

 PDF
PDF Citation
Citation Print
Print



The coronavirus disease 2019 (COVID-19) was declared a pandemic in January 2020 by the World Health Organization. The pandemic spread worldwide over the past two years.1 To prevent infection and viral spread, a social distancing and quarantine policy was implemented. However, as the pandemic prolonged, the widening disease burden forced people to adapt to a completely new way of life; daily lives changed instantaneously and interpersonal and community interactions were limited.2 People feared contracting COVID-19 and restricted their daily activities, including meeting family and friends, exercising, and visiting hospitals.
COVID-19 infection fear is a type of health anxiety, defined as worrying about one’s health.3 Nearly everyone experiences COVID-19 infection fear to some degree, and its degrees may influence potential health-related behaviors. Those with high levels of infection fear can perceive bodily sensations or changes as symptoms of infection, but those signs are not limited to infectious disease.4 Infection-protective behaviors can differ depending on the level of COVID-19 infection fear.4
During pandemics, psychological factors are known to play an important role in successful public health management, including awareness of early signs of viral infection, promoting healthy behaviors, and knowledge of protective treatments. Among psychological problems, sex differences are prominent in anxiety disorders characterized by similar fear symptoms.45 Women are more likely to have twice the lifetime rates for most anxiety disorders than men. Additionally, their symptoms are different.6 Women with anxiety disorders reported somatic discomfort due to excessive worrying, while men were more likely to have trouble with interpersonal relationships.7 Although sex differences and comorbid symptoms are reported in psychological problems, the difference in COVID-19 infection fear remains uncertain.
A quantile regression model allows assessment of the distribution of COVID-19 infection fear. It explicitly informs whether risk factors are associated differentially across its distribution. People with high levels of fear have trouble in health-related behaviors and social interaction. Thus, it is necessary to know the risk group for COVID-19 infection fear and provide early intervention. This study aims to explore in-depth the inferences of distribution changes of COVID-19 infection fear with sex differences and provide evidence to assist in policymaking for COVID-19 public management.
The present study analyzed the dataset of the survey of COVID-19 related to negative psychological states (i.e., infection fear, depression, and functional impairment), conducted by the Jeju mental health welfare center in Jeju, Korea. Data were collected from June to July 2021, and this was a period when the COVID-19 pandemic, where the 4th wave began to thrive, and the high-intensity social distancing policy continued for several months. A quota sampling strategy was used to collect data, and the sampling was considered appropriate for ensuring proportionality in terms of age and sex. The study sample comprised 500 community-dwelling adults, aged 20–69 years, living in Jeju, Korea. Informed consent was obtained from all of the participants included in the study. Surveys missing responses to any sociodemographic questions or with no responses to over half of the questionnaire items were excluded; thus, 483 participants were included in the final analysis.
The survey comprised self-report questionnaires. Sociodemographic data were collected, including age, sex, marital status, education, monthly income, and employment status. COVID-19 infection fear was assessed using the COVID-19 Infection Fear Scale (CIFS) developed by the Korean Society for Traumatic Stress Studies.8 The CIFS scale consists of nine related items on a 4-point Likert scale, with scores ranging from 0 to 27. The Cronbach’s alpha of the CIFS in this study is 0.91. Depressive symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9),9 a reliable and validated measure for examining depression severity over the previous two weeks. The PHQ-9 consists of nine related items on a 4-point Likert scale, with scores ranging from 0 to 27. The Cronbach’s alpha of the PHQ-9 in this study is 0.86.
First, the χ2 and Mann-Whitney U test were conducted for the difference comparison between COVID-19 infection fear and depressive symptoms by sex. Second, quantile regression was used to explore the regression relationship of COVID-19 infection fear and sex. Because the levels of COVID-19 infection fear have a non-normal distribution, quantile regression was used to estimate the median difference by sex and to quantify the percentile variation of the effect of sex on fear. Considering the factor distribution, the 10th to 90th percentile of conditional quantile points were described as the quantile regression analysis range. Each of the nine regression analyses were adjusted for depressive symptoms. Stata statistical software v13.0 (StataCorp LLC, College Station, TX, USA) was used to analyze the data and a P value < 0.05 was considered significant.
Of the 483 participants included in the analysis, 241 (49.9%) were male and 242 (50.1%) were female. Among men, 129 (53.5%) were 20–49 years old, and 112 (46.5%) were 50 years old or above. Among women, 126 (52.1%) were 20–49 years old, and 116 (47.9%) were 50 years old or above. Employment status significantly differed by sex (P < 0.001), while the remaining general characteristics were not statistically significant by sex, including age, marital status, household income, and education.
The median score of CIFS in men was 17 out of 27 (interquartile range: 13–21) and that in women was 18 out of 27 (interquartile range: 16–22). There was a significant difference in the CIFS between the sexes (P = 0.001) (Table 1). The median score of depressive symptoms in men was 1 out of 27 (interquartile range: 0–4.5), and that in women was 2 out of 27 (interquartile range: 1–6). There was a significant difference in depressive symptoms between the sexes (P = 0.008) (Table 1).
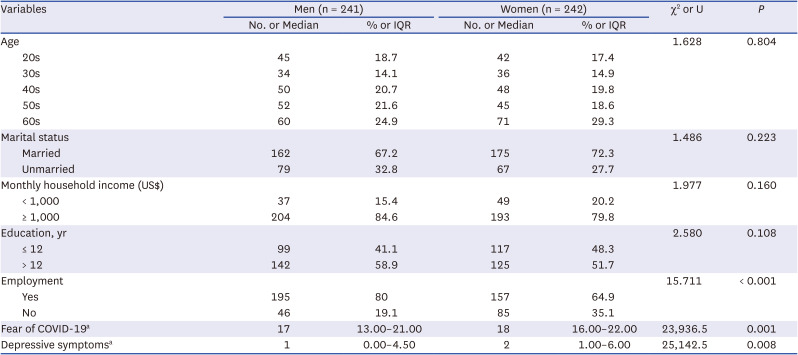
Table 1
Sex differences of variables
![]()
Fig. 1 shows the distribution of the CIFS by sex. Coefficient estimates and associated P values for each of the nine quantile regression models are described in Table 2. Each coefficient describes the increase in the given quantile of CIFS associated with sex difference. While the median CIFS differences between the sexes was not significant (β = 0.71, P = 0.162), differences at the 20th and 30th percentiles were significant (β = 2.04, P = 0.006; β = 1.5, P = 0.004, respectively). The results indicate that sex differences in the level of CIFS were substantially larger at the mild level. For the low level of the quantile regression model, women were more likely to experience COVID-19 infection fear compared to men.

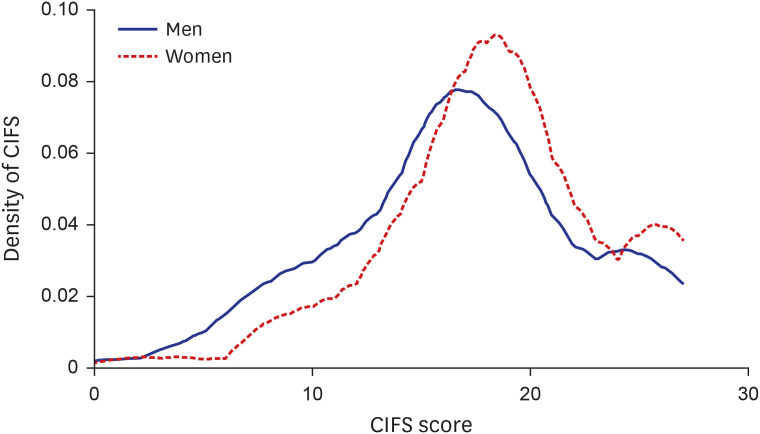 | Fig. 1Distribution of COVID-19 infection fear by sex.COVID-19 = coronavirus disease 2019, CIFS = Coronavirus Disease 2019 Infection Fear Scale.
|
Table 2
Regression coefficients and P values for the nine quantile regression models
![]()
The survey results indicated that the median level of COVID-19 infection fear was 17 out of 27 in men and 18 out of 27 in women. These moderately-high levels of CIFS scores were higher than those assessed in the previous year (2020) in Korea with the same measurement (mean score 12.14). Moreover, this study’s participants reported much higher levels of fear than those surveyed in the same region in the previous year (mean score 12.0).8 In other countries too, respondents were fearful; a study conducted in the United States reported an average score of nearly 7 on a scale of 10.10 Respondents in Eastern Europe and Spain used the worldwide validated Fear of COVID-19 Scale, and their fear score was moderate, with mean values of 17.2 and 16.8 out of 35, respectively.1112 It is difficult to directly compare the infection fear level in this study with that of other studies as different instruments were used. The prolonged and extraordinary situation of the COVID-19 pandemic can induce fear among people, likely due to continued social distancing policies and increased prevalence of infections in this period.
The quantile regression results confirmed that sex is a significant predictor of COVID-19 infection fear. An individual’s sex may have had a disproportionately stronger effect at the mild levels of COVID-19 infection fear. Women experience greater impact of COVID-19 infection fear than men at a low quantile indicating a mild level of fear. These results were consistent with the findings of previous studies on infection fear.13141516 Given the risk of infection fear among women, further research in this context is needed.
Although this study focuses only on sex differences in COVID-19 infection fear, previous research found that infection preventive behaviors, including adopting preventive hygiene and social distancing, differed depending on sex.17 Furthermore, more educated and well-informed people experience less COVID-19 infection fear.15 These results emphasize the importance of providing women with correct COVID-19 health information to reduce fear and promote infection protective behaviors.
The present study has several limitations. First, a cross-sectional research design was used, limiting the inference of causality among the variables. Second, when measuring the COVID-19 infection fear, the timing and location of the investigation may have decisive influences. This study was limited to people in a community setting, thus limiting generalizability for those in other regions. Third, self-report questionnaires were used, which may risk response bias as it was not yet verified.
To prevent COVID-19 fear, we must know the risk factors of those who are overly fearful of COVID-19. Further research is necessary to examine whether potential risk factors can influence COVID-19 infection fear. Additionally, health professionals can help reduce COVID-19 infection fear in adults through interventions, including targeted education.
 XML Download
XML Download