

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
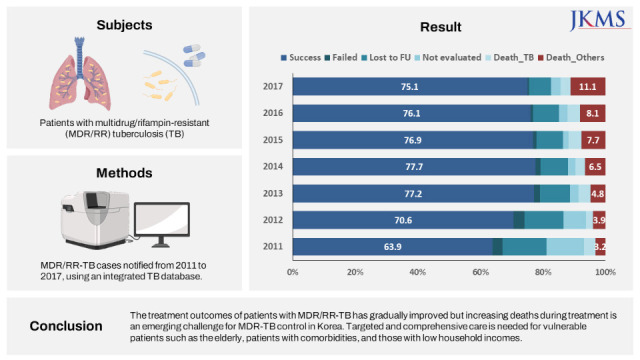
The emergence and spread of multidrug/rifampin-resistant (MDR/RR) tuberculosis (TB) occurs when each step of the TB control program fails to work properly, and these failures are repeated without correction.1 Therefore, the burden and treatment outcomes of MDR/RR-TB are important indicators that reflect the current status of TB management and identify the key challenges encountered by TB control programs in a country.
Over the last decade, considerable progress has been made in the management of MDR/RR-TB in Korea. The annual number of notified MDR-TB cases were peaked at 1,122 in 2012, gradually decreasing to 371 in 2021.2 Based on the findings from several cohort studies in Korea,345 treatment outcomes of patients with MDR/RR-TB seem to improve. In the largest retrospective multicenter cohort study published in 2008,6 treatment success and default rates were only 45% and 32%, respectively. However, recent MDR-TB cohort studies have reported a higher treatment success rate: 82.1% in fluoroquinolone susceptible patients7 and 79.2% in patients using bedaquline and/or delamanid.8
Previously, treatment outcomes of MDR/RR-TB in Korea were estimated from single or multicenter retrospective studies rather than population-based studies.3456 Recently, Lee et al.9 have reported the treatment outcomes of patients with MDR-TB using TB notification data, which was the first published report on nationwide outcomes of patients with MDR-TB in Korea. However, as the notification data contains only minimal information required in the legal format, there are limitations to evaluate various predictors of outcomes such as socioeconomic factors and comorbidity, and to determine post-treatment outcomes such as relapse, retreatment, and long-term mortality.
Although several studies using national statistics related to TB have been published,10111213 few have used an integrated database of various source data. If various national statistical data are properly linked and integrated, it can be utilized as an important tool to evaluate the current situation and identify major challenges of MDR/RR-TB in Korea. We constructed an integrated TB database by linking the Korean Tuberculosis Surveillance System data, the National Health Information Database, and the Causes of Death Statistics databases.14 Using this integrated database, we aimed to evaluate the treatment outcomes and trends of patients with MDR/RR-TB notified from 2011 to 2017, along with predictors of unfavorable outcomes.
METHODS
Data collection
The Korean Tuberculosis and Post-Tuberculosis (TB-POST) cohort was constructed by linking the following three databases14; 1) the Korean Tuberculosis Surveillance System (KTBS) data between 2011 and 2018; 2) the National Health Information Database between 2006 and 2018; 3) the Causes of Death Statistics databases between 2011 and 2018. Data linkage was implemented through the registration number of each data source, which was converted into an alternative personal identification number after linkage to identify subjects from each data source during anonymized analysis.
Study design and population
The present study is a retrospective nationwide cohort study of patients with MDR/RR-TB notified between 2011 to 2018. Patients were selected based on the 10th Revision of the International Classification of Diseases (ICD-10) and phenotypic drug susceptibility testing results. Patients were included by any one of the following criteria: 1) patients with codes U84.30 (MDR-TB), U84.31 (extensively drug-resistant TB, XDR-TB), and U88.2 (arbitrary code for RR-TB), 2) patients who were at least resistant to rifampin on phenotypic drug susceptibility testing.
A treatment episode was defined as a set of consecutive events without treatment interruption more than 2 months.14 If a patient was transferred from one institution and registered with another institution within 2 months, it was considered a continuous treatment episode. On the other hand, if the transferred patient was not registered with another institution within 2 months, it was designated as not evaluated. If a patient underwent multiple treatment episodes, the treatment outcome of the first treatment episode was defined as the final treatment outcome. All patients were followed up for retreatment or death in the integrated database until July 30, 2020.
Definition and measurement
MDR-TB is defined as TB resistant to at least isoniazid (INH) and rifampin (RIF).15 Extensively drug-resistant TB (XDR-TB) is defined as TB resistant to at least INH and RIF plus any fluoroquinolones and at least one of the injectable second-line drugs (amikacin, kanamycin, or capreomycin). The treatment outcomes were defined according to the criteria suggested by the World Health Organization (WHO)15 and reported to the KTBS. The sum of the cured and treatment completed was designated as the treatment success. Unfavorable outcomes were defined as treatment failure, death during treatment, lost to follow-up, and not evaluated. Recurrence was defined as the presence of a new episode of treatment in a patient who was declared treatment success. This includes bacteriologically confirmed cases and clinically diagnosed cases.
Using the phenotypic drug susceptibility testing results at baseline, RR was defined as the case with RIF resistant without any evidence of INH resistant, Pre-XDR categorized as second-line injectable drug (SLID) group with resistant on second-line injectable drugs including kanamycin, amikacin, and capreomycin, and flouroquinolone (FQ) group with resistant on ofloxacin, moxifloxacin, or levofloxacin. Household income was classified into the 5th quintile (1 = the lowest, 5 = the highest) among health insurance beneficiaries, according to the national health insurance premium and medical aid beneficiaries were classified into group 0.
Region was categorized into metropolitan that included a special city (Seoul), Metropolitan cities (Busan, Daegu, Incheon, Gwangju, Daejeon, and Ulsan) and special self-governing city (Sejong), and others that included other provinces except metropolitan. Diabetes mellitus (DM) was defined by at least three claims of ICD-10 code for DM. The presence of human immunodeficiency virus (HIV) and cancer were defined by one or more claims of ICD-10 code for each disease. End stage renal disease was defined cases who submitted claims for any procedure or material associated with either hemodialysis or peritoneal dialysis combined with the ICD-10 code for end state kidney disease (N18.5). Finally, variables may influence the final treatment outcome, including age, gender, nationality, residential region, type of notifying health institutions, previous TB treatment history, lesions site, sputum smear results, sputum culture results, and comorbidities (diabetes mellitus, end stage renal disease, cancer and HIV status) were measured as covariates.
Statistical analysis
Continuous variables are presented as mean (standard deviation) if the variable is normally distributed, otherwise described as median (interquartile range, IQR), and categorical variables are expressed as numbers (percentages). The Student’s t-test if the variable normally distributed or Mann–Whitney test was used to compare continuous variables, and the χ2 test was used to compare categorical variables appropriately. Cochran–Armitage test was used to evaluate annual trends in treatment outcomes. Cox proportional hazard analysis was used to evaluate the predictors of unfavorable outcomes. Variables with P values < 0.2 on univariate analysis were entered into the multivariate models. All P-values were two-tailed, and a P value of < 0.05 was deemed statistically significant. All statistical analyses were performed using STATA/MP version 17 (StataCorp LLC, College Station, TX, USA).
RESULTS
Baseline characteristics
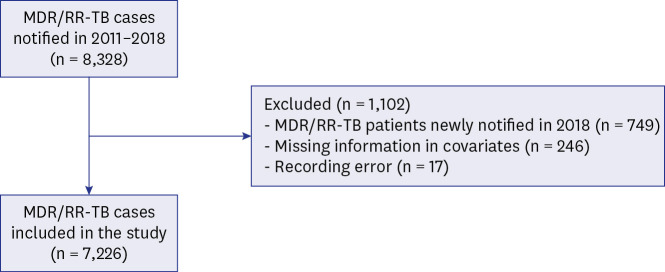
A total of 8,238 patients with MDR/RR-TB were identified in the integrated database (Fig. 1). Among them, the 2018 cohort (n = 728) was excluded because some patients were still on treatment and had a short follow-up period after the end of treatment. In addition, those with record errors (n = 17) and missing information on household income (n = 246) were also excluded. Therefore, 7,226 patients were included in the final analysis.
Fig. 1
Flowchart of selection of patients with multidrug/rifampin-resistant tuberculosis for this study.
MDR = multidrug resistance, RR = rifampin resistance, TB = tuberculosis.
The patients were arbitrarily divided into two groups based on the year of notification, and their baseline demographic and clinical characteristics were compared (Table 1). Compared with patients notified in 2011–2014, the patients notified in 2015–2017 had a higher mean age, and in particular, the proportion of those aged ≥ 75 years was approximately two-fold higher. The patients notified in 2015–2017 had a higher proportion of new patients, extrapulmonary TB, RR-TB, and comorbidities, than those notified in 2011–2014.
Table 1
Baseline characteristics of patients with multidrug/rifampin-resistant tuberculosis by treatment period
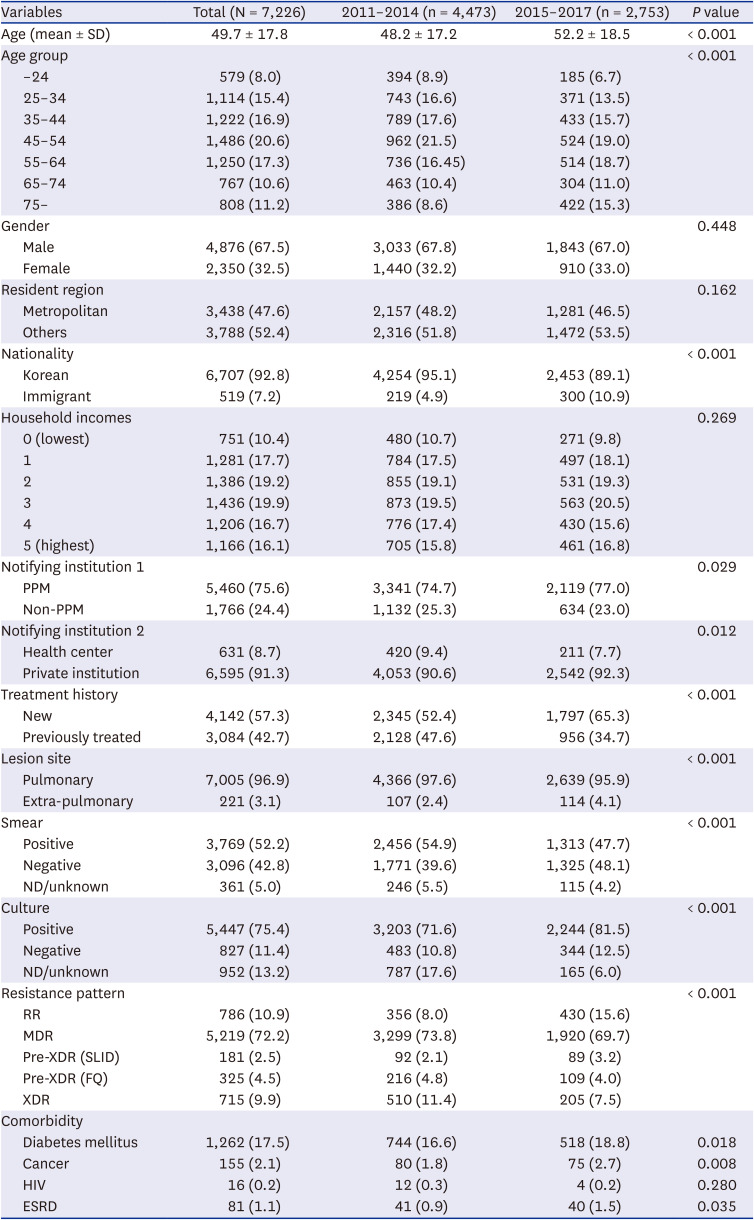
Data are presented as number (%), unless otherwise indicated.
SD = standard deviation, PPM = public-private mix, ND = not done, RR = rifampin resistance, MDR = multidrug-resistance, XDR = extensively drug resistance, SLID = second line injectable drug, FQ = fluoroquinolone, HIV = human immunodeficiency virus, ESRD = end-stage renal disease.
Treatment outcomes and trends
The annual number of notified patients with MDR/RR-TB gradually decreased from 1,340 in 2011 to 802 in 2017 (Table 2). The treatment success rate had significantly increased from 63.9% in 2011 to 75.1% in 2017 (P for trend < 0.001). The highest success rate was observed in 77.7% of patients in 2014 but decreased slightly thereafter.
Table 2
Treatment outcomes of patients with multidrug/rifampin-resistant tuberculosis notified from 2,011 to 2,017

Among unfavorable outcomes, the proportion of patients who failed, were lost to follow up, and were not evaluated gradually decreased (P for trend < 0.001). In contrast, the all-cause death rate during treatment increased gradually from 6.9% in 2011 to 14.5% in 2017 (P for trend < 0.001). The TB-related death rate was not significantly changed (P for trend = 0.513), but the non-TB-related death rate markedly increased from 3.2% in 2011 to 11.1% in 2017 (P for trend < 0.001).
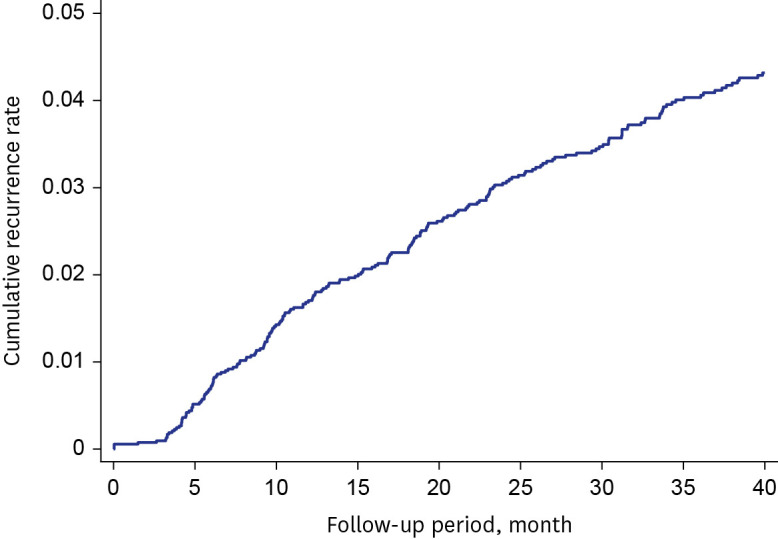
The median follow-up time from the date of treatment completion to July 30, 2020, was 50.7 months (IQR, 31.0–71.2). Of the 5,308 patients who were successfully treated, recurrence occurred in 241 patients (4.5%) at a median 18.4 months (IQR 9.2–32.4) after completion treatment (Fig. 2). Among 241 recurrent cases, the 1-year and 2-year cumulative recurrence rates were 36.6% and 63.2%, respectively.
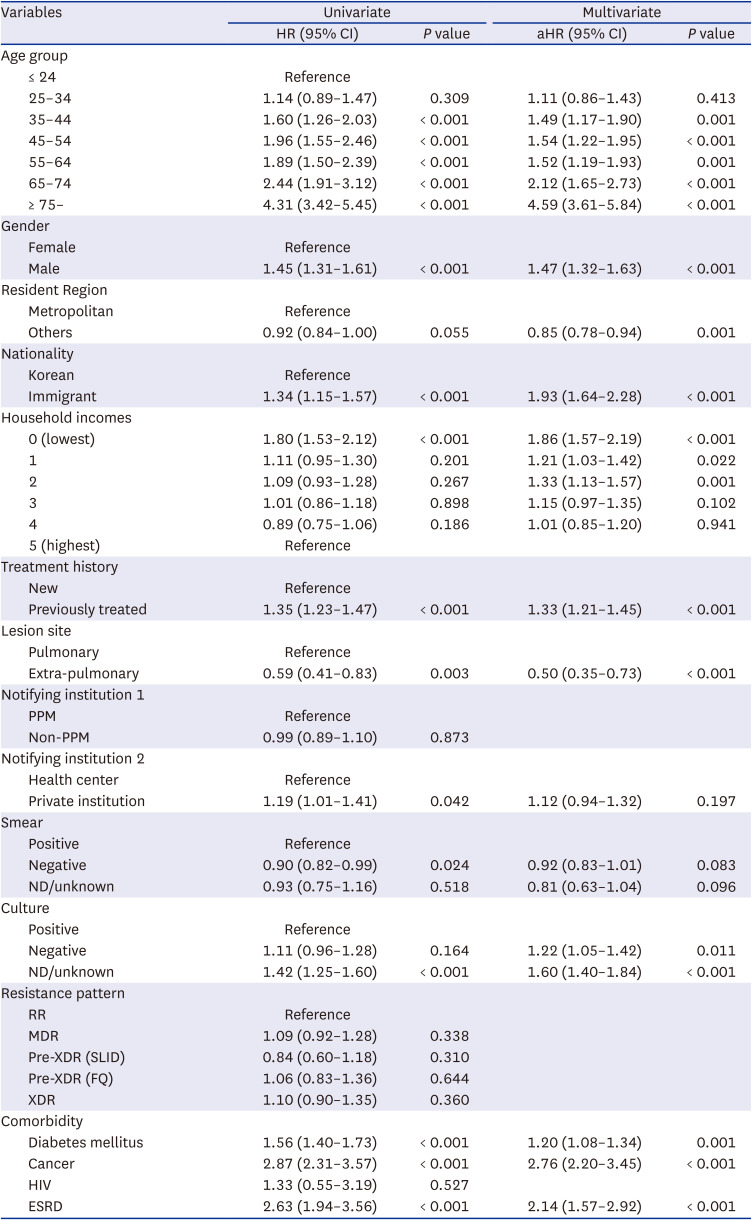
Predictors of unfavorable outcomes
Predictors of unfavorable outcomes were shown in Table 3. In the multivariate analysis, older age, male sex, immigrant, low household income, previous history of TB treatment, and comorbidities were found to be independent predictors of unfavorable outcomes. However, drug resistance patterns and smear-positive results at baseline showed no significant correlation with unfavorable outcomes.
Table 3
Predictors of unfavorable outcomes for patients with multidrug/rifampin-resistant tuberculosis notified from 2,011 to 2,017
Data are presented as number (%), unless otherwise indicated.
HR = hazard ratio, CI = confidence interval, aHR = adjusted hazard ratio, PPM = public-private mix, ND = not done, RR = rifampin resistance, MDR = multidrug-resistance, XDR = extensively drug resistance, SLID = second line injectable drug, FQ = fluoroquinolone, HIV = human immunodeficiency virus, ESRD = end-stage renal disease.
DISCUSSION
In the present study, we simultaneously identified the achievements and new challenges in MDR/RR-TB control in Korea. The achievement of the TB control program was demonstrated by an increase in treatment success rate and a decrease in unfavorable outcomes including treatment failure, lost to follow-up, and not evaluated. This achievement might be due to significant progress in the management of drug-resistant TB over the last decade.16 TB diagnosis is shifting from culture-based tests to rapid molecular tests. In terms of treatment, new and repurposed drugs have become core drugs, replacing injectable and old TB drugs. Recent studies in Korea have revealed that the introduction of molecular drug susceptibility testings17 and the use of new drugs8 have contributed to improving treatment outcomes.
Herein, we found that increasing deaths during treatment, especially non-TB-related deaths, has emerged as a new challenge in Korea. The all-cause death rate during treatment more than doubled, from 6.9% in 2011 to 14.3% in 2017. Among unfavorable outcomes, default accounted for the highest proportion previously,6 however, death currently accounts for the highest proportion. Effective anti-TB chemotherapy can increase treatment success and decrease TB deaths. Several studies conducted in other countries have reported that the use of new drugs has contributed to a reduction in TB deaths.181920 However, in the present study, the treatment success rate marginally decreased since 2015, concurrent with the availability of new drugs in Korea. In a recent study, new drug-containing regimens achieved a treatment success of 79.1% but also presented an all-cause death of 11.9%.8 This study has limitations in determining the impact of new drugs on mortality because the use of the new drug was limited only to some patients during the study period. Further studies using nationwide data are needed.
It is speculated that the increasing non-TB-related deaths could be associated with changing demographic characteristics of patients with TB. In the present study, the proportion of elderly patients and patients with comorbidities increased, and these were found to be independent predictors of unfavorable outcomes. The growing elderly population presents special challenges for TB control in Korea.21 Among new patients with TB notified in Korea in 2021, 51.3% were 65 years or more.2 TB treatment outcomes in older adults are often poor due to delayed diagnosis, increased rates of drug-related adverse events, and frequent comorbidities.2223 Targeted and specific interventions for older populations are urgently needed. It might be controversial to define non-TB related death as unfavorable outcome for TB. Although, the WHO does not distinguish the cause of death in the outcome analysis,15 further studies that classify and analyze deaths according to causes of death are needed to better understand the TB situation.
In this study, low level of household income was an independent predictor of unfavorable outcomes. Various factors may be involved in the impact of social determinants on the treatment outcome of TB.2425 The lower socioeconomic groups have a higher risk of malnutrition, less healthy behaviors (smoking, alcohol abuse) and less likely to seek health care.24 In addition, they likely have more diseases potentially associated TB such as DM, smoking- and alcohol-related conditions, chronic obstructive pulmonary disease, and mental illness.25 In our study, the group with the lowest household income level was the medical aid beneficiaries who had been exempted from direct medical expenses for most diseases, including TB. Our findings suggest that exemptions from direct medical costs alone cannot overcome the impact of socioeconomic differences on outcomes. Therefore, more integrated medical care and active social protection scheme such as sickness benefit, paid sick leave or cash transfer are required.26
This study has strengths in that it is a population-based study covering almost all MDR/RR-TB cases notified in Korea. Hence, the findings of this study are highly representative of MDR/RR-TB situation and applicable to the development of suitable strategies for MDR/RR-TB in Korea. Compared to Lee’s study using the notification data alone,9 we constructed and used the integrated database by linking three national databases. Accordingly, we could analyze more relevant covariates, such as socioeconomic status, and identify long-term recurrence rates. The predictors of unfavorable outcomes identified in the present study could help target high-risk groups and develop specific interventions.
However, our study has also some limitations. First, we could not evaluate the effects of individual drugs and regimens, which are known to be important factors impacting treatment outcomes. Second, although this study was a representative study using the KTBS data, there might be limitations in the accuracy and completeness of the collected data. The KTBS was established in 2000 and some inaccuracies and incompleteness were initially reported.2728 Recently, the completeness and accuracy of data from the KTBS have been gradually improved probably due to strengthened efforts such as the National Public- Private Mix program29 and the national quality assessment program of TB healthcare service.30 Third, we did not distinguish recurrence between clinical and microbiological recurrence, and relapse and re-infection.
In conclusion, the treatment outcomes of MDR/RR-TB are gradually improving; however, the increasing TB deaths poses a new challenge in Korea. Elderly patients, patients with comorbidities, and those with low household incomes were the independent predictors of unfavorable outcomes. Therefore, more targeted and comprehensive approaches should be developed for these vulnerable groups.
 XML Download
XML Download