

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
With improvements in efforts to prevent suicide globally, suicide rates have been decreasing in many countries. However, suicide rates in some countries, such as the United States (US), the Netherlands, and Australia, have increased over the past decade. In Korea, the rate of suicide is still very high, even though it has generally been declining.1 The suicide rate in Korea is 2.4 times higher than those of Organization for Economic Co-operation and Development member countries, of which there were 28.6 deaths per 100,000 people recorded in 2019. These statistics suggest that a comprehensive approach and improvement of the effectiveness of preventive programs are urgently needed to reduce the rate of suicide globally.2
It is widely recognized that in addition to mental disorders such as depression and alcohol use disorder, previous suicide attempt (SA) or self-harm behavior is a strong risk factor for eventual suicide.3456 Individuals who attempt suicide or self-harm owing to suicidal ideation need immediate psychiatric intervention and constant attention from the community, which is one of the major strategies for suicide prevention.7 Compared to suicidal ideation, which can only be identified through reports by the individual, SA is an indicator of suicide risk that can be detected objectively. Understanding the magnitude of SA in detail is of great relevance in implementing preventive interventions since it can provide important clues for identifying vulnerable subpopulations and intercepting suicidal trajectories.8 Nevertheless, it is difficult to calculate the overall incidence of SA at the national level, partly because many cases of SA are not reported for reasons such as social stigma or because it is impossible to systematically detect the occurrence of SA.
The emergency department (ED) database can be a valuable resource for monitoring SA because the ED often serves as the first point of medical contact for individuals at the risk of committing suicide.910 Individuals who attempt suicide or self-harm can be treated for physical injuries and provided with psychiatric interventions in the ED, and directed to receive subsequent continuous care in inpatient or outpatient settings.11 Thus, the ED can function as a part of the suicide surveillance system and as a referral facility for individuals with a risk for suicide.10 In Korea, most local EDs are designated and managed by the government health authority, and information on ED visits, including patient characteristics or utilization of EDs, are collated through these EDs nationwide. This database permits the evaluation of the magnitude and trends of SA or self-harm among individuals who visit the ED, which can contribute to the identification of subpopulations with a high risk for suicide and guide the implementation of effective prevention strategies for them.
It is important to identify and monitor subpopulations with elevated risks for suicide in consideration of age, sex, or other demographic characteristics to facilitate the development of tailored countermeasures aimed at mitigating the risk factors of suicide.12 The purpose of this study was to examine annual trends in age standardized ED visits for adult SA or self-harm in Korea from 2016 to 2020 using the nationwide data, and to investigate the characteristics related to the utilization of the ED for SA or self-harm and the disposition of the patients at discharge.
METHODS
Study design and data sources
This retrospective population-based study was conducted using data on ED visits for SA or self-harm from 2016 to 2020 extracted from the National Emergency Department Information System (NEDIS). The NEDIS is a nationwide ED-based database developed in 2003 to evaluate the performances of the emergency care systems in Korea. To achieve the unique goal of evaluating emergency care systems, the participating EDs submitted visit-level patient data, including demographic, clinical, administrative, and relevant hospital information, to NEDIS. All patient-related information is anonymized and submitted electronically to the central processing facility. Data inconsistencies are investigated using computerized algorithms and through manual checks by a trained data manager. In 2020, all the EDs in Korea (n = 403) participated in the NEDIS data collection. The participation rates of the EDs since 2016 are presented in Supplementary Table 1. The detailed design and variables of the NEDIS database have been described previously.1314
Study population
The study population included adult patients (who were older than aged 18) who visited EDs for SA or self-harm from January 2016 to December 2020. SA or self-harm was defined as an injury caused by intentional self-harm according to the Columbia Classification Algorithm of Suicide Assessment.15 Patients of unknown age and sex were excluded from the study.
Variables
The following demographic and clinical variables of ED visits for SA or self-harm were collected from the NEDIS: sociodemographic factors, including sex (male or female), age group (19–29, 30–44, 45-64, or 65+ years), comorbid psychiatric conditions including a pre-existing psychiatric diagnosis extracted from the patient’s history or a provisional psychiatric diagnosis made in the ED (dementia, alcohol use, schizophrenia, bipolar disorder, depression, anxiety disorder, adjustment disorder, somatoform disorder, or sleep disorder [all identified using International Classification of Diseases (ICD)-19 codes]), and type of insurance (National Health Insurance, Medical Aid, or others); pre-hospital factors, including method of SA, season at the time of SA (spring, summer, fall, or winter), time of arrival to the ED (9am–6pm or 6pm–9am), initial triage, length of stay (< 6 hours or ≥ 6 hours), and patient disposition; and post-hospital factors including patient disposition at discharge and mortality. Initial triage was designated according to the Korean Triage and Acuity Scale (KTAS), which prioritizes patients according to five ordinal scales that reflect both clinical severity and acuity (1, resuscitation; 2, emergent; 3, urgent; 4, less urgent; 5, non-urgent). Methods of SA were classified as vehicle-related, jumping, cutting, drowning, poisoning, hanging, or others. The dispositions of patients who visited the ED were classified into ‘against medical advice’ (AMA) and non-AMA, and the latter was categorized into home, hospitalization, transfer, death in the ED, or others/unknown. Similarly, patient disposition at discharge was categorized into AMA, home, transfer, death, or others/unknown.
Statistical analysis
The age-standardized rates of ED visits for SA or self-harm per 100,000 persons were calculated using data from the 2020 resident registration population, as reported in the Korean Statistical Information Service database of Statistics Korea (https://kosis.kr/). We plotted the rate of ED visits for SA or self-harm and evaluated the sex-specific rates of hospital mortality among individuals who visited the ED for SA or self-harm. To visualize the scale and the severity, we estimated injury pyramid from ED visits for SA or self-harm to death in Supplementary Table 2. We also calculated the proportions of the pyramid for each year in Supplementary Table 2. In addition, we summarized the demographic characteristics of the individuals who visited the ED for SA and self-harm and calculated the proportions of the patients according to age groups and sex using the chi-square test, and tested for significant annual trends among the patients according to age groups and sex using Jonckheere-Terpstra trend test. We conducted a sensitivity analysis and summarized the number of ED visits for SA or self-harm in Korea according to sex and age. In addition, we calculated the proportions of patients with underlying psychiatric disorders, followed by a chi-square test performed according to sex. Statistical analyses were conducted using the R software (version 4.1.1; R Foundation for Statistical Computing, Vienna, Austria). Two-tailed statistical tests were conducted, and statistical significance was set at P < 0.05.
Ethics statement
This study was approved by the Institutional Review Board of the National Medical Center (approval number: NMC-2021-10-123) and was performed according to the tenets of the Declaration of Helsinki. Owing to the retrospective nature of this study, the requirement for informed consent for inclusion was waived by the same board that approved the study protocol.
RESULTS
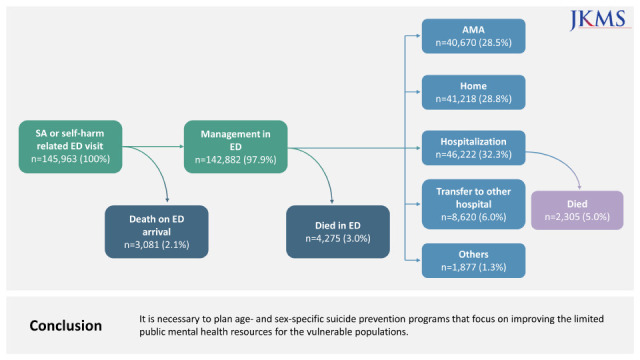
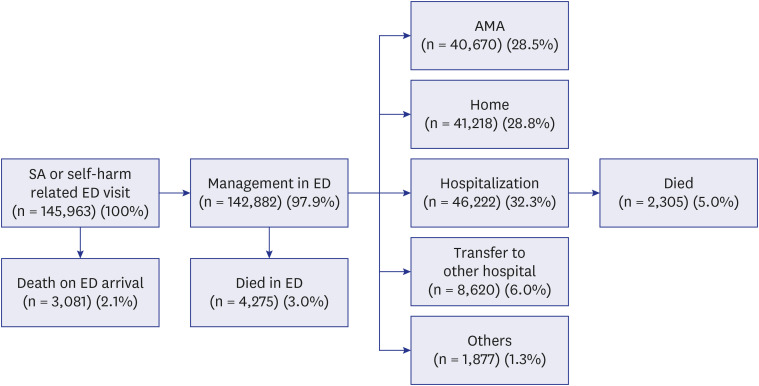
Of a total of 34,591,040 ED visits recorded during the study period, 145,963 (0.42%) were ED visits for SA or self-harm. The proportion of ED visits for SA or self-harm out of all ED visits increased from 0.37% to 0.51% between 2016 and 2020 (Supplementary Table 3). During the study period, 3,081 (2.1%) patients were dead on arrival (DOA) at the ED, whereas 142,882 (97.9%) were admitted to the ED (Fig. 1). Among the patients admitted to ED, 4,275 (3.0%) died in the ED, 40,670 (28.5%) were discharged AMA from the ED, 41,218 (28.8%) were discharged after primary treatment, and 46,222 (32.3%) were hospitalized following evaluation in the ED. Overall, the mortality rate for ED visits for SA or self-harm, including deaths on arrival to the ED, was 6.6% (n = 9,661).
Fig. 1
Summary of results and disposition routes after ED visits for SA or self-harm. The proportion of disposition after the ED admission was calculated with the population treated in ED as the denominator (n = 142,882), except the proportion of patients who died after hospitalization (2,305/46,222).
SA = suicide attempt, ED = emergency department, AMA = against medical discharge.
Trends of ED visits for suicide attempts or self-harm by sex and age group
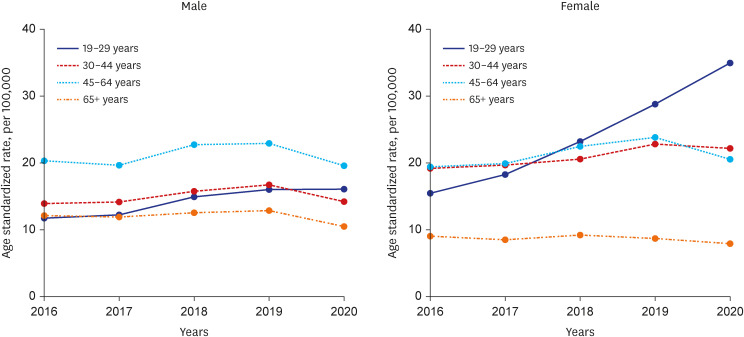
The age-standardized rates of ED visits for SA or self-harm from 2016 to 2020 stratified according to sex and age group are shown in Fig. 2. For men, the group of aged 45–64 years had the highest rate of ED visits in all five years. From the start of the coronavirus disease 2019 (COVID-19) pandemic in 2020, the incidence rates of ED visits decreased in all age groups, except the group of aged 19–29 years, which maintained an increasing trend. For women, the group of aged 19–29 years showed a steep increase in the rate of ED visits for SA or self-harm from 2016 to 2020 (an average increase of 22.5% per year), regardless of the COVID-19 pandemic. Women aged 65+ years had the lowest rate of ED visits among all age groups. In Supplementary Table 4, the annual trend of ED visits for SA or self-harms in the male and female groups of aged 19–29 was significantly increased (P for trend is 0.014).
Mortality related to suicide attempts or self-harm
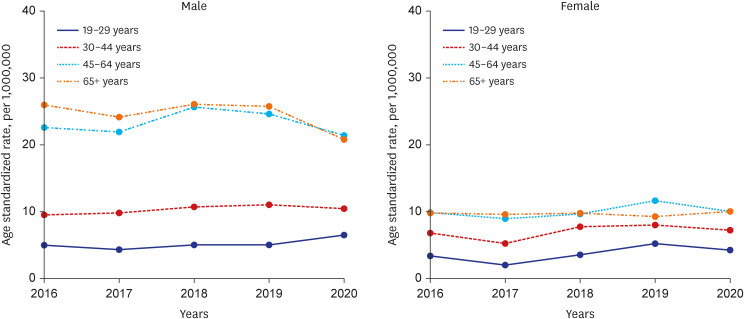
The overall rate of mortality among individuals who visited the ED for SA or self-harm, including death on arrival, death in the ED, and death during hospitalization, is presented in Fig. 3. The mortality rates of men in 45–64 years and 65+ years age groups were significantly higher than those of the two younger age groups. In 2018, the mortality rates of the 45–64 and 65+ years age groups were approximately 2.4 times that of the group of aged 30–44 years, and 5.1 times and 5.2 times that of the group of 19–29 years, respectively. The gap in mortality rate between age groups was smaller in women; however, the mortality rate was higher in the older age groups than in the younger age groups, as in men.
Characteristics of ED visits for SA or self-harm
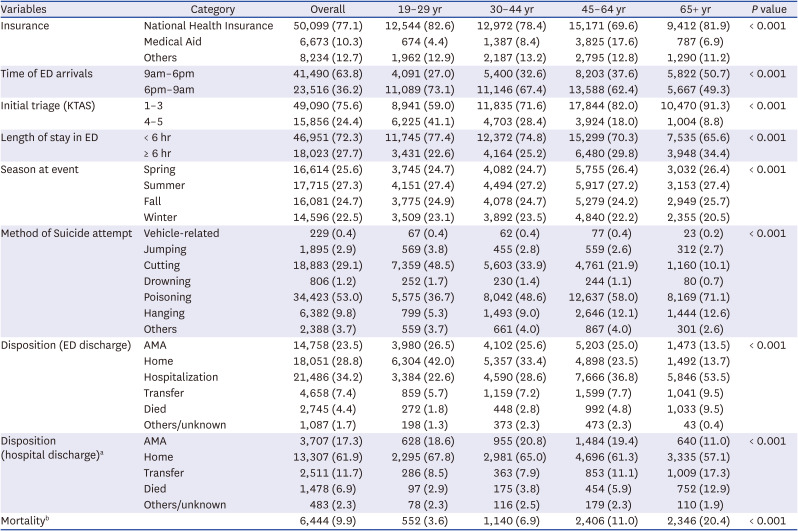
For men, the proportion of patients who did not have National Health Insurance was highest in the group of aged 45–64 years (30.4%) (Table 1). In the older age groups, poisoning was the most common method of SA or self-harm, and daytime (9am–6pm) ED visits were more common than nighttime (6pm–9am) ED visits. Regarding triage, the results showed that the older the age group, the higher the patient's ED priority (the lower on the KTAS) on initial triage and the higher the proportion of patients hospitalized. Discharge from the ED AMA was more frequent in the younger age groups. The proportion of inpatients who were discharged AMA was highest in the group of aged 30–44 years (20.8%). The mortality rate of the oldest age group was 5.6 times that of the youngest age group (20.4% vs. 3.6%). Regarding comorbid conditions, 10.3% of the men had comorbid psychiatric conditions, and the top three diagnoses were depression (53.7%), alcohol use (20.3%), and schizophrenia (9.3%) (Supplementary Table 5).
Table 1
Characteristics of ED visits for SA or self-harm, by male age group (n = 65,006)
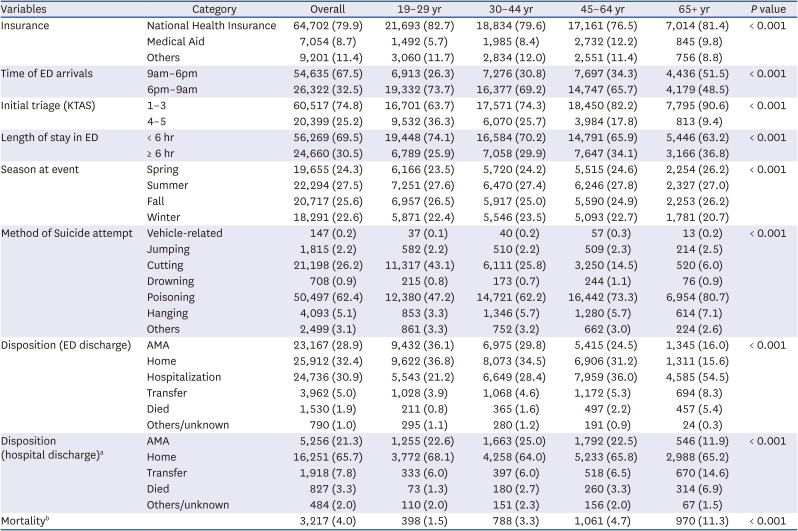
Women showed trends similar to those shown by men in terms of insurance type, method of SA or self-harm, initial triage, and the proportion of patients hospitalized according to age (Table 2). Discharge from the ED AMA was highest in the youngest age group (19–29 years, 36.1%). The mortality of the oldest age group was 7.5 times that of the youngest age group (11.3% vs. 1.5%). Regarding comorbid conditions, 13.8% of the female patients had comorbid psychiatric conditions (Supplementary Table 5). Depression (62.0%) was the most common underlying disorder, followed by alcohol use (9.5%), bipolar disorder (8.1%), and adjustment disorders (8.0%).
Table 2
Characteristics of ED visits for SA or self-harm by female age group (n = 80,957)
DISCUSSION
We investigated the annual trends and epidemiological characteristics of ED visits for SA or self-harm in Korea using a nationwide ED database. The results indicated that the proportion of ED visits for SA or self-harm increased by 37.8% from 2016 to 2020. The overall rate of mortality among individuals who visited the ED for SA or self-harm was 6.6% during the same period. In addition, we analyzed the ED utilization details, disposition, and brief clinical information, such as the KTAS score, of individuals who visited the ED for SA or self-harm. Although we did not include all cases of SA or self-harm across the country, the findings of this study highlight important trends in populations that have a high risk for suicide and will enable ED physicians to properly determine the disposition of such patients.
A major issue highlighted in this study is that the age-standardized rate of ED visits for SA or self-harm in the youngest age group has continued to increase, especially among women, despite the COVID-19 pandemic in 2020. It should be noted that the total number of ED visits in Korea declined substantially during the early COVID-19 pandemic period (Supplementary Table 3), as in other countries.161718
Unlike other age groups, both the number and the rate of ED visits by young women (19–29 years old) increased during the study period. This can be interpreted as an increase in help-seeking behavior owing to heavy mental burden. Studies conducted in the United Kingdom revealed that women, young adults (18–29 years old), and socially disadvantaged groups were especially vulnerable to mental health problems such as suicidal ideation, self-harm, or SA during the early COVID-19 pandemic period.192021 Women and young adults (18–29 years old) experienced higher levels of anxiety, defeat, entrapment, and loneliness at the start of lockdown than men and older adults, respectively.2122 In Japan, the rate of suicide among women younger than 40 years old increased significantly in the late 2020 period compared to the 2017–2019 period, presumably owing to unfavorable psychological and economic conditions.23 It is known that SA at a younger age is likely to lead to repeated SAs,2425 and repeated SA is the strongest predictor of eventual suicide.2627 Psychological support to reduce the incidence of adverse mental outcomes among younger people, especially women, should be provided along with economic support. In addition, diverse efforts to strengthen social ties and restore relationships between individuals at the community level are important.
The results of the present study support the call to pay more policy-related attention to the middle-aged population (aged 45–64 years) as a high-risk group for suicide in Korea. Male patients in this age group had the highest rate of ED visits in the present study, and both men and women had a higher mortality rate owing to SA or self-harm than other age groups, and the highest proportion of individuals on Medical Aid among other age groups (2.1–4.0 times those of other age groups for men, 1.2–2.1 times for women). Many studies have shown that economic difficulties are associated with an elevated risk of suicide, especially in the middle-aged population.2829303132 In the US, the proportion of suicides related to economic crises increased disproportionately among individuals aged 40–64 years between 2005 and 2010.31 In Japan, the suicide rates from 1979 to 2014 stratified according to age showed a pattern of increase in suicide rate with age, after the first peak in the 50–59 years age group.33 These results were observed only in men, and low income and unemployment were estimated to have contributed to the first peak in the rate of suicide.28 The rate of suicide among Korean men aged 40–69 years old increased by 8.0–15.6% annually from 1993 to the late 1990s or the mid-2000s; however, the increasing trend slowed until 2016.34 The sharp increase in suicide rate is presumed to be related to the high economic burden on individuals owing to the structural adjustment of the International Monetary Fund in the late 1990s. However, such increase in suicide rate was not observed in women in the group of aged 40–69 years in the same report. We found that the proportion of the middle-aged population on Medical Aid who visited the ED for SA or suicide has been on the rise, and was highest in 2020 at start of the COVID-19 pandemic (Supplementary Table 6). Thus, preventive measures that include various policies for financial and psychological support are needed for the middle-aged population, particularly middle-aged men in East Asia.
We found that 13.5–26.5% of the men and 16.0–36.1% of the women were discharged from the ED AMA, with the highest proportion in the youngest age group. Not much is known about discharge AMA among individuals who attempt suicide or self-harm3536; however, it is likely to be more common than discharge AMA among all ED visitors.37 Discharge AMA in psychiatric patients involves various factors, including comorbid psychiatric diagnosis, pessimistic attitudes toward treatment, and failure to build a supportive doctor-patient relationship.38 In addition, low awareness of the seriousness of SA, concerns about social stigma, or an implicit bias toward psychiatric treatment may contribute to discharge AMA in the ED. Nevertheless, discharge AMA among individuals who attempt suicide has been noted as a risk factor for eventual suicide.3839 In Korea, policy-related efforts have been made since 2013 to lower the rate of discharge AMA through the effective management of individuals who visit the ED for SA.40 However, the results of the present study consistently emphasize the need for the initiation of additional measures based on the findings of in-depth studies of the drivers and outcomes of discharge AMA.
This study has several limitations and considerations. First, we evaluated the trends in SA or self-harm through the analysis of the rates and numbers of ED visits extracted from a national dataset. Thus, the findings do not represent the overall magnitude of SA or self-harm within the entire population in Korea. Second, as the ED database we used was designed for the improvement of the quality of ED services, the dataset lacks variables that could identify the factors that influence mental health. Studies conducted using additional variables, such as socioeconomic status, family relationships, linkage to the patient’s psychiatric clinic, and information on mental health programs, are needed to understand the factors related to SA or self-harm in populations that have a high risk for suicide. Third, since the present study involved the assessment of anonymized ED visits, repeated visits by the same individual to a single ED or multiple EDs for SA or self-harm could not be identified. Fourth, the overall ED visits were decreased in 2020 due to COVID-19 pandemic, so we should consider the dynamic effect of the pandemic when we evaluated the annual trend of ED visits for SA or self-harm. Even though more consideration of this issue is needed, we wanted to highlight the increase of ED visits for SA or self-harm among young-aged female people. Lastly, the mortality rate of the study population is different from the suicide rate of the National Statistical Office, as intrahospital mortality cases included all deaths of patients who visited ED for SA or self-harm, regardless of death either immediately after arrival at the ED or at the hospital after admission. Therefore, suicide attempt might not be recorded as a direct cause of death on the death certificate in the hospital mortality of the study population. Nevertheless, a significant proportion of the intrahospital mortality was presumed to be contributed by serious injuries from SA; the mortality of the 45–64-year-old group was high enough to be close to that of the 65-year-old or older group, and the relatively high fatality rate among men and the middle-and old-aged group is consistent with the previous results of the fatality rate of SA.
The increasing rate of ED visits for SA or self-harm among young women and the elevated rates of SA or self-harm and mortality among middle-aged individuals are issues of concern. From the perspective of public mental health, it is necessary to plan a suicide prevention program that focuses on improving the limited resources for these populations, with different approaches and considerations depending on age and sex. In addition, the ED should focus on more effective management of SA cases, including provision of appropriate psychiatric interventions, referral for more specialized professional care, linking the patient to a follow-up program, and collaborating with social welfare or private organizations.
 XML Download
XML Download