

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
A systematic review of cross-sectional reported the prevalence of depression was 25% in the general population during the coronavirus disease 2019 (COVID-19) outbreak. This was 7 times higher than the overall global estimated prevalence of depression of 3.4% in 2017.1 According to the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (American Psychiatric Association, 2013), the criteria for major depressive disorder are met when an individual exhibit at least five of nine heterogeneous psychiatric symptoms. Previous research shows that different life stressors provoke different symptoms of depression,2 giving insight into the need for research regarding the heterogeneity of depression symptoms. It is important to determine whether there has been an increase in severe depression since COVID-19. Individuals with severe depression are more likely to develop serious mental health problems, and even commit suicide. If we know that certain depressive symptoms are related to the COVID-19 infectious disease crisis and if the number of individuals with severe depressive symptoms increased during COVID-19, it is expected that this will help in establishing community mental health management and treatment methods in the future.
Gender differences in the prevalence of depression were highlighted in the1970s. About twice as many women suffered from depression as men.3 Although restrictions on daily life and changes in economic structure due to COVID-19 would likely have affected men and women differently, there is still a lack of research on the impact of COVID-19 on depression levels among men and women.
A previous report has shown that there were associations among employment, economic status, and mental health suggesting that persistent job insecurity or loss of job security was related to adverse psychological conditions, including psychological distress, depressive symptoms, and anxiety symptoms.4 Some other studies have found that employment status had a profound impact on men’s mental health. Such work-related factors as unemployment, economic insecurity, poverty, and stressful working environment, have been associated with men’s mental problems.5 The economic insecurity caused by the COVID-19 pandemic may threaten men’s position.6 As the COVID-19 pandemic has both economic and occupational impacts, we assume that there may be a gap between men and women in the size of mental health impact left by the COVID-19.
This study investigated whether there was gender difference in the magnitude of increase in prevalence of depression, depression severity, and individual symptoms of depression during COVID-19 compared with before the pandemic using the Korea National Health and Nutrition Examination Survey (KNHANES) data. The KNHANES has been conducting surveys annually with the same sampling frame, survey tools, and methods; it can identify changes in mental health status throughout the community before and after the COVID-19 pandemic.
Go to : 
METHODS
Study population
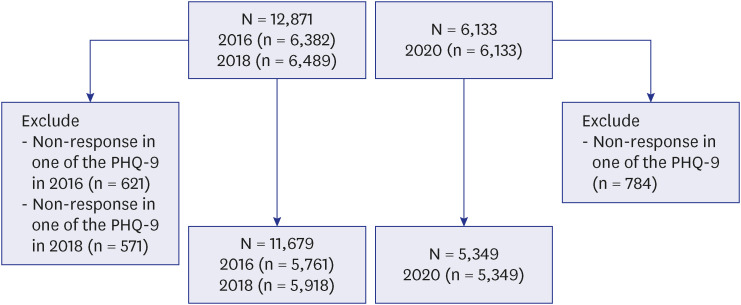
The target population of KNHANES comprises noninstitutionalized Korean citizens residing in Korea. The sampling plan follows a multi-stage clustered probability design.7 Primary sample units (PSUs) for KNHANES were chosen from a sampling frame of all census blocks or resident registration addresses. Each PSU consisted of approximately 50 to 60 households. Following the selection of PSUs, it was made a list of all dwelling units in the PSU were and selected around 25 households for a field survey for household screening. The final stage of selection was made in each household, where all members aged one year or older were included as participants. The sample weights were calculated for sample participants to represent the Korean population by accounting for the complex survey design, survey non-response, and post-stratification. The weights based on the inverse of selection probabilities and response rates were modified by adjusting for the sex- and age-specific Korean populations. Since depression was evaluated biannually, a KNHANES (2016, 2018) sample of 11,679 individuals was used to evaluate pre-pandemic depression, and a KHANES 2020 sample of 5,854 individuals was included to evaluate the effects of the first year of the pandemic on depression. In this study, analysis was conducted on subjects at 19 years of age or older. A flowchart of the included analysis samples in each outcome is presented in Fig. 1.
Measurements
Depression was measured by the Patient Health Questionnaire-9 (PHQ-9). PHQ-9 is a self-reporting assessment tool useful for depression screening and used to determine the severity of depressive symptoms.8 KNHANES used PHQ-9 for the first time in 2014, and continued ever since in every other year. This depression assessment tool consists of a nine-item depression module that assesses if individuals experienced “little of interest,” “feeling down or hopelessness,” “trouble falling or staying asleep,” “Poor appetite or overeating,” “feeling tired,” “feeling bad or worthlessness,” “trouble concentrating,” “moving or speaking slowly that other people could have noticed,” and/or “suicidal ideation” over the past two weeks. These items were adopted directly from the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition. Each item is scored from 0 (not at all) to 3 (almost every day), with the higher score indicating severer depressive symptoms. Clinically significant depression requiring treatment was determined using an optimal cut-off score 10.89 The Korean version of PHQ-9 was previously validated so it could be used in the Korean population.10
Binary classification of depression was defined by a score of a PHQ-9 score ≥ 10. Depression symptom severity categories were defined as none (score 0–4), mild (score 5–9), moderate (score 10–14), moderately severe (score 15–19), and severe (score ≥ 20). In addition, the presence or absence of individual depressive symptoms was classified as “No” when “Not at all” was answered, and “Yes” when “Several days” or “More than half the days” or “Nearly every day” was answered for each question.
Demographic characteristics
Participants reported their age (grouped into 19–29, 30–39, 40–49, 50–59, 60–69, and 70+ years old). Years of education was categorized into four groups: 0–6; 7–9; 10–12; 13 or more. Marital status was classified by whether or not the participant has spouse. Residential area was either urban or rural, employment condition either employed or not employed. Monthly household income was divided into five groups with the lowest income through the highest income quintiles.
Statistical analyses
All analyzes were stratified by gender to present the differences between men and women. Categorical factors were represented as numbers and weighted percentages. All comparisons and analyses were weighted based on the complex survey design of both studies and producing nationally representative estimates. Sampling weights were generated accounting for complex sample design and nonresponse rates of the target population. PROC SURVEYFREQ was used to calculate weighted prevalence and confidence intervals (CIs), and also the weighted difference and CIs between the two periods using PROC SURVEYREG. We applied Difference-in-differences (D-I-D) design to measure the change of prevalence of depression between before and after COVID-19 in men and women using the following equation.
Where Y is prevalence of depression, sex is a dummy variable for group assignment (men = 1, women = 0), and time point is dummy variable for the time point (after COVID-19 [2020] = 1, before COVID-19 [2016, 2018] = 0). The interaction term is the D-I-D estimator. The statistical significance of the interaction term was estimated using PROC SURVEYLOGISTIC. All statistical analyses were analyzed with two-tailed tests and were considered statistically significant for P < 0.05 using SAS analytics software version 9.4 (SAS Institute, Cary, NC, USA).
Ethics statement
KNHANES has been conducted by the Korean government for public welfare in accordance with paragraph (1) of Article 2 of the Bioethics and Safety Act and Article 2 (2) 1 of the Enforcement Rule of the same act. Based on that fact, the Institutional Review Board (IRB) exempted its review on it; thus KNHANES 2016 was conducted without IRB approval. Since KNHANES 2018, however, IRB approval has been obtained because it collected human data prospectively, and KNHANES raw data has been available to third-party users for KNHANES 2018 and 2020 (2018-01-03-P-A and 2018-01-03-2C-A). All subjects signed a consent form before participating in the survey.
Go to :
RESULTS
The socio-demographic characteristics of the KNHANES participants in 2016 and 2018 (before COVID-19) and in 2020 (during COVID-19) are shown in Table 1. The total number of subjects aged 19 years or older was 11,679 in 2016 and 2018 and 5,349 in 2020. Of these, 5,056 were men and 6,623 were women in 2016 and 2018; and 2,417 were men and 2,932 were women in 2020. The gender ratio was the same for each survey period. For both men and women, the distributions by age group, year of education, marital status, residential area, employment condition, and household income were similar in the 2016, 2018 and 2020 surveys (Table 1).
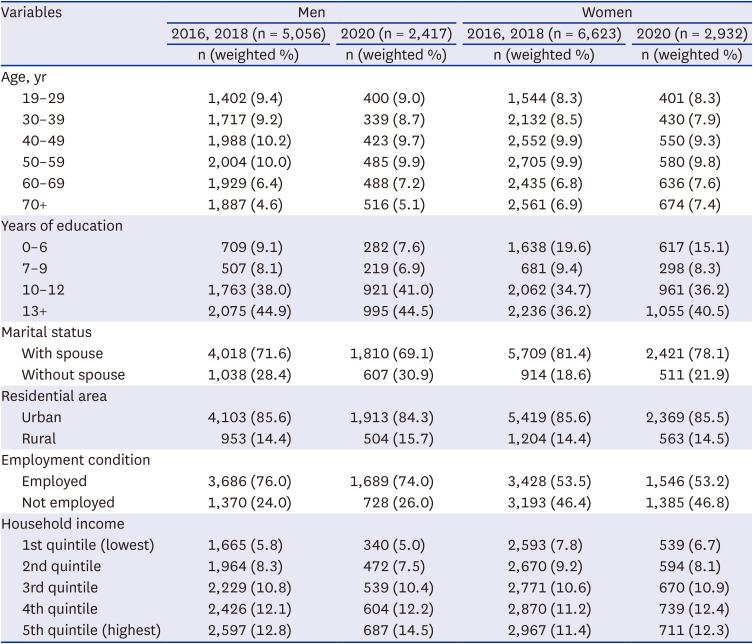
Table 1
Socio-demographic characteristics of a nationally representative sample of Korean adults before and during the COVID-19 pandemic, stratified by gender
![]()
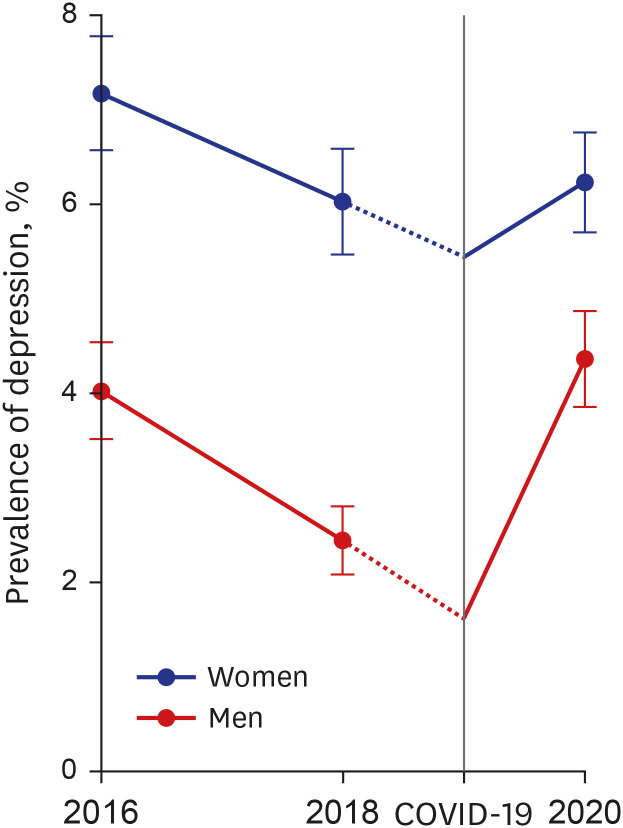
The weighted prevalence of depression in 2016, 2018, and 2020 was 4.0%, 2.4%, and 4.4%, respectively in men; 7.2%, 6.0%, and 6.2%, respectively, in women. The prevalence of depressive symptoms showed similar in men and women before COVID-19 with holding parallel trends assumption before conducting D-I-D.11 As shown in Fig. 2, the prevalence of depression was decreased trend before COVID-19, however it has shifted in the direction of increasing during the COVID-19, with a marked increase in men compared to women.
The D-I-D design estimated sex difference in prevalence of depression between before and after COVID-19. The results showed that statistically significant sex difference in prevalence of depression between before and after COVID-19 (interaction term P = 0.036) (Table 2).

Table 2
Difference-in-differences in prevalence of depression between before and after COVID-19 in men and women
![]()
In men, the prevalence of depression symptoms severity was higher in every category during the pandemic than before. There was a little difference in mild depression symptoms prevalence before and during COVID-19 (10.8% [95% CI, 9.7–11.9] and 0.9% [95% CI, 9.3–12.6], respectively); moderate depression symptom prevalence was slightly higher, 2.2% (95% CI, 1.7–2.6) before compared with 2.7% (95% CI, 1.9–3.4) during COVID-19; moderately severe depression symptom prevalence was slightly higher, 0.8% (95% CI, 0.5–1.0) before compared with 0.9% (95% CI, 0.5–1.3) during COVID-19; and severe depression prevalence was 0.3% (95% CI, 0.1–0.5) before COVID-19 compared with 0.8% (95% CI, 0.4–1.3) during COVID-19. Severe depression symptom prevalence was 0.5% (95% CI, 0.0–1.0), a significant increase from before to during COVID-19 in absolute difference. The prevalence of severe depression symptoms was 2.6-fold (95% CI, 1.2–5.7) higher during COVID-19 compared with before COVID-19 in relative difference. In women, there was no difference in any depression symptom category before and during COVID-19 (Table 3).
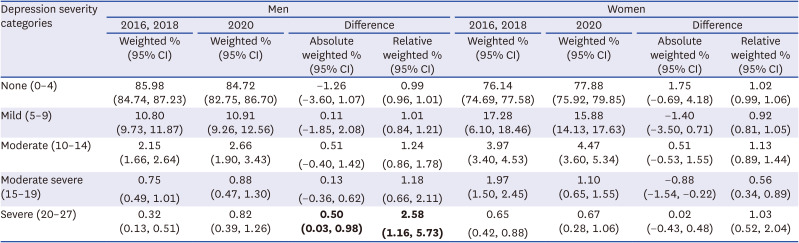
Table 3
Absolute and relative differences in depressive symptom severity proportions by gender before and during COVID-19
![]()
In men, during the pandemic the prevalence of difficult symptoms with little interest or pleasure in doing things was 1.26-fold higher, the symptoms of feeling tired or having little energy were 2.2-fold higher, and thoughts that it would be better to die or self-harm were 1.7-fold higher compared with before COVID-19. However, in women there was no significant difference in any symptom before and during COVID-19 (Table 4).
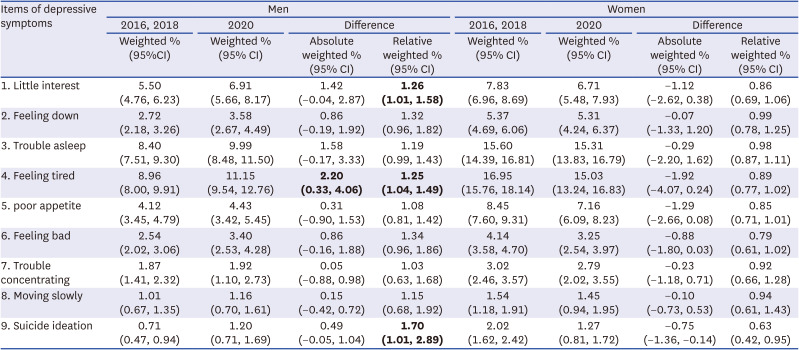
Table 4
Differences in absolute and relative positive rates in individual depression symptoms by gender before and during COVID-19
![]()
Go to :
DISCUSSION
The COVID-19 pandemic has affected socio-economic status as well as individuals’ mental health. According to Organization for Economic Co-operation and Development reports, the COVID-19 pandemic reduced the global real GDP by 4.5% in 2020 compared with 2019.12 The COVID-19 pandemic brought about an employment crisis due to reducing production and the labor market worldwide.13 Its impact on unemployment became so rampant in March and April of 2020 that the Korean government imposed quarantine measures including social distancing and restriction of social gatherings. More than one million individuals lost their jobs in a month.14
This study investigated the impact of the COVID-19 pandemic on gender differences in depression using Korean national representative data. There were gender differences in reactions to COVID-19 based on differences in the prevalence of depression, with its severity and individual symptoms before and during the COVID-19 period, although the point prevalence of depression was higher in women than in men in both periods. The weighted prevalence of depression increased by 40% among men, and there was no difference in women, indicating that men may react significantly worse to lockdown in terms of depression than women. When classified according to depression symptoms severity, weighted prevalence significantly increased by 2.6 times in the severe depression group. Of the nine symptoms of depression, three symptoms significantly increased: “Little interest or pleasure in doing things,” one of the core symptoms of depression, significantly increased by 1.3 times. “Feeling tired or having little energy” increased by 1.3 times, and “Suicidal thoughts” increased by 1.7 times during COVID-19 compared to before the pandemic in men, but there were no differences in women before- and during COVID-19. Existing literature about the COVID-19 pandemic has reported that women demonstrated a higher prevalence of mental health issues, including depression, than men.1516) Point prevalence of depression among women is higher than that of men when pre-COVID-19 prevalence is not considered.
The current study hypothesized that COVID-19 social distancing measures induce mental health effects differently among men and women. Although COVID-19 has affected the mental health of the entire population,17 this study compared changes in the prevalence of depression between men and women during COVID-19 compared to before COVID-19. It has been suggested that the magnitude of the effect on mental health may differ according to gender in response to social changes caused by various social distancing policies as well as fear of infectious disease. Investigating how gender differences in depression evolved during the pandemic compared with before COVID-19, will help us understand the consequences of the various social measures imposed due to COVID-19. The current study clearly found a difference between men and women: the prevalence of depression in men significantly increased during the COVID-19 pandemic compared with before COVID-19. Moreover, from a public health perspective, the significant increase in those with severe depression suggests that more attention should be paid to male depression caused by COVID-19. The D-I-D design correctly estimates sex difference in prevalence of depression between before and after COVID-19, since the parallel trends assumption is that the change in the prevalence of depression between 2016 and 2018 is similar in both sexes. However, the trend of the prevalence of depression before COVID-19 was analyzed with only two points in 2016 and 2018, it may not be sufficient data to estimate a stable trend.
The main reason for men’s increased depression seems to be that men are concerned about economic challenges caused by the COVID 19 than women because as economically active population, they were more affected by layoffs and business closures. The COVID-19 pandemic also resulted in an employment crisis with challenges for supply chain and the labor market. The explosive pandemic spread so quickly in March and April of 2021 that the Korean government imposed Level 2 quarantine measures including social distancing and restriction of social gatherings which caused more than one million jobs lost in a month.18 Moreover, an unpaid leave policy was instituted for employees in various professional settings such as airlines and travel agencies.19 This type of policy would have added to the psychological burden in men.
Although gender roles differ across time and space, in Korean society, male identity is, in a complicated way, linked to having a job and it is severely challenged by unemployment. Uncertainty and worries of the future employment may have a higher impact on men’s mental health than on women’s mental health. A previous report has revealed that earlier periods of financial recession appeared to have a greater impact on the mental health of men compared to that of women,20 such as an increased prevalence of depression among men compared to women during the Spanish economic crisis.21
The significant increase in the prevalence of severe depression in men during COVID-19 may be partially explained by gender differences in help-seeking for mental health problems. Women may seek help or treatment earlier or more easily than men.22 Although depression is about twice as prevalent in women, men are 1.8 times more likely to commit suicide.2324 Earlier antidepressant use was previously reported to be associated with lower cortisol measures.25 The relatively less early treatment-seeking by men may have also contributed to a disproportionately greater increase in depression severity in men.
Symptoms related to suicidal ideation significantly increased by 1.7 times in men. This can be explained by the difference between men and women in the way they cope with stressful situations. Men have been reported to make riskier decisions under stress.2627 In contrast, women were more likely to demonstrate a prosocial “tend and befriend” response in reaction to acute stress.28 Experiencing little interest or pleasure in doing things was 1.26-fold significantly higher than before COVID-19. While subjects with reduced ventral striatum (VS) reactivity to reward was associated with greater anhedonia, greater VS reactivity to losses or recent life stressors was linked to a negative affect.2930 A significant sex difference was previously reported for VS and cortisol reactivity to reward and stress.31
From an evolutionary perspective, men with more reactive salience and stress systems may have an edge over others in challenging situations such as hunting, survival, and reproduction. However, such enhanced reactivity to acute stress may render men more prone to reactive depression, substance abuse, and suicide in stressful situations.32 Future studies should verify the relative contribution of biological and cultural factors that lead to the more pronounced severity of depression in men experiencing acute stressful situations.
This study had several limitations. It is better to provide the temporal pattern or trend of depression before and after COVID-19 to understand the trend, we reported only the thresholds of the during COVID-19 compared to before COVID-19, since there were not enough period data to see the trend. Future research should identify gender-specific changes in depression prevalence in before and during the COVID-19 pandemic using longitudinal data to explore if such changes were associated with socio-demographic, movement behaviors, and health variables due to the COVID-19 pandemic. We did not standardize comparisons between the pre-pandemic period (2016 and 2018) and the first year of the pandemic (2020). However, because between 2016, through 2020 was a relatively short period, we did not expect any serious changes in the population composition affecting the current study results, and all frequencies were calculated as weighted values for a representative Korean population in the current analyses. The current survey did not include residents in long-term care institutions, the prevalence of depression in the general population may have been underestimated. People living in long-term care institutions have experienced a reduction in social contacts, with a consequent increase in depression during the pandemic period. A strength of the study is that we drew on nationally representative probability-based samples including the same measures at each time-point, leading to the generation of meaningful estimates of population prevalence. Though plenty of cross-sectional online surveys with convenience samples have reported on point depression prevalence, they have failed to consider any changes in depression before and during the COVID-19 pandemic by gender.
According to the current findings, both severe depression level and suicide ideation increased during COVID-19 compared to before COVID-19 among men. A previous report estimated that 15% of patients with severe major depression eventually die from suicide, though suicide is an unpredictable event.33
The COVID-19 pandemic, in spite of many expected negative repercussions on mental health, may not lead to an immediate increase in the suicide rate34; however, possibly the long-term negative social and economic impacts of the COVID-19 pandemic may eventually result in such increase.353637 Given that the mental health effects of the pandemic are likely to increase over time due to prolonged financial distress and ramification of underemployment or post-infection, the researchers anticipate an increase in the prevalence of some psychiatric illnesses. Specifically, since the suicide rate of men is higher than that of women, active public health interventions are needed to prevent an additional increase resulting from the long-term effects of the pandemic. It is also necessary to establish national policies for overcoming psychological, social, and economic losses from COVID-19.
Go to :
 XML Download
XML Download