained from all respondents prior to the data collection being initiated. Specifically, we drew attention to respondents’ right to refuse the survey request on the first page of the online survey form.
RESULTS
Demographic characteristics of the study population (N = 460)
A total of 460 undergraduate and graduate Korean students responded to the online questionnaire survey administered to achieve the purpose of the study (Table 1). The respondents’ general characteristics were analyzed as follows: women far outnumbered men (72.6 vs. 27.4%); the region of residence was distributed in the order of Seoul/Gyeonggi/Incheon (32.2%), Gyeongsang-do/Busan (25.2%), Jeolla-do/Gwangju (18.7%), Gangwon-do (17.6%), and Chungcheong-do/Daejeon (6.3%); and living with family/friends accounted for 85.0% of the respondents. Regarding the characteristics pertaining to COVID-19 infection and its mitigation policy, 65.2% of respondents had tested positive for COVID-19 92.4% found social distancing measures to be inefficient, and 64.8% agreed with the government’s COVID-19 mitigation policy. In regard to the COVID-19 prevention behaviors, 46.1% of respondents answered that they avoid crowded places, and the percentages of those who comply with mandatory mask wearing, social distancing, and regular indoor ventilation were 95.9%, 88.0%, and 73.3%, respectively.
Table 1
Characteristics of the respondents (N = 460)
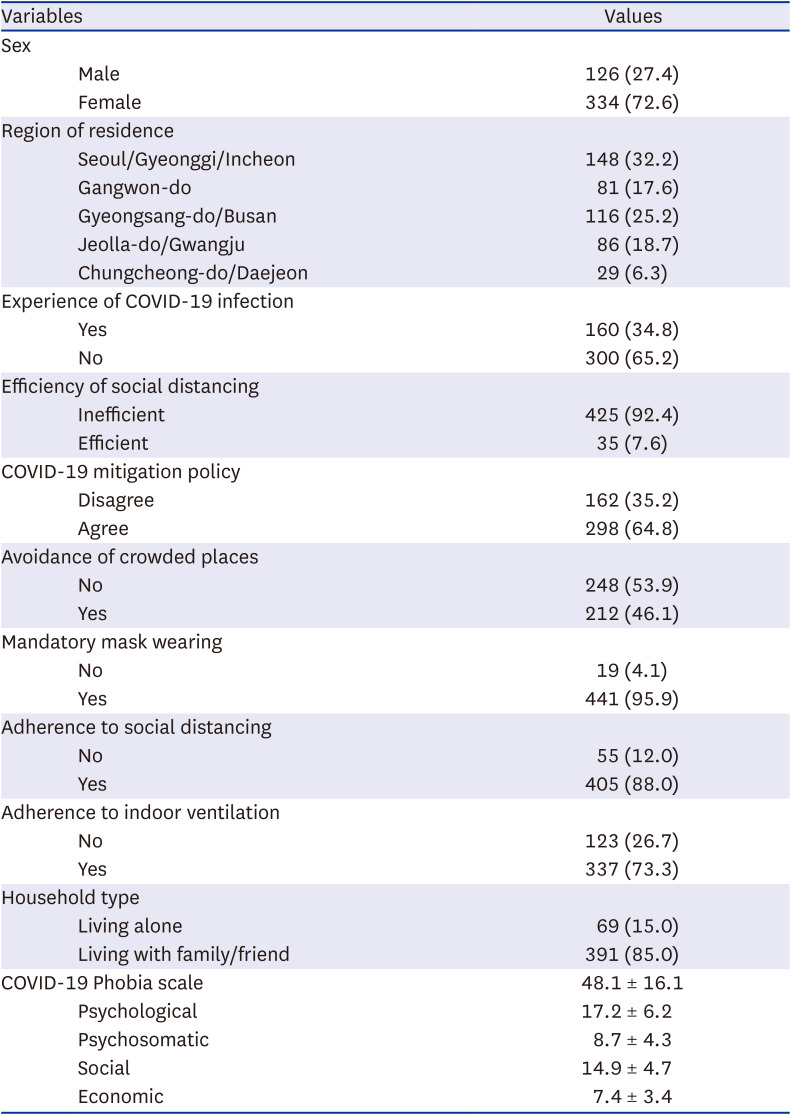
The mean C19P-S score for the respondents was 48.1 points out of a total of 100 points, and this consisted of the four subscale scores as follows: psychological = 17.2 (out of 30); psychosomatic = 8.7 (out of 25); social = 14.9 (out of 25); and economic = 7.4 (out of 20).
Evaluation of the differences in the C19P-S scores
For the purpose of this study, we measured the COVID-19 phobia using the C19P-S scores; additionally, we evaluated the differences in the scores according to respondents’ characteristics using an independent-samples t-test. The C19P-S score (total score: 100 points) consists of the psychological (30 points), psychosomatic (25 points), social (25 points), and economic (20 points) subscales (Table 2, Fig. 2). The mean C19P-S score for the respondents was 48.1/100 points, and the four subscale scores (mean values) as follows: psychological = 17.2/30; psychosomatic= 8.7/25; social =14.9/25; and economic = 7.4/20.
Table 2
Evaluation of differences in COVID-19 phobias according to respondent characteristics
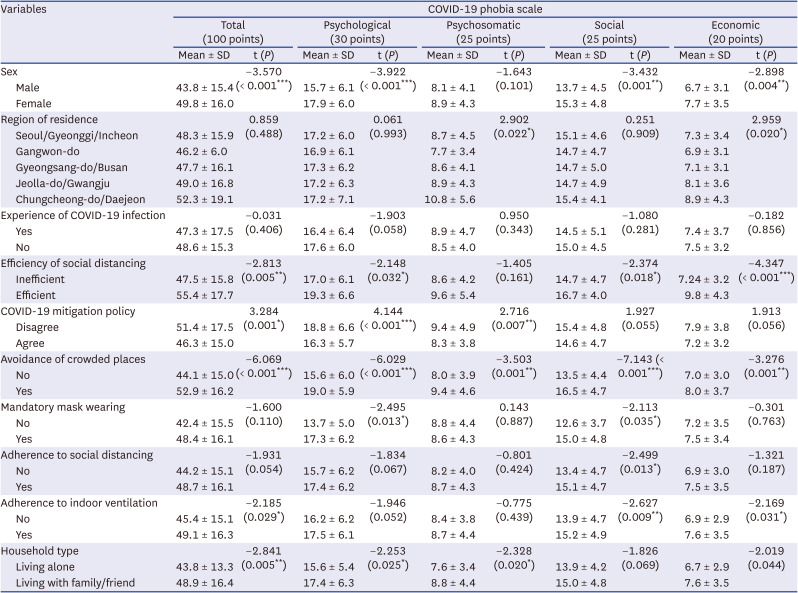
Fig. 2
COVID-19 Phobia Scale used in this study.
COVID-19 = coronavirus disease 2019.
*P < 0.05; **P < 0.01; ***P < 0.001.
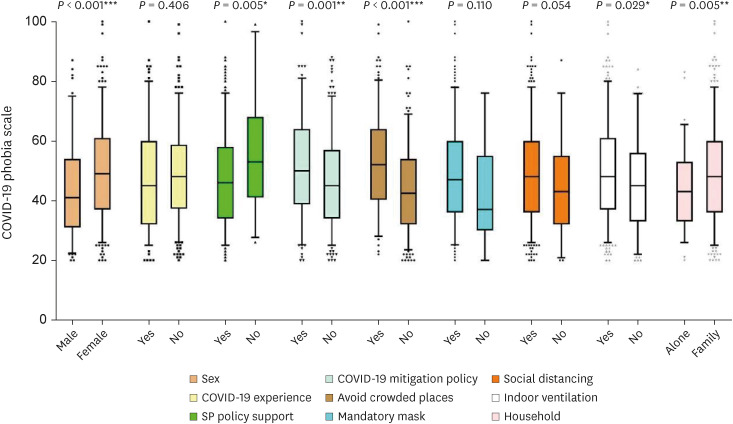
The analysis of the test of differences in the C19P-S scores by the respondent characteristics revealed that women far-outscored the men (P < 0.001), with significant differences in the psychological (P < 0.001), social (P = 0.001), and economic (P = 0.004) subscale scores. In the evaluation of the differences by region of residence, only the psychosomatic subscale scores showed a significant difference (P = 0.022). No statistically significant difference was observed in the C19P-S scores with respect to previous history of being tested positive for COVID-19.
Differences in the participants’ characteristics pertaining to the government’s COVID-19 mitigation policy were analyzed to assess the differences in the levels of COVID-19 phobia according to the government policy. The analysis revealed that the respondents who considered social distancing efficient had a significantly higher mean C19P-S score (P = 0.005) than those who considered it inefficient. By subscale scores, phobia was observed to be significantly higher in the psychological (P = 0.032), social (P = 0.018), and economic (P < 0.001) subscales. Respondents who disagreed with COVID-19 mitigation policy exhibited significantly higher psychological (P < 0.001) and psychosomatic (P = 0.007) subscales scores than those who agreed with it.
Among the characteristics of COVID-19 prevention behaviors, significantly higher COVID-19 phobia was demonstrated by respondents avoiding crowded places (P < 0.001) and those adhering to regular indoor ventilation (P = 0.029).
Analysis of the factors affecting COVID-19 phobia
We performed multiple linear regression to identify the factors affecting COVID-19 phobia in Korean undergraduate and graduate students (Table 3). Multiple linear regression was performed on the C19P-S scores using five models with the following dependent variables: (Model 1) total C19P-S score (total score: 100 points), (Model 2) psychological subscale score (30 points), (Model 3) psychosomatic subscale score (25 points), (Model 4) social subscale score (25 points), and (Model 5) economic subscale score (20 points). The fit of these five models was established, with the P value of each test statistic (F test) being less than 0.05.
Table 3
Results of multiple linear regression analysis of COVID-19 phobia scale scores
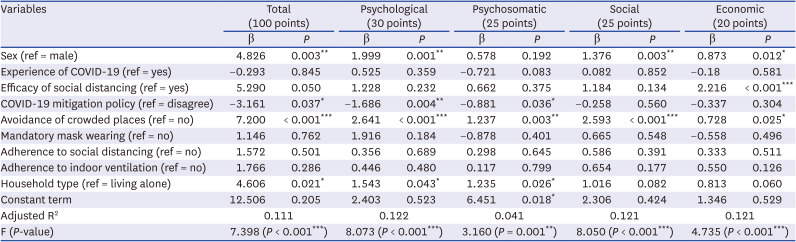
An analysis of the factors affecting the total C19P-S score (Model 1) led to the following findings: women significantly outscored men (difference: 4.826 points, P = 0.003); the group that favored the government’s COVID-19 mitigation policy scored significantly lower than those who did not favor it (difference: 3.161 points, P = 0.037); the group that avoided crowded places scored significantly higher than the group that did not avoid crowded places (difference: 7.200 points, P < 0.001); and those living with family/friends scored significantly higher than those in other living situations (difference: 4.606 points, P = 0.021).
It is worth noting that the group that avoided crowded places had significantly higher mean C19P-S scores than the group that did not avoid crowded places in all five models and that the variables “COVID-19 mitigation policy” and “living with family/friends or alone” had significant effects on the psychological and psychosomatic subscale scores, whereas the variable “efficiency of social distancing” had a significant effect on the economic subscale score.
The COVID-19 phobia (psychological) score (Model 2) showed significantly higher psychological fear in women than men, by 1.999 points (difference: 1.999 points, P = 0.001). Those in favor of the COVID-19 mitigation policy had a significantly lower psychological fear than those who were against it, by 1.686 points (difference: −1.686 points, P = 0.004). Psychological fear was also significantly higher for those who avoided crowded places compared to those who did not, by 2.641 points (difference: 2.641 points, P < 0.001). Furthermore, fear was significantly higher in people cohabitating than those living alone, by 1.543 points (difference: 1.543 points, P = 0.043).
The COVID-19 phobia (psychosomatic) score (Model 3) showed that psychological fear was significantly lower in those in favor of the COVID-19 mitigation policy than those who were against it, by 0.881 points (difference: −0.881 points, P = 0.036). Psychosomatic fear was significantly higher in respondents who avoided crowded places compared to those who did not, by 1.237 points (difference: 1.237 points, P = 0.003). Furthermore, psychosomatic fear was significantly higher in people cohabitating than those living alone, by 1.235 points (difference: 1.235 points, P = 0.026).
The COVID-19 phobia (social) score (Model 4) showed that social fear was significantly higher in respondents who avoided crowded places compared to those who did not, by 2.593 points (difference: 2.593 points, P < 0.001).
The COVID-19 phobia (economic) score (Model 5) showed that economic fear was significantly higher in women than in men, by 0.873 points (difference: 0.873 points, P = 0.012). In addition, economic fear was significantly higher in those who responded that the social distancing policy is ineffective than those who responded positively, by 2.216 points (difference: 2.216 points, P < 0.001). Economic fear was significantly higher in those who avoided crowded places than those who did not, by 0.728 points (difference: 0.728 points, P = 0.025)
DISCUSSION
This study aimed to identify the factors affecting COVID-19 phobia among Korean undergraduate and graduate students and the factors affecting COVID-19 phobia. To this end, we conducted an online questionnaire survey of 490 students using an assessment tool developed based on the C19P-S.
The following were the main findings of the study. The percentage of respondents who considered social distancing effective was as low as 7.6%, and this may be ascribed to the tremendous soar in daily newly confirmed cases to 400,000 for 7 consecutive days amid the fourth wave of the COVID-19 outbreak, which began on April 2, 2021. Additionally, 64.8% of respondents agreed with the government’s COVID-19 mitigation policy, which is similar to the results of a survey conducted on 1,003 Koreans in April 2022 where 69% were in favor.21 The respondents’ mean total C19P-S score was 48.1 out of 100 points, which is consistent with the score calculated in a previous study on C19P-S (47.06). When divided into subscale scores, the psychological and social subscale scores were higher than those observed in previous research studies (17.2 vs. 16.74 and 14.9 vs. 14.0, respectively), and the psychosomatic and economic subscale scores were lower than those observed in previous research studies (8.7 vs. 8.87 and 7.4 vs. 7.45, respectively).19
This survey was conducted during the fourth wave of the COVID-19 outbreak in Korea, when the average number daily newly confirmed cases was 400,000, marking a record high since its first confirmed case in January 2020, much higher than that in neighboring Japan (40,000 cases per day) and that in Australia (50,000 cases per day). As of April 19, 2022, the cumulative number of confirmed cases in Korea is 16.5 million, accounting for 31.8% of the total population (51.78 million), which is within the margin-of-error for the experience of COVID-19 infection among the respondents of the survey conducted in this study.
To analyze the differences in the C19P-S scores according to respondents’ characteristics associated with COVID-19 phobia, we performed the chi-square test and independent sample t-tests. Women were found to have a significantly higher rate of COVID-19 phobia than men, which supports the finding of a preliminary study that women have a higher fear of COVID-19 than men.2022 In addition, there was significant variation depending on the current residential area in the C19P-S scores of psychosomatic phobia and economic phobia. COVID-19 phobia was highest in Chugcheong-do/Daejeon region and lowest in Gangwon-do. According to the Community Health Survey conducted by the Korea Disease Control and Prevention Agency, Chungcheong-do/Daejeon region appeared to experience a major psychological impact due to COVID-19, which is comparable to the results of this study.23 Moreover, Gangwon-do has the second largest area among the 11 provinces and cities in Korea; it is a mountainous, difficult-to-access region. According to previous studies, greater psychological stability is felt by those residing in areas with lower population density, a result that is similar to that of this study.24
Regarding social distancing, the group that considered social distancing as being efficient scored higher on the mean total C19P-S score than the group that considered it inefficient. A previous study reported that the higher the fear of COVID-19, the higher the rate of adherence to social distancing measures.25 Despite social distancing that had been implemented at different levels, Korea saw the fourth wave of the COVID-19 outbreak with a rapid soar of daily new confirmed cases, starting from the last week of February 2020, in which discussions about easing COVID-19-related restrictions began. This sudden increase in COVID-19 infection appears to be reflected in the results of our study regarding the correlation between COVID-19 policy and COVID-19 phobia; we found that the group that disagreed with the government’s COVID-19 mitigation policy scored higher on the mean total C19P-S score than the one that agreed with it. Among the COVID-19 prevention behaviors, the groups that avoided crowded places and adhered to regular indoor ventilation showed significantly higher levels of COVID-19 phobia. With the prolongation of the COVID-19 crisis, citizens’ increased fatigue and decreased sensitivity to infection prevention measures drove high crowd densities to places such as shopping malls, supermarkets, parks, and amusement facilities. In tandem with this, the survey period (April 5 to 16, 2022) coincided with the unbridled spread of infection in the fourth wave of COVID-19 in Korea, which was reflected in the trend that the higher the level of COVID-19 phobia, the more likely respondents were to avoid crowded places. Compared with other studies, the frequency of visiting public places was considerably lower among the respondents with higher COVID-19 phobia, and the frequency was extremely low during the period of the COVID-19 wave.26 In contrast, the C19P-S scores were not significantly correlated with mandatory mask-wearing or social distancing measures. This may be attributed to the penalty imposed by the Korean government for non-compliance with mask-wearing and social distancing. In addition, the higher the educational level, the more likely citizens are to comply with government policy measures.2728 Korea is one of the OECD countries with the highest level of education, and most people adhere to all the preventive measures in place, resulting in little difference in the level of COVID-19 phobia with regard to mandatory infection prevention measures.29
Next, we used multiple linear regression to analyze the factors affecting COVID-19 phobia. The analysis revealed that whereas women generally had higher C19P-S scores, men outscored women on the economic subscale, which is not consistent with the findings of previous research, presumably due to the increased economic burden imposed on men arising from COVID-19-related economic slowdown. In addition, a significant effect of social distancing was found only in the economic subscale, which reflects the heavier economic burden on the self-employed, owing to the Korean government’s restrictions on business hours and the size of allowed gatherings (four or six persons) since 2021.30 The Korean government has introduced measures to ease the aforementioned COVID-19-related restrictions and has gradually implemented them from April 2022. However, the analysis in this study revealed that a higher COVID-19 phobia was observed in the groups that considered social distancing measures ineffective, disagreed with the government’s COVID-19 mitigation policy, and avoided crowded places. This can be interpreted to mean that, if the Korean government eases the COVID-19 mitigation policy, COVID-19 phobia among these people will likely be maximized. The WHO, in the Statement on the eleventh meeting of the International Health Regulations (2005) Emergency Committee regarding the coronavirus disease (COVID-19) pandemic, announced 11 recommendations on April 11, 2020.31 One of these recommendations is that the government should provide correct information on COVID-19 and ensure risk communication such that people can make the right decisions.32
This study had the following limitations. First, since this was a cross-sectional study, it could not determine a causal relationship between daily/cumulative confirmed cases and regulatory policies and COVID-19 fear (or phobia). Second, since the survey was carried out online due to the fourth wave of the COVID-19 outbreak, the results may have a higher rate of non-sampling errors than that of a face-to-face survey. Third, since the survey period coincided with the peak period of the fourth wave in Korea, it cannot be ruled out that the level of COVID-19 phobia measured in this study was higher than the typical level. Fourth, the gender distribution of university students was 72.6% women to 27.4% men. This distribution imbalance may be because the research department was in a health-related field, and the ratio of female students is generally high. Finally, the F-statistic of the regression model was significant, thereby the linear regression equations from Models 1 through 5 were significant, but the adjusted R2 value was less than 0.02 with a large variance around the regression line; thus, the confidence change may be low. In future research, it will be necessary to formulate an equation that minimizes the non-sampling error through face-to-face surveys and minimizes the scatter plot of the regression line by increasing the number of samples.
The Korean government has introduced measures to ease COVID-19-related restrictions, such as social distancing and reduced business hours, and has gradually implemented them since April 2022. Consequently, if the Korean government eases the COVID-19 mitigation policy, COVID-19 phobia among university students will probably increase. It is therefore necessary to establish an appropriate response plan before easing the COVID-19 mitigation policy to prevent an increase in COVID-19 phobia. In particular, measures to manage phobia and depression should be planned at the national level and policies to return to daily life as before the COVID-19 pandemic should be designed and implemented, while maintaining public trust through openness, transparency, and government accountability.
 XML Download
XML Download