

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Until the emergence of coronavirus disease 2019 (COVID-19), tuberculosis (TB) was the deadliest infectious disease in the world. In 2020, COVID-19 overtook TB as the infectious disease that caused the most deaths globally. Between 2020 and 2021, global reported deaths due to COVID-19 reached 5.94 million.1 The global number of deaths officially classified as caused by TB in 2020 was 1.3 million.2 Approximately one-quarter of the world’s population is estimated to have latent TB infection (LTBI).3 Its treatment is a critical component of the World Health Organization (WHO)’s End TB Strategy.4 The current COVID-19 pandemic is imposing unprecedented impact to the health systems, with adverse effect being reported on TB services and outcomes.2 In the current public health emergency during which health resources are limited, TB health services is delayed due to reallocation of resources into the COVID-19 response measures. TB preventive services is the first to be suspended based on the assumption that it was less of a priority compared to treatment services. This is an alarming situation as many studies project that such decline in TB case detection and prevention will eventually lead to increased TB mortality in the near future, reversing years of global progress and efforts in the fight against TB.2
During the last two years of the pandemic, experiences from the ground, policy suggestions, and recovery strategies to reverse its impact on the healthcare systems has been increasingly developed and shared.5 Numerous studies have assessed the impact of COVID-19 on individual TB preventive measures, such as Bacille Calmette-Guérin (BCG), LTBI management, TB surveillance, and early detection activities such as contact tracing and case finding. However, there are currently a limited number of studies that analyzed the impact of the pandemic on a full spectrum of TB preventive services in aim to develop sets of policy recommendations recovery strategies. In this regard, this study aims to review the literature on the impact of COVID-19 on TB preventive services. Then, we discussed their recovery strategies and policy options for more effective management of TB in both the pandemic and post-COVID public health landscape.
METHODS
This study is a rapid review of original studies and other scientific literature on the impact of COVID-19 on TB preventive services and relevant policy implications. To conduct this review, we adopted the updated Preferred Reporting Items for Systematic reviews and MetaAnalyses (PRISMA) 2020 statement using the 27-item checklist.6 We further elaborate on other methods of the study below. The detailed methods of a rapid review and search protocol are also provided in the Supplementary Data 1. Ethical approval was not required for this study as this was a review of existing studies.
Search strategy
The formulation of the search question was based on SPICE framework, which is more suitable for investigating outcomes of a health service or policy compared to the traditional PICO framework.7 The question was structured to search literature in the setting of any national, local, and or global settings (S), in the perspectives of policy makers and/or service providers (P), on how the phenomenon of COVID-19 pandemic (I) compared with pre-pandemic (C) impacted the preventive services (E), which include BCG vaccination, LTBI management, TB surveillance, screening, case finding, and contact tracing.
A literature search was conducted using the Medline Database and Embase Database with the following strategy: studies must include “COVID-19” and at least one of the terms associated with TB preventive services mentioned above in the title or abstract. The search included studies published between 1 December 2019 to 30 June 2022. For Medline database search, Medical Subject Headings (MeSH) terms and search texts were used. “COVID-19” search keywords not restricted to “COVID-19” but also included related keywords such as “SARS-CoV-2”, “nCoV”. For Embase database search, Emtree terms and Emtree-preferred terms were used along with general search terms. No filters or restrictions were applied on year, region, and population. The studies analyzing primarily clinical outcomes or molecular level data were beyond the scope of this study and thus were removed from the search by using the Boolean operator “NOT” combined with relevant keywords (e.g., antibody, RNA, clinical trials, immuno*). Regarding the study designs, except for excluding clinical trials in the search protocol, we intended to be as broad as possible and thus did not apply any filters.
Given the rapidly expanding body of evidence and published literature on the impact of COVID-19 on TB services, we also searched for documents released from relevant organizations, such as the WHO, Centers for Disease Control and Prevention, the Stop TB Partnership, among others. Retrieved documents included reports, guidelines, independent studies, information notes, and media statements, etc. As we aimed to be as inclusive as possible of all evidence generated on this issue, reference lists of retrieved documents, from both the peer reviewed studies and gray literature, were reviewed for citation tracking, using forward and backward snowballing. The Peer Review of Electronic Search Strategies (PRESS) 2015 checklist8 was referred to internally. All initial searches were conducted by one of the authors (YJ) in May–June 2022.
Screening and study selection
A total of 221 articles were retrieved from literature searching and citation tracking (Fig. 1). The first and last articles retrieved were published in February 2020 and June 2022, respectively. A total of 95 articles were duplicates included in both the MEDLINE and EMBASE database and 4 articles were duplicates identified otherwise. After removing duplicates, a total of 122 articles were left for initial screening. Two authors (YJ and JM) conducted an independent screening of all titles and abstracts. Our inclusion criteria were that studies must assess the impact of COVID-19 pandemic on TB on at least one of the following TB prevention-related services: 1) BCG or vaccination against TB, 2) detection and treatment of LTBI, 3) TB screening and diagnostics, 4) TB active case finding and/or contact tracing, and 5) TB surveillance. Studies that aimed to solely evaluate a clinical aspect of COVID-19 and TB (e.g., COVID-19 and TB co-infection, susceptibility of COVID-19 in TB patients) were excluded. We also excluded articles that explored the interrelationship of COVID-19, TB, and a third independent factor and also articles that addressed the currently unvindicated hypothesis of the protective effect of BCG against COVID-19. The review process sorted out 26 articles which were not fit for the criteria, which were reviewed once again by one of the authors before final exclusion. A total of 96 articles went under independent, full-text screening by both authors, to evaluate whether they still met the inclusion criteria. After the full-text screening, a total of 93 articles were selected for our review. Complete author agreement of article selection was achieved. No automation tools were used in the process. As articles may have explored the impact of COVID-19 on more than one type of TB service, the numbers may have duplicates and add up to more than the total number of reviewed articles.

Data extraction
From the 93 articles, data were extracted on—title, author, type and year of publication, study setting, estimate of effect, and key findings or policy recommendations (Supplementary Table 1). In the case where the estimate of effect was not quantitative, as in many qualitative studies reviewed, descriptive estimate of effect was collected. The decision on which data is to be extracted was informed by the Checklist of items to consider in data collection or data extraction from the Cochrane Handbook. The extracted data also included all the elements of the research question of this study formulated through the SPICE framework. Data extraction was conducted by a single reviewer (YJ) with verification of a random subset 31 (33.3%) of the results by the second reviewer (JM).
Knowledge synthesis
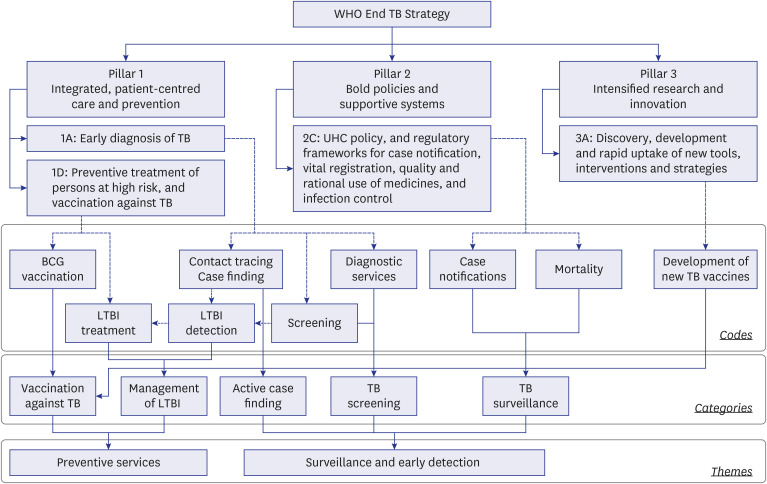
A combination of thematic and framework synthesis methods was applied. A line-by-line open coding was initially conducted independently by both authors on a set of 31 randomly selected articles (33.3%). The resulting codes were then applied in the descriptive theme building process which was guided by the WHO End TB strategy4 as an a priori framework on TB management. The WHO End TB strategy suggests three pillars as essential components of effective TB management, which are 1) TB care and prevention, 2) policies and support programs, and 3) research and innovation. These “pillars” were used as primary themes in the descriptive theme building process. After completion of the descriptive theme building based on the 30 selected articles, the authors went under an iterative process of final theme building. The authors agreed that the three pillars of the WHO End TB strategy respectively encompassed elements that could broadly be considered as preventive measures. Therefore, these preventive measures were selected from the pillars to build final analytical categories, which is as follows: 1) vaccination against TB, 2) detection and treatment of LTBI, 3) TB screening and diagnostics, 4) TB active case finding and/or contact tracing, and 5) TB surveillance. These categories were further worked up to be classified as codes specifying a more detailed programs and activities pertaining to respective categories. Five categories were also grouped into two themes, namely “preventive services” and “surveillance and early detection” (Fig. 2). This final TB prevention thematic framework, developed by the authors, was then applied in the knowledge synthesis of all articles, including the 30 initial articles selected during the theme building process. We analyzed each article to synthesize 1) the impact of COVID-19 on TB preventive services (e.g., changes and/or disruptions in service delivery, coverage, obstacles, and barriers, etc.) and 2) policy recommendation and implications.
Fig. 2
Tuberculosis prevention thematic framework, which was applied in the knowledge synthesis, and their final analytical categories and codes.
Dashed lines indicate selecting preventive measures from each pillar of the WHO End TB Strategy. Dotted lines indicate linking similar characteristics of preventive measures. Solid lines indicate merging codes into categories and themes.
WHO = World Health Organization, TB = tuberculosis, UHC = universal health coverage, LTBI = latent tuberculosis infection, BCG = Bacille Calmette-Guérin.
RESULTS
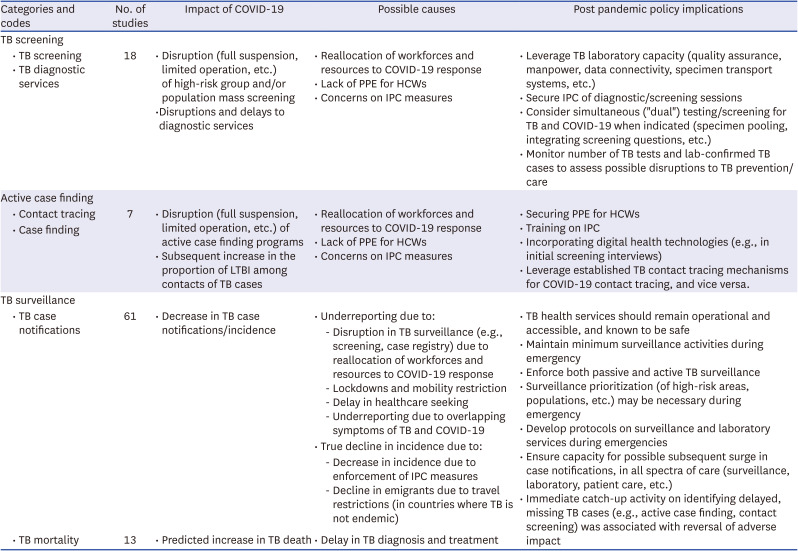
The basic characteristics of the articles selected for review is presented in Table 1. Proportions of original articles increased from 12.9% in 2020 to 29.0% in 2022. TB surveillance (73.2%) was the most common category, followed by the LTBI management (19.4%). In Tables 2 and 3, we present the summary of knowledge synthesis on the impact of COVID-19 pandemic on TB services, possible causes, and relevant policy implications.
Table 1
Basic characteristics of the enrolled articles stratified by each calendar year
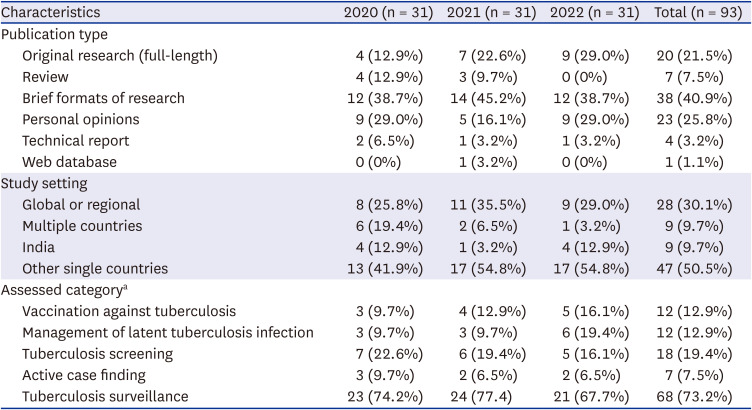
Table 2
Summaries of impacts of the COVID-19 pandemic on tuberculosis preventive services and their recovery strategies

Table 3
Summaries of impacts of the COVID-19 pandemic on tuberculosis surveillance and early detection and their recovery strategies
BCG vaccination
On vaccination against TB, a total of nine articles assessed BCG coverage, all of which suggested that COVID-19 had negatively impacted BCG coverage on a national, regional, or global level. WHO reported that the global TB vaccination dropped from 88% in 2019 to 85% in 20209 while articles from individual countries reported a drop in coverage that ranged from 7% to 60%.1011121314 In Pakistan, the BCG vaccine was the vaccination that showed the highest decline (40.6%) among routine vaccination.11 In one modeling study, the COVID-19-disrupted BCG vaccination coverage was estimated to be a global decline of 25%, with an additional 33,000 TB deaths in children.15 Studies identified healthcare service disruption and movement restrictions regarding COVID-19 responses as the main cause of such decrease in BCG coverage; disruption of immunization services, reduced TB healthcare seeking behavior, fear of COVID-19 infection, movement restrictions, reduction in vaccine shipments due to border closures and air freight restrictions, and instability of the BCG vaccine in the production market.1011121415 Studies generally agree on the concern that such decline in BCG coverage may lead to increased pediatric TB mortality, suggesting routine immunization programs, catch-up activities and/or periodic intensification of routine immunization services,101315 promotion of safe immunization sessions,11 and securing of BCG supply for routine immunization.1617
New TB vaccines
The impact of COVID-19 on the development of new TB vaccines was explored in four articles. A point was raised that the concentration of resources to COVID-19 response may have brought a setback in TB research and new vaccines development, through the research funding gap of US $900 million against a target of US $2 billion, and also by the comparison of US $104 billion spent on COVID-19 during the first year of pandemic and US $5.5 billion spent of TB research during the past decade.1819 While articles also mention that the intrinsic nature of Mycobacteria and the complexity of human immune response against it are additional factors of the relatively slow progress of vaccine development compared to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines,1319 all articles agree that more funding and long-term commitment is needed.13181920
Management of LTBI
Detection and treatment of LTBI was generally negatively affected during the COVID-19 pandemic as numerous articles revealed that new LTBI cases and LTBI treatment has declined during the pandemic,21222324 possibly due to delays in LTBI service or the lower priority of LTBI testing over detection of active TB and COVID-19.2122 WHO reported that there was a 21% reduction in the number of people who were started on TB preventive treatment in 2020, which was a reversion of the positive trend that had been maintained until 2019.2 In a Canadian study, reductions in LTBI treatment initiation rate ranged from 30% to 66%, which showed a higher drop compared to active TB.25 On the other hand, there was one study where maintenance of TB health services resulted in minimal disruption of LTBI treatment and screening.26 On the other hand, articles revealed that there was an increase in the proportion of LTBI among TB contacts during the pandemic, which ranged from 5.9% to 14.3% difference.2728 This trend was more prominent in children as observed through a much higher percentage of LTBI and active TB among children who were household contacts in 2020 compared to 2019 (57.7% vs. 5.3%)29 and less than 30% of TB preventive treatment rate among children under the age of 5 years.230
TB screening
The impact of COVID-19 pandemic on TB testing and screening is revealed to be detrimental. WHO reported that global TB diagnosis declined by 20% in 2020 compared to 2019.2 In single country studies, TB testing decreased by 50% from pre- to post-lockdown in South Africa31 and by 73% from March to April 2020 at a primary referral laboratory in UK.32 This TB diagnosis gap was greater in drug-resistant TB and pediatric TB patients.3334 Such impact in TB testing was suggested to be due to numerous factors including diversion of resources to COVID-19 response, stigma preventing access to diagnostic services, and reduction in laboratory capacity and operations.353637 In a study conducted on a network of 31 national TB reference laboratories in Europe, more than 56% of laboratories experienced “very significant” and “significant” disturbances in its operation in April 2020.38 Numerous countries have diverted GeneXpert for COVID-19 testing amidst the pandemic3539 and this diversion of diagnostic resources is identified as a major cause of decline in TB testing capacities.34353740 However, in Korea with sound public-private partnership, coverage of smear, culture, and drug susceptibility tests among active pulmonary TB patients were not affected during the early phase of the pandemic.41 It is suggested that guaranteeing continuity of TB diagnostic services and leveraging TB laboratory capacity is necessary to ensure TB testing and diagnosis.31323334363740
Active case finding
Like TB testing and screening programs, TB case finding and contact tracing has been impacted by the pandemic, from full suspension of activities in Indonesia to a limited and/or less exhaustive operation in India, China, and Spain.27424344 A single country study in Spain suggested that the limited operation of active case finding and contact tracing amidst COVID-19 might have led to increased transmission within households.27 TB contact tracing is recognized as a labor-intensive process and numerous studies suggested incorporating digital health technologies in its process to promote efficiency.314243 Because infection prevention and control (IPC) of contact tracing and screening sessions was considered as a factor in suboptimal operation of TB detection activities, IPC training, supply of personal protect equipment, and awareness campaigns were also suggested.4243
TB surveillance
A total of 61 articles assessed the impact of COVID-19 on TB case notifications, which is an indicator reflecting an immediate effect of the pandemic on TB management. Although side-by-side comparison is difficult due to different methodologies of respective articles, universal decline in TB case notifications at a global, regional, national, or institutional level is apparent in all articles. WHO estimated that TB cases dropped 21% in 2020 compared to 2019, with 1.4 million people missing out on timely detection.2 Compared to pre-pandemic period, TB case detection declined by 20–80% during the pandemic in Nigeria, Ghana, Ethiopia, Nepal, India, China, Pakistan, Brazil, Korea, Japan, and South Africa.2445464748495051525354 In several studies, a decline in TB cases coincided with national lock-down measures and/or shelter-in-place orders.21225556575859 While in a few studies figures showed a rebound after such measures were lifted2957 or once response measures were rolled-out,60 articles generally stated that such decline in case notification did not resume its pre-pandemic levels even after lockdowns were lifted.4961 Studies from several countries showed relatively minimal disruption to the TB case notification figures, such as a 12% decline in Germany,62 8% decline in Vietnam,63 14.6% decline in a single district in Malaysia,64 and a decrease from an average of 4.7 cases to 4.1 cases per day in UK.65 A modeling study that reflects the current trend of TB case notification revealed that 25% decline in TB case notifications may lead to an additional 190,000 TB deaths.66 Other studies suggest that current disturbances in TB services may result in 201,595 additional TB deaths in China, India, and South Africa67 and 374,000 additional TB deaths in India, Kenya, and Ukraine.68 WHO reported an increase of more than 100,000 TB deaths in 2020 compared to 2019, which was the first transition into an increasing trend since 2005.2
DISCUSSION
This rapid review of literature revealed that the COVID-19 pandemic has had significantly negative impact on the effort to prevent TB, as evident through the universal decline in BCG coverage, detection of LTBI, TB screening and case finding activities, and TB case notifications. Such scale-down of preventive activities is projected to lead to increased TB burden, putting the global TB targets off-track and retreating recent progress at least a decade back. Nevertheless, the current review synthesized policy implications and post-pandemic recovery strategies suggested in respective literature, which could be applied in various regional and national settings in aim to bring TB response back on track.
As the only TB vaccine currently in use, BCG significantly decreases TB deaths in children, through effective protection against military TB and TB meningitis.13 However, it is also well known that provision of routine immunization programs including BCG, and maybe especially the BCG, are vulnerable in public health disaster situations. During the 2014–2016 Ebola virus disease outbreak in West Africa, BCG was the most prominent contributor to the total vaccine stock out, contributing 54% of the total facility-days of stock-outs in one study.6970 Similar situation is ongoing with the current COVID-19 pandemic.
To prevent further decline in BCG coverage, it has been suggested that routine immunization services be maintained as much as possible, with strengthening of immunization registries which can aid in real time monitoring of immunization rates.2 With regards to IPC and immunization safety, immunization sessions and delivery modes should be strengthened to ensure IPC through provision of adequate personal protective equipment, separated immunization sessions, drive-through services, and public campaigns on the safety and necessity of continuing timely routine vaccination even during the pandemic.1115 Benchmarking the global cooperation on the development and distribution of the SARS-CoV-2 vaccines, efforts should be made by states and relevant international partners to secure BCG stocks through political support and international cooperation.1617 Immediate catch-up vaccination or periodic intensification of immunization services has been recommended in critically affected areas to recover coverage rates and minimize duration of delay.1013
One situation specific to COVID-19 is the assumption regarding the protective effect of BCG against COVID-19 infection, which may be negatively affecting procurement of BCG vaccination in parts of the world.161771 As it is beyond the scope of this study, this review did not assess articles that have explored this hypothesis. However, as of April 2020, WHO stated that there is no evidence that the BCG vaccination is protective against COVID-19 infection, and numerous articles have warned against unnecessary BCG administration that might disrupt routine immunization services amidst the pandemic.
Numerous articles suggested that diversion of resources to the COVID-19 research and development could be a contributing factor in the delayed progress in TB research and new vaccines development, as evident through the growing research funding gap in TB.1819 While BCG is the only currently available TB vaccine in use for a century, its efficacy in protection against pulmonary TB and TB re-infection in adults and adolescents is controversial, thereby putting demand on new TB vaccines.1318 With several TB vaccine candidates in the pipeline, reviewed articles equally suggest that the experience of the global society in the development of SARS-CoV-2 vaccines should be applied in the development of TB vaccines, which include rapid multi-disciplinary and multi-national cooperation, successful public-private partnerships, experience with the vaccine platform, innovations in trial designs and endpoint selection, and fund sharing.131872 Commercial-scale manufacturing should be discussed and tuned early in the clinical development process to ensure timely market distribution following efficacy trials.
This review revealed that the COVID-19 pandemic has disrupted LTBI-related services, such as surveillance, case finding, and contact tracing, with a generally higher frequency and magnitude compared to active TB. It caused under-diagnosis of LTBI and reduction in its treatment initiation. Because TB preventive therapy is one of the critical components in the TB management strategy, the current impact of COVID-19 on LTBI management is especially alarming, as we observe an increase in the proportion of LTBI among TB contacts and higher percentage of LTBI and active TB among household child contacts.272829 The combined effect of the lower BCG coverage rate and increased LTBI among children may lead to amplification in pediatric TB burden in the near future. It is suggested that TB health services remain functional and early detection activities be maintained even at a minimum level during emergencies.21222527 During the pandemic, established TB contact tracing mechanisms could be leveraged for COVID-19 contact tracing, vice versa. In post-pandemic situations, catch-up activities to identify missed cases, strengthening of household contact tracing in response to the increased LTBI, and enforcing LTBI in targeted population groups are necessary.232873
The “dual” or “bi-directional” screening for TB and COVID-19 during the pandemic has been suggested as an integrated model of service delivery, optimizing the use of limited diagnostic and laboratory resources during the pandemic. With 5% TB prevalence among COVID-19 patients, this dual testing may be an efficient diagnostic strategy that could support both diseases, when applied with strict indications and quality control measures.7475 At the same time, there are concerns surrounding the possibility of suboptimal diagnosis for both diseases in settings where laboratory capacity is weak.3537 To minimize any negative impact on TB diagnosis and detection, capacity planning should be carefully conducted, including the details of supply chain management, specimen transport, operating procedures of specimen pooling, equipment maintenance, training and protection of human resources, monitoring of laboratory burden and strategies to deal with any overburden.
The most obvious and immediate impact of the COVID-19 pandemic on TB is the decline in TB case notifications, which is universally evident in global, regional, and national level data. Global TB case notifications have been increasing from 2017 until 2019, which then reversed to a large drop in 2020. What is even more concerning is the fact that such drop in case notifications generally did not resume its pre-pandemic levels even after lockdown measures were lifted.4961 The speculation regarding the cause of the drop in TB notification is a mixture of underreporting of TB cases and a true reduction in TB incidence. Underreporting of TB cases is one that should have been detected but went undetected due to a variety of possible causes, such as disruption of active case finding programs and surveillance systems, overload in laboratory capacity, mobility restrictions due to lockdowns, delay in healthcare seeking, and overlapping symptoms of TB and COVID-19.49515254565876777879808182838485868788 A true reduction in TB incidence might be the effect of social distancing, lock-downs, strengthening of IPC in congregate settings, and mask use that may have generally decreased transmission of infectious diseases among susceptible individuals.89 In low-burden countries, decline in emigrants due to travel restrictions is also considered as a possible cause of decrease in incidence. Although there is no clear evidence on their attributable risk to the current trend in TB cases, the Stop TB Partnership assumed that physical distancing and consequent reduction in transmission may be attributable to about a 10% decrease in TB case notifications in high TB burden settings78 suggesting that the proportion of under-diagnosis is much greater than any decline in true incidence.
The significance of this decline in TB case notifications is that it is anticipated to bring dire consequences in the long-term, if left un-intervened. Numerous modelling studies equally suggested that the current trend in TB case notifications would direct to a loss of the progress made in the past 8 to 10 years.666768 So, what should be done to mitigate this detrimental impact of COVID-19 on TB? Reviewed articles suggest a common set of interventions that should rapidly and sustainably be conducted, which include: maintaining and leveraging TB detection services (e.g. contact tracing, screening, laboratory services), support the provision of TB preventive treatment services with TB/COVID-19 detection, incorporating digital technologies in TB detection activities, awareness campaigns on the necessity and safety of TB health service seeking, developing and applying operation protocols for TB surveillance during emergencies which include details regarding prioritization of activities, resource allocation, and post-emergency recovery strategies. Considering that the volume of missed TB cases is large and its long-term impact may be devastating, a catch-up activity on identifying these cases (e.g., temporary intensification of active case finding sessions, household contact screening, self-reporting campaigns) was suggested to reverse adverse impacts.45586068 As possible surge in TB case notifications may occur after social functions and health services are normalized, it is essential to ensure capacity in all spectra of TB preventive services including laboratory, early detection, and patient care services.4463
This rapid review has several limitations. First, because of the rapidly expanding body of evidence on this topic, newer studies that have been published later than our literature search may provide a more precise or different results on the impact of COVID-19 on TB prevention. Second, our search protocol with no restrictions on the study designs yielded more comments and letters compared to original studies to be included in the review. However, unlike systematic reviews of trials and clinical outcomes, in our review which focused on short term policy outcomes in a public health emergency, we saw this as less as a limitation and more of a necessity, in our effort to gather all bits and pieces of wisdom in this global endeavor to overcome the pandemic. Third, we identified articles revealing that additional TB death occurred during the pandemic. However, we could not assess the actual causal relationship between the COVID-19 pandemic and TB mortality, because there are many factors associated with anti-TB treatment outcomes. Further evaluation is necessary to identify impact of the pandemic on treatment outcome, such as mortality, loss to follow-up, and treatment failure.
This rapid review revealed the detrimental impact of COVID-19 on TB preventive services and outcome, which is evident through the decrease in BCG coverage, detection and treatment of LTBI, TB diagnostic services, case finding activities, and TB case notifications. The COVID-19 has threatened TB research and new TB vaccine development; however, the global response of COVID-19 vaccine development offered distinct possibility that TB research in the future could be scaled up significantly. It is critical to ensure the availability of funding to continue and complete critical TB research. We summarized recovery strategies and policy recommendations to maintain or optimize essential TB preventive services during and after the pandemic. These findings and lessons learnt from the COVID-19 pandemic can aid in the development of future national TB control program in order to restore TB services and maintain it robust control.
 XML Download
XML Download