

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Globally, adolescent suicide is a social problem and the second leading cause of adolescent deaths.1 Korea not only has a high adolescent suicide rate but suicide is also the leading cause of adolescent deaths in South Korea.2 There are usually 6–10 survivors for a person who died by suicide.3 According to “a white paper on suicide prevention” published by the Korea Foundation for Suicide Prevention, the average South Korean suicide rate in 10–24 year-olds from 2012 to 2019 was 8.5 persons per 100,000 persons, resulting in approximately 40,000 suicide survivors every year.45 Suicide survivors feel more rejection, shame, loneliness, and social stigma than family, relatives, or friends of people who died by other causes.6 Some develop physical or mental disorders including insomnia, anxiety, depressive disorder, and alcohol dependence. In severe cases, they attempt suicide.678 The ones who lived with or had a close relationship with the person who died by suicide are at a higher risk of developing psychiatric disorders.910 In particular, parent survivors show more post-traumatic stress disorder (PTSD), depression, and psychological problems than parents who lose their children to accidents, natural deaths, and drug abuse.11 They often experience complicated and prolonged bereavement and grieving processes due to parental guilt, shame, shock, and self-blame.12
Most people adjust to the loss without professional intervention.811 Complicated grief (CG) has a global prevalence of 2–3%, and higher (approximately 10–20%) after the loss of a loved partner or child.13 CG is associated with adverse psychological and physical outcomes.14151617 Regarding the psychological aspect,141516 it is associated with reduced quality of life, functional impairment, high-risk behaviors, and suicidal ideation and behaviors, even after adjustment for comorbid depression and PTSD. Regarding the physical aspect,1718 it increases the rates of cardiovascular illness, cancer, and sleep disturbance. Therefore, it is necessary to screen for CG in parent survivors, evaluate the risk factors, and implement preventive measures.
Risk factors for CG include the nature of death, age of the deceased, intimacy level, relationship with the deceased, previous psychiatric history, mental illness (including depression, anxiety, and insomnia), personality traits, coping styles, and socioeconomic status.1920 Depression, anxiety, PTSD, alcohol abuse, and CG increase the risk of suicidal ideation and suicide.20212223 Depression, among several mental disorders, is especially strongly associated with suicide.24 Insomnia is a symptom of depression and, subjectively, the pain felt is high.2425
Most previous studies have focused on insomnia or mental health after the death of an adult or spouse, or have identified risk factors and interventions for CG.21232526 To the best of our knowledge, studies have not examined the mental health of the surviving parents, which also includes psychological autopsies of deceased adolescents. This study aims to evaluate suicidal ideation, depression, and insomnia in surviving parents and examine the psychological factors related to the deceased adolescents using psychological autopsy data from Korea.
Go to : 
METHODS
Materials
This study used data from the Korean Psychological Autopsy of Adolescent Suicide, conducted by the Suicide and School Mental Health Institute, the official student mental health policy-focused research institute of the Korean Ministry of Education. Data from 2015–2021 were used. Psychological autopsy was performed with surviving parents of adolescents who died by suicide before the age of 20 years. Participants were recruited when parent suicide survivors agreed to the psychological autopsy, which was announced by the Korean National Police Agency, Schools, Korea Foundation for Suicide Prevention, the Mental Health Welfare Center, and the Korea Suicide Prevention Center. Trained psychiatrists participated as primary interviewers and trained persons with master’s degree, or higher, in the mental health field participated as assistant interviewers. This study analyzed the psychological autopsies of 35 adolescents who died by suicide and 42 parents (10 fathers and 32 mothers). For seven adolescents, both mother and father participated in the psychological autopsy. In this case, information about deceased adolescents was based on the more reliable parent’s report. This parent was identified through a research team meeting. Interviews with the parents were conducted after a bereavement period of at least one month.272829
Methods
Korean Psychological Autopsy Checklist for Adolescents (K-PAC-A)
The K-PAC-A30 was developed to evaluate suicide status and suicide-related factors in adolescents who died by suicide and in their parents. This tool consists of a semi-structured clinical interview and various psychological assessments. After conducting the interviews, the research team formulates the final diagnosis of the deceased, suicide risk factors, protective factors, and pathways leading to death. The K-PAC-A comprises three parts: 1) Information about the interviewee who is a suicide survivor (socio-demographic information, response to death and adaptive status, and psychological and emotional states with standardized questionnaires after loss); 2) Information about the adolescents who died by suicide (sociodemographic information, developmental history, temperament, relationship with parents, peers, teachers, family related information, school life, personality, coping skills, traumatic experiences, internet and game use, age at the time of death, method of suicide, place of suicide, and diagnosis); and 3) Psychological assessment of adolescents using diagnostic interviews and standardized questionnaires. We used the Patient Health Questionnaire-9 (PHQ-9) and the Korean version of the Insomnia Severity Index (ISI-K) to evaluate the parents’ mental health. For obtaining information and psychological assessment of the deceased adolescents, we used the Korean version of the Barratt Impulsiveness Scale-11 (K-BIS-11) and the Korean version of the Beck Depression Inventory-II (K-BDI-II).
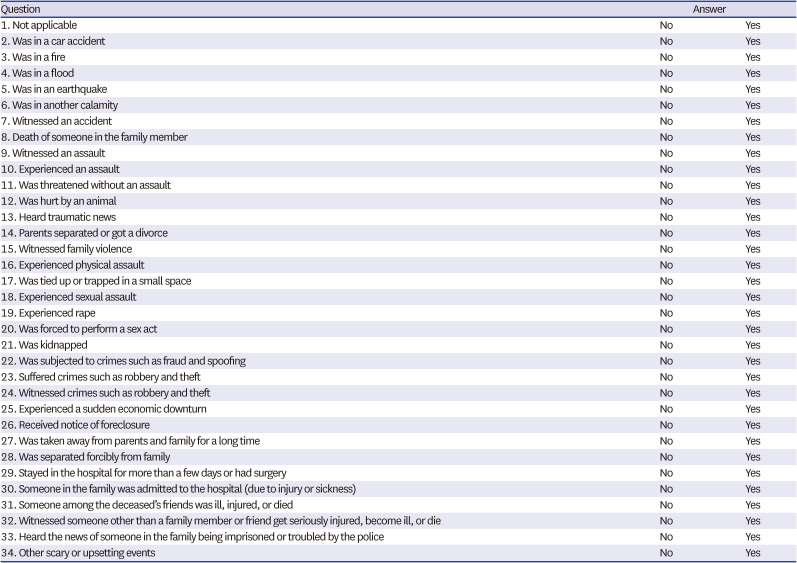
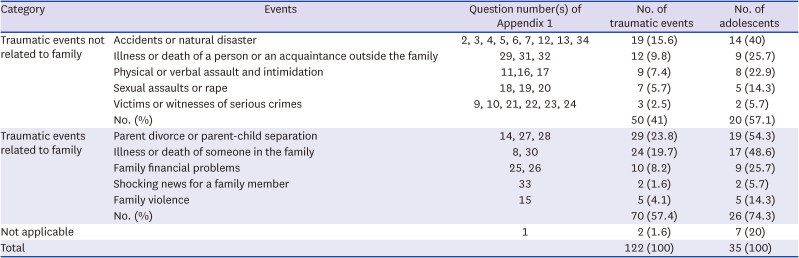
The incidence of traumatic events in adolescents who died by suicide was confirmed by their parents during the K-PAC-A (Appendix 1). We evaluated the various events in detail based on the Lifetime Incidence of Traumatic Events for parents, a tool to evaluate the presence and extent of trauma experienced by children and adolescents.31 It consists of a total of two domains and includes the following contents: traumatic events not related to family (various accidents, natural disasters, illness or death of the person or an acquaintance outside the family, physical or verbal assault and intimidation, sexual assault or rape, and victims or witnesses of serious crimes) and traumatic events related to family (parents’ divorce or parent-child separation, illness or death of someone in the family, family financial problems, shocking news for a family member, and family violence). The parents selected any traumatic events experienced by the adolescents before death. A higher total score indicated greater trauma and loss.
ISI-K
The ISI32 is a self-report assessment that evaluates the severity of insomnia and was completed by the surviving parents to evaluate their insomnia. The ISI consists of seven items, and each item is rated on a scale of 5-point Likert scale. A total score of 15 or more indicates clinically significant insomnia.3334 In the ISI-K,34 Cronbach’s alpha was 0.92; the sensitivity and specificity were 0.92 and 0.82, respectively.
PHQ-9
The PHQ-935 is a self-report assessment used to evaluate depression, and was completed by parent survivors to evaluate their symptoms. It is composed of 10 items, of which nine assess the severity of depression with a total score, and the last item evaluates the degree of functional dysfunction. Each item is rated on a 4-point Likert scale. A total score of 10 or more indicates clinically significant depression.36 In the 9th item of the PHQ-9, indication of more than one point (several days) indicated suicidal ideation.36 In the Korean version of the PHQ-9,36 Cronbach’s alpha was 0.85; the sensitivity and specificity were 0.82 and 0.90, respectively.
Kiddie-Schedule for Affective Disorders and Schizophrenia-Present and Lifetime-Korean version (K-SADS-PL-K)
The K-SADS-PL-K37 is a semi-structured interview tool used to assess symptom severity and morbidity in children and adolescents with 32 psychiatric disorders. Standardization of the Korean version of the K-SADS-PL was carried out by Kim et al.38 In this study, we utilized the K-SADS-PL-K to diagnose adolescents who died by suicide.
K-BIS-11
The BIS-1139 is a self-report questionnaire consisting of 30 items revised by the BIS.40 Parent survivors completed this scale to evaluate the deceased’s symptoms because impulsivity is strongly related to suicide.2124 Each item is rated on a 4-point Likert scale. The total score was the sum of each item. The higher the total score, the higher is the impulsiveness. The K-BIS-11 was standardized by Heo et al.41 Cronbach’s alpha was 0.80, and the test-retest reliability was 0.95.
K-BDI-II
The BDI-II42 is a self-report questionnaire that evaluates the presence and severity of depressive symptoms over the previous two weeks. However, we instructed parent survivors to evaluate the depressive symptoms of the deceased before suicide. It consists of 21 items that assess the cognitive, emotional, motivational, and physical symptoms of depression. Each item is rated on a 4-point Likert scale. The total scores for mild, moderate, and severe depression were 10–15, 16–23, and 24–63, respectively. The K-BDI-II was standardized by Sung et al.,43 and the Cronbach’s alpha was over 0.80.43
Statistical analysis
All statistical analyses were performed using R version 3.5.0 for Windows and Rex (version 3.6.3; Rex Soft Inc., Seoul, Korea), and IBM SPSS Statistics (version 27.0; IBM Corp., Armonk, NY, USA). First, we conducted descriptive statistics to confirm the sociodemographic data of adolescents and their parents such as age, sex, education, job, interview time of death, method of suicide, place of suicide, diagnosis of adolescents who died by suicide, psychiatric treatment history of suicide survivors, incidence of traumatic events, and psychological assessments. Second, we used Spearman’s correlation coefficient (ρ) to examine the relationships between insomnia (ISI-K) and depression (PHQ-9) in suicide survivors, the lifetime incidence of stressful or traumatic events, impulsivity (K-BIS-11), and depression (BDI) in adolescents who died by suicide. Third, the generalized estimating equation (GEE) assessed the association between the incidence of traumatic events and motor impulsivity in adolescents, insomnia, and depressive symptoms in suicide survivors with a statistically significant Spearman’s correlation coefficient. Since parental gender44 and interview time9 after death have been shown to significantly influence depression in parent survivors, they were adjusted as covariates in the GEE. A P value of < 0.05 and 95% confidence intervals not including 0 were considered statistically significant.
Ethics statement
The present study was approved by the Institutional Review Board of Hallym University Sacred Heart Hospital (2016-1044). Informed consent was submitted by all subjects when they were enrolled.
Go to :
RESULTS
Sociodemographic and psychological characteristics of parent survivors and adolescents who died by suicide
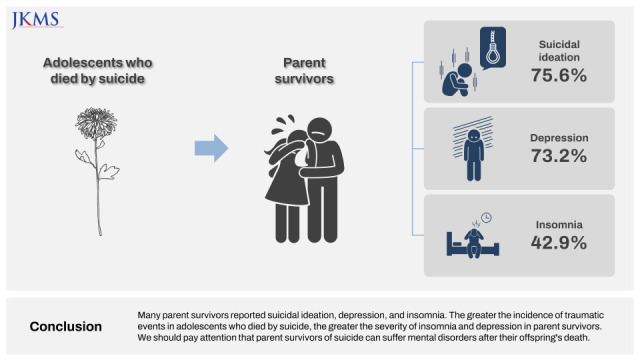
Table 1 shows the sociodemographic and psychological characteristics of the parent survivors. The mean age of the parents was 46.79 years (standard deviation [SD], 4.59), with 32 mothers (76.2%) and 10 fathers (23.8%). A psychological autopsy was conducted with the parents at an average of 7.9 months (SD, 13.3) after the death of their adolescent child by suicide. 18 (42.9%) and 30 (73.2%) parents had clinically significant insomnia and depression, respectively. Many parents (75.6%) were evaluated to have suicidal ideation. The average age at death of the adolescents was 16.11 years (SD, 1.98); 17 deceased adolescents were male (48.6%) and 18 were female (51.4%) (Table 2). At the time of psychological autopsy, 26 adolescents (74.3%) had been diagnosed with depressive disorders, 2 (5.7%) had been diagnosed with bipolar II disorders, and 7 (20%) had been diagnosed with other mental diseases. According to the information provided by the parent survivors, majority of the adolescents had experienced traumatic events (80%) during their lifetime (Table 2). A lot of the deceased adolescents had experienced traumatic events (74.3%) related to their families (Table 2). Additionally, deceased adolescents experienced an average of 3.54 traumatic events (SD, 3.56, range 0–15) before death (Table 2). We have explained, in detail, the trauma experienced by deceased adolescents before death in Appendix 2.
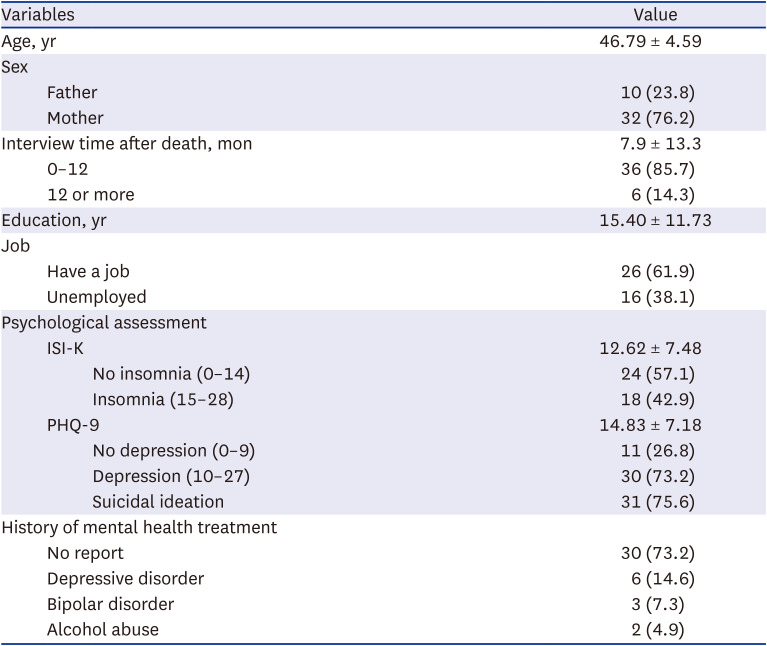
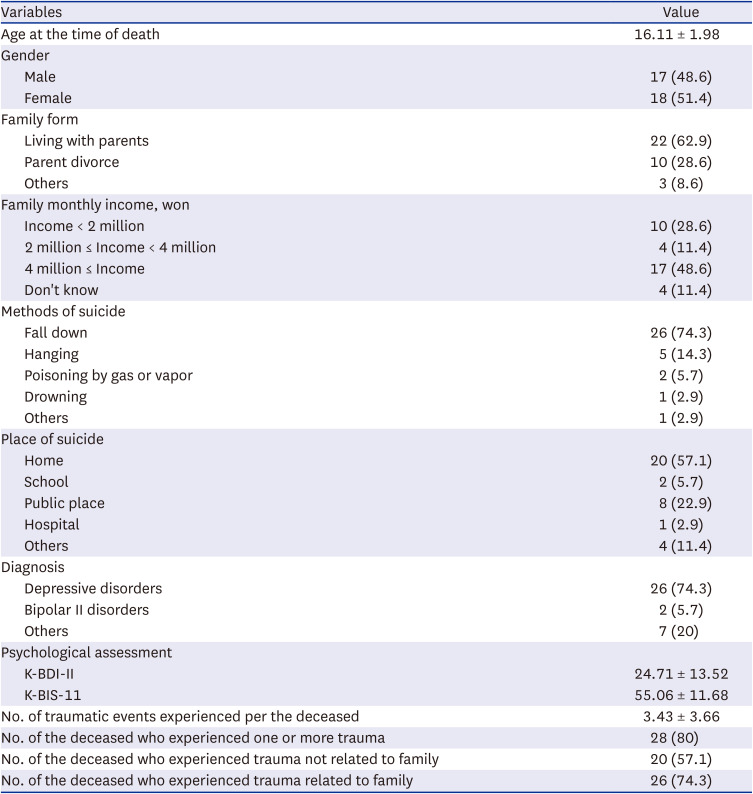
Table 1
Socio-demographic and psychological characteristics of the suicide survivors (N = 42)
Values are presented as mean ± standard deviation or number (%).
ISI-K = Korean version of the Insomnia Severity Index, PHQ-9 = Patient Health Questionnaire-9.
![]()
Table 2
Socio-demographic and psychological characteristics of the adolescents who died by suicide (N = 35)
Values are presented as mean ± standard deviation or number (%).
K-BDI-II = Korean version of the Beck Depression Inventory-II, K-BIS-11 = Korean version of the Barratt Impulsiveness Scale-11.
![]()
Correlation analyses
Table 3 presents the bivariate correlations between variables included in the hypothetical model.

Table 3
Spearman’s correlation coefficients between the study variables (N = 42)
| Subjects | Variables | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|
| Parents | 1. PHQ-9 | - | ||||
| 2. ISI-K | 0.65** | - | ||||
| Adolescents | 3. K-BIS-11 | −0.15 | −0.16 | - | ||
| 4. K-BDI-II | 0.34* | 0.24 | −0.08 | - | ||
| 5. Traumatic events | 0.50** | 0.56** | 0.19 | 0.28 | - |
PHQ-9 = Patient Health Questionnaire-9, ISI-K = Korean version of the Insomnia Severity Index, K-BIS-11 = Korean version of the Barratt Impulsiveness Scale-11, K-BDI-II = Korean version of the Beck Depression Inventory-II.
*P = 0.038; **P < 0.001
![]()
First, the depression scores of parent survivors (PHQ-9) had a moderately positive linear relationship with their insomnia scores (ISI-K) (r = 0.65, P < 0.001). Second, their depression scores had a moderately positive linear relationship with the incidence of traumatic events among deceased adolescents and a weak positive linear relationship with their depression scores (K-BDI-II) (r = 0.50, P < 0.001; r = 0.34, P = 0.038, respectively). Third, the parents’ insomnia scores (ISI-K) had a moderately positive linear relationship with the incidence of traumatic events faced by their adolescent children (r = 0.56, P < 0.001).
Association between insomnia and depression in parent survivors of suicide and the incidence of traumatic events in adolescents who died by suicide
For every increase in the incidence of traumatic events in the deceased adolescents, the depression severity (PHQ-9) of the parents increased by 1.12 (P < 0.001). Furthermore, their insomnia severity (ISI-K) increased by 1.30 (P < 0.001), which was calculated using the GEE method with adjustment for parental sex and interview time after the adolescent’s death (Table 4).

Table 4
Generalized estimating equation between depression and insomnia of suicide survivors and the incidence of traumatic events of adolescents who died by suicide
| Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| B (95% CI) | P value | Adjusted B (95% CI) | P value | |
| PHQ-9 | 1.04 (0.46–1.64) | < 0.001 | 1.12 (0.56–1.68) | < 0.001 |
| ISI-K | 1.23 (0.64–1.82) | < 0.001 | 1.30 (0.91–1.67) | < 0.001 |
Model 1: The generalized estimating equation was performed. Model 2: The generalized estimating equation was adjusted for parental sex and interview duration after adolescent death.
PHQ-9 = Patient Health Questionnaire-9, ISI-K = Korean version of the Insomnia Severity Index, B = regression coefficient, CI = confidence interval.
![]()
Go to :
DISCUSSION
This study investigated depression, insomnia, and suicidal ideation among parent survivors and their relevant risk factors using psychological autopsies in Korea. Several key findings were obtained. 1) The psychological pain of parents who have lost an adolescent to suicide is considerable. Clinically significant suicidal ideation, depression, and insomnia were identified in 75.6%, 73.2%, and 42.9% of parent survivors, respectively. 2) The severity of depression of the surviving parents was positively correlated with their insomnia severity, the deceased adolescents’ depressive symptoms, and the incidence of traumatic events. Overall, the higher the incidence of traumatic events in adolescents who die by suicide, the greater is the severity of insomnia and depression in the parent survivors.
As mentioned above, many parent survivors (75.6%) had suicidal ideation. Suicidal behaviors, including suicidal ideation, were significantly more frequent in suicide survivors than in the general population.945 In previous studies,2146 suicidal ideation was observed in 9–55% of suicide survivors, which is somewhat lower than that in our study. Generally, the greater the perceived stigma surrounding loss by suicide survivors, the greater is the appeal of suicidal ideation.47 Parent survivors face complex and challenging issues such as stigma, shame, guilt, and anger.12 They regard their offspring’s suicide as their failure as parents to raise, nurture, and protect.12 The feeling of hurt in parents is greater than that experienced by close relatives or friends.12 Therefore, it is estimated that our study reported higher suicidal ideation than other studies because the participants of our study were all parents.
Our results showed that many parent survivors (73.2%) had clinically significant depression. In a study on survivors of adult suicides in Korea,21 the average PHQ-9 score was 10.7 (SD, 7.73), and the prevalence of major depressive disorders was 47.1%. Another psychological autopsy study48 showed moderate depression in 28.6% of suicide survivors after the suicide of a family member or close friend. In other studies,4950 15–55% of the bereaved families of deceased individuals who died of a disease had depressive symptoms. The severity of depression is high when the relationship between suicide survivors and the deceased is close.91045 The higher rate of depression in this study compared to previous studies21484950 is presumed to be due to the suddenness of the loss faced by the parents, who were the subjects of this study. Moreover, it is related to the time of psychological autopsy. The severity of depression and grief symptoms in bereaved families is elevated within a short period immediately after loss. It appears to decrease in the first year after the loss,51 and most symptoms have been found to disappear within 3–5 years after the loss.5253 In a study,48 62.9% of participants underwent psychological autopsy after three years. In another study,21 57.7% of participants performed psychological autopsy after two years. In this study, 85.7% of the participants had participated in a psychological autopsy within 1 year of the suicide. Therefore, it can be inferred that there was a difference in the rate of depression between the two studies. In future studies, it will be necessary to assess how mental health evaluations of parent survivors are affected by the period between death and psychological autopsy.
Our study confirmed that 42.9% of parent survivors had clinically significant insomnia. Previous studies2154 also support our findings by confirming insomnia in approximately half of the bereaved families. Many suicide survivors have shorter sleep durations and poor sleep quality.18 Sleep changes during mourning are associated with decreased activity, lifestyle changes related to disengagement from usual activities, and psychological discomfort such as rumination and anxiety due to grief from the loss of a loved one.55 Furthermore, insomnia adversely affects the metabolic, endocrine, and immune systems and increases mortality.13565758 Therefore, suicide survivors should evaluate their insomnia to assess their psychological and physical health.
Another important finding of this study is that the greater the incidence of traumatic events in adolescents who die by suicide, the greater is the severity of depression and insomnia in parent survivors. Previous studies1059 have reported that past traumatic events in suicide survivors increased CG. There have been no studies related to trauma among adolescents. However, adverse life events were related to suicide ideation, but not attempts.60 In our study, the many adolescents who died by suicide experienced traumatic events related to family (74.3%), such as the illness or death of a family member, parental divorce, separation, or parent-child separation, family financial problems, family violence, and shocking news for a family member. This indicates that both, the adolescents and their parents, were experiencing stress and trauma during their lifetime. Traumatic events may negatively affect the mental health of suicide survivors, making them more vulnerable to trauma from offspring suicides. Additionally, parent survivors of suicide may have felt guilty for failing to protect their deceased adolescents from these traumatic events, which may have further contributed to their insomnia and depression.
Our study has several limitations. First, the sample size was small and the control group was not included. There was a lack of representation of adolescents who died by suicide and their parents in Korea. In the future, it will be necessary to conduct continuous psychological autopsies to increase the sample size and re-evaluate the mental health of suicide survivors. Second, this is a cross-sectional study. As the mental health of suicide survivors may change depending on the timing of psychological autopsy evaluation, follow-up is necessary for a certain period. Third, the psychopathology and diagnosis of adolescents who died by suicide were based on parental reports. Because the adolescent’s report of internalized symptoms is more accurate than the parent’s report, the results should be interpreted with caution.
Despite these limitations, this is the first study to use psychological autopsy database of adolescents who died by suicide in Korea to: 1) examine suicidal ideation, depression, and insomnia among parent survivors; and 2) scrutinize the relationship between insomnia and depression among surviving parents and the traumatic events experienced by deceased adolescents.
In this study, many parent survivors reported suicidal ideation, depression, and insomnia. Additionally, we found that the greater the incidence of traumatic events in adolescents who died by suicide, the greater the severity of insomnia and depression in parent survivors. Therefore, it is necessary to pay attention that parent survivors of suicide do not suffer additional suffering from mental health difficulties or CG after their offspring's death. Future research should target a larger sample size to generalize the results of this study. Furthermore, a study observing the long-term course rather than a cross-sectional study is needed to identify risk factors related to CG and suicide risk.
Go to :
 XML Download
XML Download