

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Nontuberculous mycobacteria (NTM) are widely distributed environmental organisms that are present in the soil, natural water, and municipal water. NTM, mycobacteria other than Mycobacterium leprae and M. tuberculosis complex, can cause various human diseases, and the most common manifestation is pulmonary disease (PD).1 Epidemiological studies have shown that the prevalence and incidence of NTM infection are increasing, partly owing to improved detection techniques, greater awareness, and an aging society.2 In South Korea, between 2008 and 2016, the annual incidence and prevalence increased from 6.0 to 19.0 cases per 100,000 persons and from 9.4 to 39.6 per 100,000 persons, respectively.3 This increase in NTM infection contrasts with a declining trend in pulmonary tuberculosis (TB), indicating that NTM infection is becoming a significant medical burden.4
The number of patients undergoing solid organ transplantation (SOT) is also increasing. In 2021, SOTs performed in the United States exceeded 40,000 for the first time, an increase of 5.9 percent from the previous year.5 In South Korea, a total of 4,180 patients (1,599 from deceased donors and 2,581 from living donors) received SOT in 2020.6 Because SOT recipients are on life-long immunosuppressants, these patients have a higher risk of NTM infection, which is prevalent in hosts with impaired cell-mediated immunity.7 The incidence of NTM infection was estimated to range from 0.16% to 0.38% in kidney transplant recipients and from 0.24% to 2.8% in heart transplant recipients.7 However, although this population is at an increased risk of developing NTM-PD, information concerning the impact of SOT on the clinical presentation, course, and prognosis of NTM-PD is nearly absent.
In this study, we delineated the clinical characteristics and course of patients who developed NTM-PD after SOT at a tertiary referral center in South Korea. Then, we performed propensity score matching analysis to determine the impact of previous history of SOT on the prognosis of patients with NTM-PD.
METHODS
Study design and patient selection
We retrospectively analyzed patients who underwent SOT other than the lungs and subsequently developed NTM-PD during follow-up between January 2001 and December 2020 at Seoul National University Hospital, a tertiary referral hospital in South Korea. Because lung transplant recipients have an exceptionally high risk of developing NTM-PD due to structural lung disease or allograft exposure to NTM,8 we excluded patients who received lung transplantation in this study. All patients with NTM-PD satisfied the diagnostic criteria of the American Thoracic Society, European Respiratory Society, European Society of Clinical Microbiology and Infectious Diseases, and Infectious Diseases Society of America for NTM-PD.9
Data collection
The demographic and clinical characteristics of the patients at the time of diagnosis of NTM-PD were collected, including age, sex, body mass index (BMI), type of organ transplantation (deceased/living donor; liver, kidney, heart, pancreas), the time between transplantation and NTM-PD diagnosis, identification of NTM species from respiratory specimens, drug susceptibility test results, radiographic findings based on chest computed tomography (CT), smoking history, and relevant comorbidities (interstitial lung disease, chronic obstructive pulmonary disease, myocardial infarction, chronic heart failure, diabetes mellitus, cerebrovascular disease, and malignancy). The regimen and duration of antibiotic treatment targeting the NTM-PD, if initiated, were also collected.
Statistical analysis
Baseline characteristics were summarized as counts and proportions for categorical variables and medians with interquartile ranges (IQRs) for continuous variables. To assess the impact of a previous history of SOT on the long-term survival of patients with NTM-PD, we performed a 1:20 propensity score-matched Kaplan–Meier analysis comparing the survival of the study population with that of patients who were diagnosed with NTM-PD between January 2007 and December 2020 at the same institution. Age, sex, BMI, the presence of cavitary lesion at the time of diagnosis of NTM-PD, having M. abscessus complex species versus other species as the causative species, initiation of treatment for NTM-PD, and the presence of comorbidities (interstitial lung disease, chronic obstructive pulmonary disease, myocardial infarction, chronic heart failure, diabetes mellitus, cerebrovascular disease, and malignancy) were matched and the log-rank test was utilized. Two-sided P values < 0.05 were considered statistically significant. All analyses were conducted using the R software (version 4.1.1; R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of the Seoul National University Hospital (approval No. H-2202-109-1303), and the requirement to obtain informed consent was waived owing to the retrospective and observational study design. This study was performed in accordance with the principles of the Declaration of Helsinki.
RESULTS
Patient characteristics
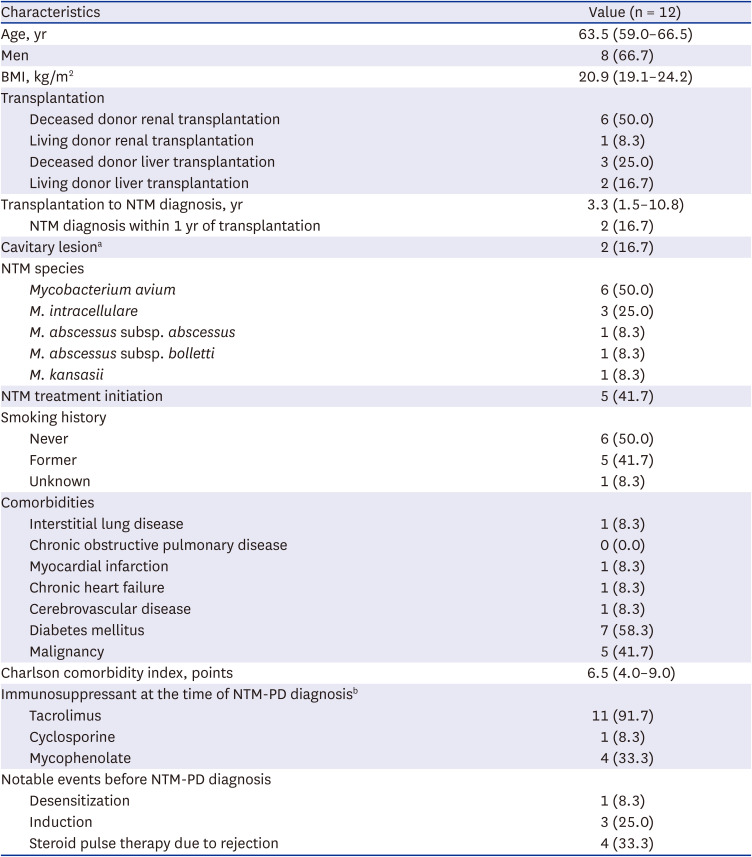
During the study period, 12 patients (median age, 64 years; IQR, 59–67 years; men, 66.7%) subsequently developed NTM-PD among a total of 4,685 SOT recipients (2,298 for kidney, 2,153 for liver, 200 for heart, and 34 for pancreas after or simultaneously with kidney). Seven (58.3%) and five (41.7%) patients underwent renal and liver transplantation, respectively. The median Model For End-Stage Liver Disease score of liver transplant recipients was 25. Nine out of 12 patients (6 for kidney and 3 for liver) received transplantation from deceased donors. The median time between transplantation and diagnosis of NTM-PD was 3.3 years (IQR, 1.5–10.8 years). Two patients (18.7%) developed NTM-PD within 1 year of transplantation. The incidence of NTM-PD was 35.6 cases per 100,000 person-years among kidney transplant recipients and 28.6 cases per 100,000 person-years among liver transplant recipients. One (8.3%) and three (25.0%) patients underwent desensitization or induction before transplantation, respectively. No one received thymoglobulin induction. Four (33.3%) patients received corticosteroid pulse therapy for the treatment of allograft rejection. At the time of NTM-PD diagnosis, tacrolimus was administered to 11 (91.7%) patients with a median trough level of 4.7 ng/mL (IQR, 4.1–5.9 ng/mL). Other than patient No. 9, whose mizoribine was stopped and tacrolimus was changed to sirolimus, no reduction or modification of immunosuppressant was made in other patients at the time of NTM-PD diagnosis. The detailed demographic and clinical characteristics of the study population are summarized in Table 1.
Table 1
Baseline characteristics of the study population
NTM-PD characteristics
The most common mycobacterial species identified were M. avium (n = 6, 50.0%), followed by M. intracellulare (n = 3, 25.0%), M. abscessus subsp. abscessus (n = 1, 8.3%), M. abscessus subsp. bolletti (n = 1, 8.3%), and M. kansasii (n = 1, 8.3%). Most patients showed a nodular bronchiectatic pattern (n = 10, 83.3%), whereas two patients (16.7%) had cavitary lesions on chest CT. Detailed clinical information of each patient is presented in Table 2.
Table 2
Detailed clinical information of each patient
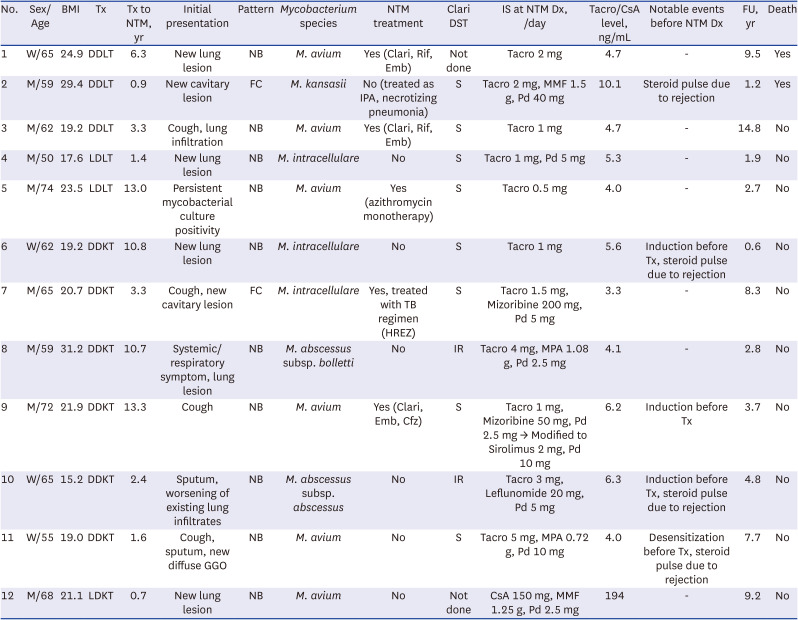
W = woman, M = man, BMI = body mass index, Tx = transplantation, DDLT = deceased donor liver transplantation, DDKT = deceased donor kidney transplantation, LDLT = living donor liver transplantation, LDKT = living donor kidney transplantation, NTM = nontuberculous mycobacteria, GGO = ground glass opacity, NB = nodular bronchiectatic, FC = fibrocavitary, Clari = clarithromycin, Rif = rifampicin, Emb = ethambutol, IPA = invasive pulmonary aspergillosis, TB = tuberculosis, HREZ = isoniazid/rifampicin/ethambutol/pyrazinamide, Cfz = clofazimine, DST = drug susceptibility test, IR = inducible resistance, S = susceptible, IS = immunosuppressant, Dx = diagnosis, Tacro = tacrolimus, MMF = mycophenolate mofetil, Pd = prednisolone, MPA = mycophenolate acid, CsA = cyclosporine A, FU = follow-up duration.
At the time of transplantation, chest radiographs showed no definite abnormalities in 8 patients (66.7%) and mild lung infiltration in 4 patients (33.3%). Among them, only one patient showed worsening of the existing lung infiltrates, whereas three patients developed new lesions in different lung regions. All sputum acid-fast bacilli tests were negative at the time of operation.
Clinical course and prognosis of study population
During a median follow-up of 4.2 (IQR, 2.3–8.8) years after the diagnosis of NTM-PD, antibiotic treatment was initiated in five (41.7%) patients with M. avium (4 patients) and M. intracellulare (1 patient) due to radiographic and/or symptomatic aggravation. The interval between NTM-PD diagnosis and treatment initiation was 1.3 (IQR, 0–1.8) years. Three patients received guideline-adhering therapy with clarithromycin, ethambutol, and either rifampicin or clofazimine, one patient (No. 5) received azithromycin monotherapy, and another patient (No. 7) was treated with a pulmonary TB regimen: isoniazid, rifampicin, ethambutol, and pyrazinamide. Culture conversion and microbiological cure were achieved in five (100%) and two (40%) patients, respectively. Both patients who underwent treatment not adhering to guidelines achieved culture conversion and patient No. 5 remained culture negative during treatment whereas patient No. 7 experienced recurrence after 14 months. Nonetheless, patient No. 7 was carefully observed without further treatment due to lack of symptomatic and radiographic aggravation.
During the study period, two patients died. One patient who received guideline-adhering NTM-PD therapy died of respiratory failure due to underlying idiopathic pulmonary fibrosis. The other patient who showed multiple cavitary lesions on chest CT with persistent fever and sputum was infected with M. kansasii. However, he was treated for suspected invasive pulmonary aspergillosis and necrotizing pneumonia. When retrospectively evaluated, NTM-PD was assumed to be the cause of death in this patient.
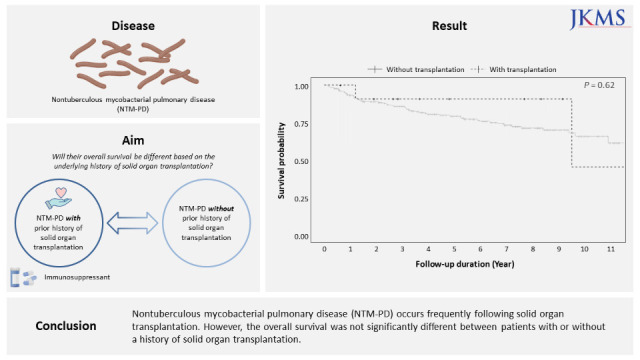
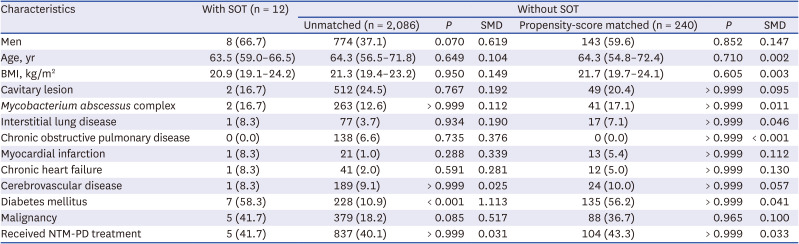
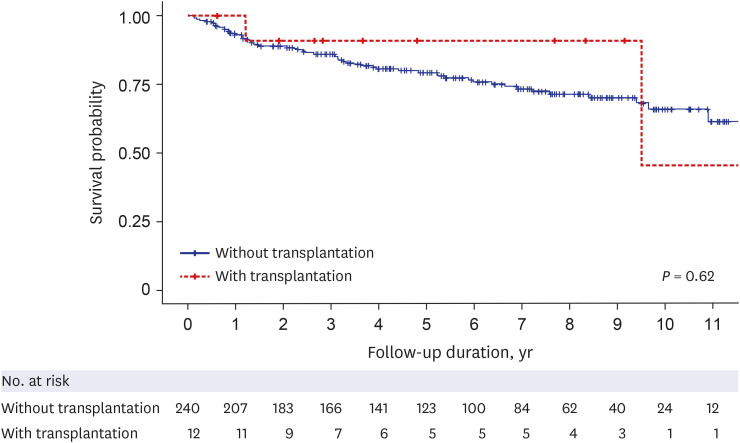
After propensity score-matching, every patient with a history of SOT was paired with 240 patients without a history of SOT. Characteristics and standard mean difference of the two groups are presented in Table 3. The overall survival between the two groups showed no statistical difference (log rank P value 0.62). The Kaplan–Meier survival plot is shown in Fig. 1.
Table 3
Characteristics of control group and the study population, before and after propensity score matching
DISCUSSION
The present study investigated the clinical characteristics, course, and prognosis of SOT recipients who subsequently developed NTM-PD during the follow-up period. Overall, 12 of 4,685 patients who received SOT developed NTM-PD over 20 years or an average incidence of 32.5 cases per 100,000 person-years. The median time between transplantation and diagnosis of NTM-PD was 3.3 years and the most common causative mycobacterial species was M. avium. The nodular bronchiectatic pattern was more prevalent than the fibrocavitary pattern, and antibiotic treatment was initiated in 41.7% of patients. During a median follow-up of 4.2 years (IQR, 2.5–8.6 years), two patients died, and only one case was assumed to be related to NTM-PD. The matched analysis showed no difference in overall survival between patients with or without a history of SOT.
This study principally showed that when NTM-PD occurs in SOT recipients, it is not significantly different from that in the general population. Even with immunosuppressant use and history (41.7%; 5 of 12 patients) of desensitization, induction, and corticosteroid pulse therapy due to allograft rejection, disease progression was observed in six (50%) patients, and antibiotic treatment was adopted in five (41.7%) patients. Other six (50%) patients did not show signs of disease progression for a median follow-up duration of 3.8 years (IQR, 2.1–7.0 years). This finding is comparable to one study based on a cohort where 94% of patients were not on immunosuppressant. Of these, 62.5% of patients showed progression of NTM-PD requiring treatment initiation within 3 years of diagnosis.10 After matching for key characteristics, the overall survival of our study population was not significantly different from that of patients without a history of SOT. Hence, the idea that the clinical course and prognosis may differ when NTM-PD develops in SOT recipients is not well established.
Although the process is not fully understood, NTM-PD improves without treatment, which have been the case for patient No. 5 and No. 7, who responded favorably despite guideline-discordant therapy. Previous studies have reported spontaneous culture conversion occurring in 25.8–51.6% of the study population.101112 Lower number of lobes involved, young age, higher BMI, negative sputum acid-fast bacilli smear, and transient anti-TB medication at the time of diagnosis were associated with spontaneous culture conversion.1011 In this context, the favorable response of patient No. 7, who received anti-TB treatment at the time of diagnosis and was affected in only one lobe, can be partially explained. On the other hand, patient No. 5 was diagnosed with NTM-PD 13 years after undergoing living donor liver transplantation and was prescribed tacrolimus 0.5 mg/day, which was the lowest dose administered among the study population. Even though we found no differences in the prognosis of NTM-PD based on SOT history, minimal disruption of the host’s immunity may have contributed to the favorable response; however, more research is needed to be generalized.
The incidence of NTM-PD in our study population was higher than that among the general population in Korea.13 According to previous studies based on national health insurance data, the reported incidence of NTM infection was 17.9 to 19.0 cases per 100,000 persons in 2016.314 In this study, the incidence of NTM-PD was 35.6 cases per 100,000 person-years (0.30%) in kidney transplant recipients and 28.7 cases per 100,000 person-years (0.23%) in liver transplant recipients. The use of immunosuppressants following transplantation, which depress cell-mediated immune responses and consequently increase susceptibility to a number of intracellular pathogens, including NTM, is likely to be the cause of this higher incidence compared with the general population.15 These numbers were also similar to or higher than the previously reported incidence of NTM-PD among SOT recipients, which was 0.16% to 0.38% in kidney transplant recipients71617 and 0.04% in liver transplant recipients.18 However, due to small sample size of this study, our findings should be taken in light of the different study design, population composition, and research period from those of previous studies.
Our study had several limitations. First, owing to the few patients with NTM-PD identified, we only provided a descriptive analysis of these patients. Second, this study was conducted retrospectively at a single institution, limiting the generalizability of our findings. Patient characteristics, the proportion of patients requiring antibiotic treatment, and long-term survival may vary depending on the composition of the study population in different settings. Also, because we excluded patients who underwent lung transplantation, applying the results to all SOT patients is limited and more research including lung transplant recipients is warranted. Third, there was a substantial reduction in the sample size after matching, potentially introducing bias in our findings. Thus, additional data from other large prospective cohorts are required.
In conclusion, NTM-PD occurs frequently following SOT. However, the overall survival is not significantly different between patients with or without a history of SOT.
 XML Download
XML Download