

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Disasters are increasing in frequency and ferocity worldwide. Over the past decade (2010–2019), 2,850 natural disasters, including typhoons, floods, heavy snowfalls, and earthquakes, have affected almost 1.8 billion people [1]. Disasters commonly affect evacuees’ food and nutrition intake [23].
When a disaster hits, health problems can occur due to a lack of water or food, confusion in eating patterns, and other various problems. There are concerns that the food procurement conditions and food environments will affect peoples’ health problems [4].
Nutrient deficiencies must be considered to help prevent health problems in the event of a disaster. During disasters, protein-energy malnutrition is likely to be a major health problem and one of the top causes of death [56]. Micronutrient deficiencies often occur in evacuees [67]. Evacuees appear to have more deficiency diseases, i.e., scurvy caused by vitamin C deficiency, beriberi caused by thiamin deficiency, and pellagra caused by niacin deficiency [7]. The length of time until the appearance of symptoms varies widely depending on the individual health status. Prompt responses and support based on nutritional standards are needed to maintain evacuees’ health conditions.
Nutritional standards can be divided into 2 types: nutrient-based standards and food-based standards. The nutrient-based standards present the reference values of energy and nutrients. The food-based standards present the frequencies and amounts of food or food groups. As the nutritional standards for school lunches, countries have nutrient-based, food-based, or both types of standards. The United States has nutritional standards for school lunches that combine nutrient-based and food-based standards [8]. In Europe, 17 countries in the European Union and Switzerland have both standards [9]. The Republic of Korea (South Korea) and Japan have nutrient-based standards only [1011]. England and France have food-based standards only [1213].
During disasters, nutritional standards play an essential role in maintaining the evacuees’ health. They are useful for preparing food stocks or emergency packaged food. They can also be used to plan menus and provide meals at institutional food services and shelters. The Japanese Ministry of Health, Labour and Welfare set the nutritional requirements to plan and evaluate the meals in shelters [14]. Furthermore, the National Institute of Health and Nutrition in Japan presented food composition examples of meals in an emergency shelter [15]. The World Health Organization (WHO) published a manual for meeting nutritional requirements and assessing nutritional status in emergencies [5]. The United Nations High Commissioner for Refugees (UNHCR) also published guidelines to provide practical tools for estimating food and nutritional requirements in emergencies [6].
Natural disasters, including heavy rain, typhoons, and extreme heat, affected 202 thousand people and caused 3.5 billion won worth of damage in South Korea from 2010 to 2019 [16]. A guideline for operating temporary residential facilities for evacuees affected by disasters in South Korea was published [17] and rules for specific requirements regarding the duration of providing meals were also regulated [18], but no nutritional requirements were included in the guideline or rules.
Preparation for disasters by developing nutritional standards is needed to respond quickly to situations prone to confusion, i.e., the early stages of disasters. WHO, UNHCR, and Japan have nutrient-based nutritional standards for disasters [5614]. However, dietary reference intakes, population structure, and usable data vary from country to country.
During disasters, food-based nutritional standards might be more useful than nutrient-based standards. However, dietitians in South Korea generally use nutrition software to plan menus according to nutrient-based standards. Nutritional standards for school lunches were also established as nutrient-based standards in South Korea [10]. Therefore, this study developed nutrient-based nutritional standards for foodservice at shelters during disasters in South Korea.
SUBJECTS AND METHODS
The standards were developed in 2 phases. In the first phase, nutrients to be included in the standards were selected. In the second phase, the reference values of energy and each nutrient per day were calculated. The developing process used by a previous study [19] was followed for the main framework, and the details were modified according to the purpose of this study.
Phase 1. Selection of nutrients
Fig. 1 presents the selection procedure for the nutrients to be included in the standards. Nutrients were included as initial candidates considering 3 aspects, and some of them were excluded for 3 reasons.
Fig. 1
Selection procedure for target nutrients to be included in the nutrient-based nutritional standards during disasters in South Korea.
KDRIs, Dietary Reference Intakes for Koreans.
1)Nutrients with insufficient intake from the results of studies on food and nutrition status during disasters.
2)Nutrients with insufficient or excessive intake among South Koreans using the Korea National Health and Nutrition Examination Survey [20].
3)Nutrients whose intake data were not available in Korea National Health and Nutrition Examination Survey.
4)Nutrients whose values presented by KDRIs are difficult to achieve based on the current diet among South Koreans.

A detailed description of the procedure to select the initial candidates for inclusion in the standards is presented below. First, the preceding guidelines and manuals on nutritional standards during disasters were collected using Internet search [5614]. These standards were compared based on the following aspects: number and kinds of included nutrients and the reference values for each nutrient. The included nutrients in the preceding standards were selected as initial candidates.
Second, the studies on the nutritional status of evacuees in past disasters were reviewed. Studies in the Google Scholars database were searched. The studies published in English, Korean, and Japanese were searched using the keywords related to nutrition during disasters on March 2021. Nutrients with insufficient intake during past disasters were also selected as initial candidates.
Third, the nutrients with insufficient or excessive intake among South Koreans were reviewed using the data from the Korea National Health and Nutrition Examination Survey (KNHANES) VIII-1 [20]. KNHANES is a population-based cross-sectional survey in South Korea that evaluates the health and nutritional status of South Koreans. Nutrients with insufficient or excessive intake among South Koreans were also selected as initial candidates.
Lastly, the final selection was made by excluding some nutrients for the following 3 reasons. First, nutrients for which there is no deficiency concern in South Korea were excluded. Secondly, nutrients whose intake data were not available in KNHANES [21] were also excluded. Even if the reference values for the nutrients were set, they would not be available. Thirdly, nutrients whose values presented by Dietary Reference Intakes for Koreans (KDRIs) [22] are difficult to achieve based on the current diet among South Koreans were also excluded.
Phase 2. Calculation of reference values
The reference values of energy and the selected nutrients were calculated as population proportion-weighted averages for the entire population who were 1-year-old and over. Additional reference values were calculated for 4 different age groups.
Reference values for energy
Appropriate energy levels were calculated using the estimated energy requirements (EER) formula based on age, sex, height, weight, and physical activity level [2223]. In KDRIs, EER was calculated using the physical activity coefficient of the low active physical activity level category [2324]. The dietary reference intakes for Japanese present EERs in sedentary, low active, and active physical activity level categories to account for individual differences [25]. In the Japanese standards during disasters [14], the energy requirement was calculated using the mean value of sedentary and low active physical activity coefficients based on field surveys at shelters. The physical activity level was reported to have decreased when living in shelters [2627]. Therefore, the appropriate energy levels were calculated using the average of sedentary and low active physical activity coefficients [23], following the Japanese method [14]. The reference heights and weights [22] were used to calculate the appropriate energy levels.
The reference values for energy were calculated using the formula for calculating EER [23] and the age and sex proportion in South Korea of 2019 [28]. The proportion for each age and sex group according to KDRIs [22] was calculated using the data from the 2019 Population and Housing Census of South Korea [28]. The values of the appropriate energy levels (AEMi and AEFi) were multiplied by the proportion (PMi and PFi) for each age group in KDRIs (i) [22]. The reference values for energy were calculated as follows:

where i is the age group in KDRIs;
AEMi is the appropriate energy level of males in the age group i;
PMi is the proportion of males in the age group i;
AEFi is the appropriate energy level of females in the age group i;
PFi is the proportion of females in the age group i.
EER in KDRIs was rounded down to the nearest hundred, considering the obesity rate [23]. However, this might cause a lack of energy intake during disasters. Hence, the reference value for energy was rounded to the nearest hundred. Rounding was performed at the end of these calculations.
Reference values for nutrients
The reference values for each nutrient were calculated using the formula for calculating recommended nutrient intake (RNI) of KDRIs [232930] and the age and sex proportion in South Korea of 2019 [28]. The proportion for each age and sex group according to KDRIs [22] was calculated using the data from the 2019 Population and Housing Census of South Korea [28]. RNI for protein, vitamin A, vitamin C, thiamine, riboflavin, niacin, calcium, and iron (RNIMi and RNIFi) [232930] were multiplied by the proportion (PMi and PFi) for each age group in KDRIs (i) [22]. The reference values for each nutrient were calculated as follows:

where i is the age group in KDRIs;
RNIMi is the RNI of males in the age group i;
PMi is the proportion of males in the age group i;
RNIFi is the RNI of females in the age group i;
PMi is the proportion of females in the age group i.
The reference values for each nutrient were rounded with the same number of digits and the same method of rounding as calculating RNI of each nutrient in KDRIs [232930]. The reference value for protein was rounded up to the nearest multiple of 5 and the reference value for vitamin A was rounded to the nearest multiple of 50. In the case of thiamin and riboflavin, the reference values were rounded to one decimal place. In the case of niacin and iron, the reference values were rounded to the nearest whole numbers. The reference value for folic acid was rounded to the nearest 10. The reference value for calcium was rounded up to the nearest multiple of 50. Rounding was performed at the end of these calculations.
Additional reference values for different age groups
The Japanese Ministry of Health, Labour and Welfare provided additional nutritional standards for different age groups to plan and evaluate the meal provisions in shelters [14]. The reference values for the entire population who were 1-year-old and over would be useful for foodservice at shelters. However, when disasters have stabilized, the nutritional standards for different age groups according to institutional foodservice types would be necessary. Therefore, additional reference values were also calculated for different age groups.
In the KDRIs, the age groups 1-year-old and over are categorized into 11 stages: 1–2, 3–5, 6–8, 9–11, 12–14, 15–18, 19–29, 30–49, 50–64, 65–74, and ≥ 75-year-old [22]. In this study, the different age groups were established considering the simplicity and the range of EER and RNI for protein. The range of EER and RNI of protein for 12–18-year-old adolescents and 19–64-year-old adults were similar [23]. Hence, the 2 age groups were combined. Therefore, the age groups were categorized into 4 groups: 1–5-year-old young children, 6–11-year-old older children, 12–64-year-old adolescents and adults, and ≥ 65-year-old older adults. The reference values of energy and nutrients for the 4 age groups were calculated using the same formula, as described above.
RESULTS
Initial selection of nutrients to be included in the standards
Table 1 lists the preceding nutritional standards during disasters. Energy, protein, fat, vitamin A, vitamin D, vitamin C, thiamin, riboflavin, niacin, folic acid, vitamin B12, calcium, iron, and iodine were included based on the preceding standards during disasters.
Table 1
Nutritional standards during disasters
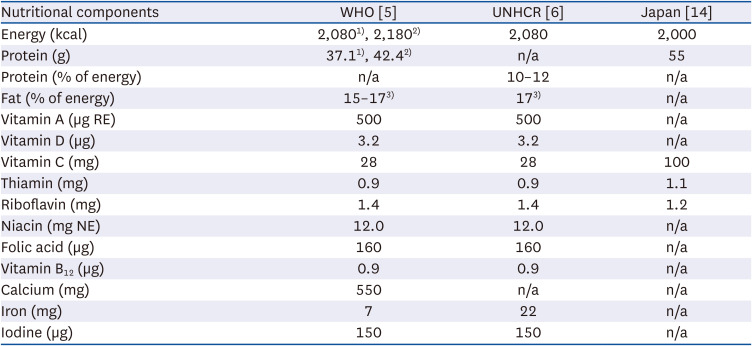
| Nutritional components | WHO [5] | UNHCR [6] | Japan [14] |
|---|---|---|---|
| Energy (kcal) | 2,0801), 2,1802) | 2,080 | 2,000 |
| Protein (g) | 37.11), 42.42) | n/a | 55 |
| Protein (% of energy) | n/a | 10–12 | n/a |
| Fat (% of energy) | 15–173) | 173) | n/a |
| Vitamin A (µg RE) | 500 | 500 | n/a |
| Vitamin D (µg) | 3.2 | 3.2 | n/a |
| Vitamin C (mg) | 28 | 28 | 100 |
| Thiamin (mg) | 0.9 | 0.9 | 1.1 |
| Riboflavin (mg) | 1.4 | 1.4 | 1.2 |
| Niacin (mg NE) | 12.0 | 12.0 | n/a |
| Folic acid (µg) | 160 | 160 | n/a |
| Vitamin B12 (µg) | 0.9 | 0.9 | n/a |
| Calcium (mg) | 550 | n/a | n/a |
| Iron (mg) | 7 | 22 | n/a |
| Iodine (µg) | 150 | 150 | n/a |
WHO, World Health Organization; UNHCR, United Nations High Commissioner for Refugees; n/a, not available; RE, retinol equivalents; NE, niacin equivalents.
1)Requirement for developing countries.
2)Requirement for industrialized countries.
3)The percentage of energy from fat was set at the level to meet the requirements of linoleic acid and α-linolenic acid.
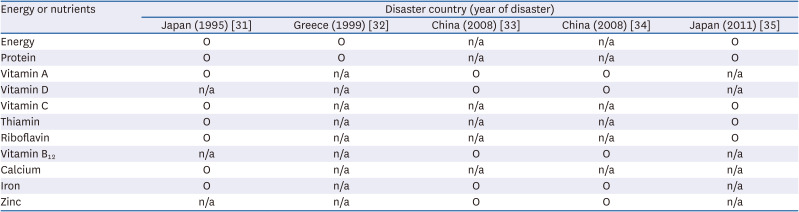
Table 2 presents the nutritional components with insufficient intake through the results of searched studies on the nutritional status of evacuees during disasters. The energy, protein, vitamin A, vitamin C, thiamin, riboflavin, calcium, and iron intake was insufficient one month after the Great Hanshin earthquake in Japan in 1995 [31]. The energy and protein intake was reported to be low in adults and older adults in a study conducted 3 weeks after the 1999 earthquake in Athens, Greece [32]. In China, one year after the Great Wenchuan Earthquake, vitamin A, vitamin D, vitamin B12, iron, and zinc deficiencies were prevalent in children and women of childbearing age [3334]. In 2011, the Great East Japan Earthquake resulted in insufficient intake of energy, protein, vitamin C, thiamin, and riboflavin [35]. Thus, energy, protein, vitamin A, vitamin D, vitamin C, thiamin, riboflavin, vitamin B12, calcium, iron, and zinc were included.
Table 2
Energy or nutrients with insufficient intake by evacuees in the past disasters
| Energy or nutrients | Disaster country (year of disaster) | ||||
|---|---|---|---|---|---|
| Japan (1995) [31] | Greece (1999) [32] | China (2008) [33] | China (2008) [34] | Japan (2011) [35] | |
| Energy | O | O | n/a | n/a | O |
| Protein | O | O | n/a | n/a | O |
| Vitamin A | O | n/a | O | O | n/a |
| Vitamin D | n/a | n/a | O | O | n/a |
| Vitamin C | O | n/a | n/a | n/a | O |
| Thiamin | O | n/a | n/a | n/a | O |
| Riboflavin | O | n/a | n/a | n/a | O |
| Vitamin B12 | n/a | n/a | O | O | n/a |
| Calcium | O | n/a | n/a | n/a | n/a |
| Iron | O | n/a | O | O | n/a |
| Zinc | n/a | n/a | O | O | n/a |
Based on the data from KNHANES, the following nutrients with insufficient or excessive intake among South Koreans were included: vitamin A, vitamin C, riboflavin, niacin, folic acid, calcium, sodium, potassium, and iron [20]. Therefore, energy, protein, fat, vitamin A, vitamin D, vitamin C, thiamin, riboflavin, niacin, folic acid, vitamin B12, calcium, sodium, potassium, iron, zinc, and iodine were included as initial candidates.
Final selection of nutrients to be included in the standards
Final selection was made by excluding nutrients for 3 reasons. Fat was excluded because there is no deficiency concern in South Korea [23]. Vitamin D, vitamin B12, zinc, and iodine were excluded since intake data were not available [21].
Sodium was excluded because chronic disease risk reduction intake of sodium presented by KDRIs [30] were difficult to achieve. [363738]. Potassium was also excluded because adequate intake (AI) of potassium presented by KDRIs were difficult to achieve [36]. AI of potassium was set at the level to prevent hypertension, considering the sodium-to-potassium ratio in the current sodium intake among South Koreans [30].
Finally, energy and 9 nutrients were selected: protein, vitamin A, vitamin C, thiamin, riboflavin, niacin, folic acid, calcium, and iron. Table 3 shows the nutritional components that were included, excluded, and finally selected in determining the nutrients to be included in the nutritional standards during disasters in South Korea.
Table 3
Nutritional components that were included, excluded, and finally selected in determining the nutrients to be included in the nutritional standards during disasters in South Korea
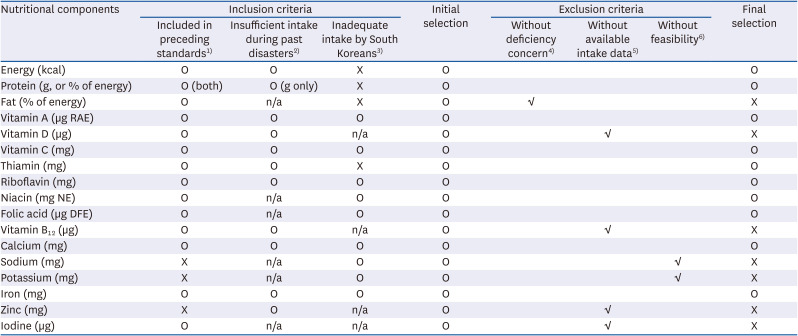
n/a, not available; RAE, retinol activity equivalents; NE, niacin equivalents; DFE, dietary folate equivalents.
1)Nutrients included in preceding standards during disasters.
2)Nutrients with insufficient intake during past disasters.
3)Nutrients with insufficient or excessive intake among South Koreans.
4)Nutrients for which there is no deficiency concern in South Korea.
5)Nutrients whose intake data were not available in Korea National Health and Nutrition Examination Survey.
6)Nutrients whose values presented by KDRIs are difficult to achieve based on the current diet among South Koreans.
Reference values of energy and selected nutrients
Table 4 lists the reference values for energy per day. The average of sedentary and low active physical activity coefficients was used to calculate energy levels in this study.
Table 4
Reference values for energy per day during disasters in South Korea
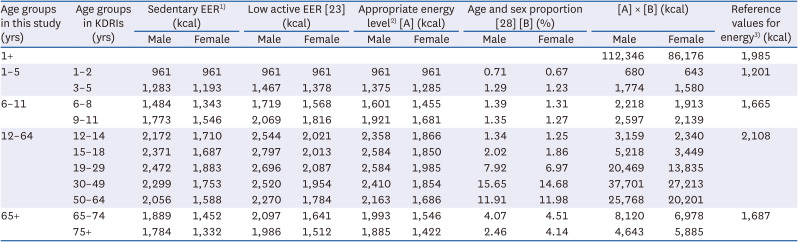
| Age groups in this study (yrs) | Age groups in KDRIs (yrs) | Sedentary EER1) (kcal) | Low active EER [23] (kcal) | Appropriate energy level2) [A] (kcal) | Age and sex proportion [28] [B] (%) | [A] × [B] (kcal) | Reference values for energy3) (kcal) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |||
| 1+ | 112,346 | 86,176 | 1,985 | |||||||||
| 1–5 | 1–2 | 961 | 961 | 961 | 961 | 961 | 961 | 0.71 | 0.67 | 680 | 643 | 1,201 |
| 3–5 | 1,283 | 1,193 | 1,467 | 1,378 | 1,375 | 1,285 | 1.29 | 1.23 | 1,774 | 1,580 | ||
| 6–11 | 6–8 | 1,484 | 1,343 | 1,719 | 1,568 | 1,601 | 1,455 | 1.39 | 1.31 | 2,218 | 1,913 | 1,665 |
| 9–11 | 1,773 | 1,546 | 2,069 | 1,816 | 1,921 | 1,681 | 1.35 | 1.27 | 2,597 | 2,139 | ||
| 12–64 | 12–14 | 2,172 | 1,710 | 2,544 | 2,021 | 2,358 | 1,866 | 1.34 | 1.25 | 3,159 | 2,340 | 2,108 |
| 15–18 | 2,371 | 1,687 | 2,797 | 2,013 | 2,584 | 1,850 | 2.02 | 1.86 | 5,218 | 3,449 | ||
| 19–29 | 2,472 | 1,883 | 2,696 | 2,087 | 2,584 | 1,985 | 7.92 | 6.97 | 20,469 | 13,835 | ||
| 30–49 | 2,299 | 1,753 | 2,520 | 1,954 | 2,410 | 1,854 | 15.65 | 14.68 | 37,701 | 27,213 | ||
| 50–64 | 2,056 | 1,588 | 2,270 | 1,784 | 2,163 | 1,686 | 11.91 | 11.98 | 25,768 | 20,201 | ||
| 65+ | 65–74 | 1,889 | 1,452 | 2,097 | 1,641 | 1,993 | 1,546 | 4.07 | 4.51 | 8,120 | 6,978 | 1,687 |
| 75+ | 1,784 | 1,332 | 1,986 | 1,512 | 1,885 | 1,422 | 2.46 | 4.14 | 4,643 | 5,885 | ||
KDRIs, Dietary Reference Intakes for Koreans; EER, Estimated Energy Requirements.
1)Sedentary EERs were calculated using the sedentary physical activity coefficient and the formula for calculating EER in KDRIs.
2)Appropriate energy levels were calculated using the average of sedentary and low active physical activity coefficients.
3)Reference values for energy per day were calculated as follows:

i, the age group in KDRIs; AEMi, the appropriate energy level of males in the age group i; PMi, the proportion of males in the age group i; AEFi, the appropriate energy level of females in the age group i; PFi, the proportion of females in the age group i.
The reference values for each nutrient were also calculated. Table 5 presents the reference values of vitamin C per day for the entire population who were 1-year-old and over and each age group as an example. The reference value of vitamin C for the entire population was calculated to be 93 mg. The reference values for vitamin C per day were 41, 62, 97, and 98 mg for those 1–5, 6–11, 12–64, and ≥ 65 years of age, respectively.
Table 5
Reference values for vitamin C per day during disasters in South Korea
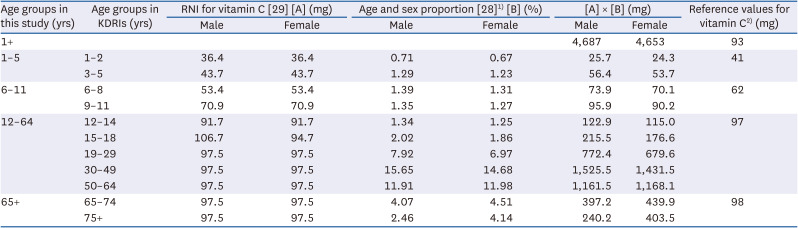
| Age groups in this study (yrs) | Age groups in KDRIs (yrs) | RNI for vitamin C [29] [A] (mg) | Age and sex proportion [28]1) [B] (%) | [A] × [B] (mg) | Reference values for vitamin C2) (mg) | |||
|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |||
| 1+ | 4,687 | 4,653 | 93 | |||||
| 1–5 | 1–2 | 36.4 | 36.4 | 0.71 | 0.67 | 25.7 | 24.3 | 41 |
| 3–5 | 43.7 | 43.7 | 1.29 | 1.23 | 56.4 | 53.7 | ||
| 6–11 | 6–8 | 53.4 | 53.4 | 1.39 | 1.31 | 73.9 | 70.1 | 62 |
| 9–11 | 70.9 | 70.9 | 1.35 | 1.27 | 95.9 | 90.2 | ||
| 12–64 | 12–14 | 91.7 | 91.7 | 1.34 | 1.25 | 122.9 | 115.0 | 97 |
| 15–18 | 106.7 | 94.7 | 2.02 | 1.86 | 215.5 | 176.6 | ||
| 19–29 | 97.5 | 97.5 | 7.92 | 6.97 | 772.4 | 679.6 | ||
| 30–49 | 97.5 | 97.5 | 15.65 | 14.68 | 1,525.5 | 1,431.5 | ||
| 50–64 | 97.5 | 97.5 | 11.91 | 11.98 | 1,161.5 | 1,168.1 | ||
| 65+ | 65–74 | 97.5 | 97.5 | 4.07 | 4.51 | 397.2 | 439.9 | 98 |
| 75+ | 97.5 | 97.5 | 2.46 | 4.14 | 240.2 | 403.5 | ||
KDRIs, Dietary Reference Intakes for Koreans; RNI, recommended nutrient intake.
1)Percentages do not add up to 100 because of rounding.
2)Reference values for vitamin C per day were calculated as follows:

i, the age group in KDRIs; RNIMi, the RNI of males in the age group i; PMi, the proportion of males in the age group i; RNIFi, the RNI of females in the age group i; PFi, the proportion of females in the age group i.
Nutritional standards during disasters in South Korea
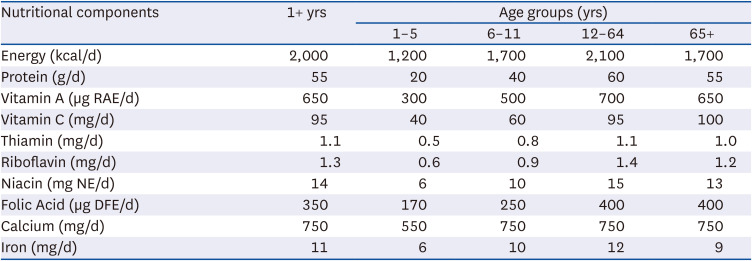
Table 6 presents the nutritional standards proposed in this study. The reference values for the entire population who were 1-year-old and over were calculated to be 2,000 kcal for energy, 55 g for protein, 650 µg retinol activity equivalents (RAE) for vitamin A, 95 mg for vitamin C, 1.1 mg for thiamin, 1.3 mg for riboflavin, 14 mg niacin equivalent (NE) for niacin, 350 µg dietary folate equivalent (DFE) for folic acid, 750 mg for calcium, and 11 mg for iron. The reference values for each age group (1–5, 6–11, 12–64, and ≥ 65-year-old) were also calculated.
Table 6
Nutritional standards during disasters in South Korea
DISCUSSION
The purpose of this study was to develop nutrient-based nutritional standards for foodservice at shelters during disasters in South Korea. Meals need to be provided to evacuees to maintain their health in chaotic and urgent situations, i.e., the early stages of disasters. Hence, nutritional standards should be prepared during non-emergency periods. Therefore, it is essential to develop nutrient-based nutritional standards for use during disasters in South Korea.
Energy, protein, vitamin A, vitamin C, thiamin, riboflavin, niacin, folic acid, calcium, and iron were selected as target nutrients in this study. In the Japanese standards [14], energy, protein, vitamin C, thiamin, and riboflavin were included. The Japanese Ministry of Health, Labour and Welfare provided nutrients and the reference values to secure the required number of meals and the nutritional requirements for 3 months after the Great East Japan Earthquake [1439]. The Nutritional Reference Values for Dietary Assessments and Planning for the Provision of Meals to Emergency Shelter standards were presented 3 months after the Great East Japan Earthquake in 2011 and one month and a half after the 2016 Kumamoto earthquakes [4041]. Vitamin A, calcium, iron, and sodium were also included as special nutrients; vitamin A, calcium, and iron to avoid insufficient intake and sodium to prevent lifestyle-related disease. The selected nutrients in the standards are the same as the results of this study except for niacin.
The selected nutrients in this study were key nutrients to be managed in the school lunches of South Korea. The nutritional standards of school lunches in South Korea include the reference values for energy, protein, vitamin A, thiamin, riboflavin, vitamin C, calcium, iron, and the percentages of energy from carbohydrates, protein, and fat [10]. In both the results of this study and the nutritional standards of school lunches, along with energy, 7 nutrients were included in common: protein, vitamin A, thiamin, riboflavin, vitamin C, calcium, and iron. The percentages of energy from carbohydrates, protein, and fat were included only in the nutritional standards of school lunches, while niacin and folic acid were included only in this study.
In this study, the nutritional standards for 4 age groups in addition to the entire population were suggested. The age groups were categorized into 4 groups: 1–5-year-old young children, 6–11-year-old older children, 12–64-year-old adolescents and adults, and ≥ 65-year-old older adults. The Japanese Ministry of Health, Labour and Welfare also provided the nutritional requirements for 4 age groups to plan and evaluate the meal provisions in shelters [14]; the age groups were 1–5-year-old children, 6–14-year-old growth period I, 15–69- year-old growth period II and adults, and ≥ 70-year-old older adults.
For energy, the appropriate energy levels were calculated using the average of sedentary and low active physical activity coefficients according to the Japanese method [14]. In the Japanese standards, the energy requirement was calculated considering the physical activity level reported in studies on the physical activity level in shelters [2627]. In the case of WHO and UNHCR standards, the energy requirement was calculated for light physical activity as an initial value [56] that must be adjusted, based on the degree of physical activity levels in each country. To the best of our knowledge, no studies have been reported on the physical activity level during disasters for South Koreans. Therefore, the Japanese method [14] was used in this study.
This paper presented protein requirements in grams, this is the same as the WHO and Japanese standards [514]. The UNHCR standards presented protein in the percentage of energy from protein, not in grams [6]. The nutritional standards of school lunches in South Korea are presented in both grams and percentage of energy from protein.
Fat was not selected in this study, like the Japanese standards which did not include fat. On the other hand, in the WHO and UNHCR standards, the percentage of energy from fat was included as fat enhances palatability and provides energy in a highly concentrated form [56]. WHO recommended that fat/oils provide at least 15–17% of the total energy intake to cover certain essential fatty acid (linoleic acid and α-linolenic acid) requirements [5]. However, fat intake is often excessive in developed countries [5]. For instance, there is no deficiency concern in South Korea [23].
Six vitamins were selected in this study: vitamin A, vitamin C, thiamin, riboflavin, niacin, and folic acid. Only 3 vitamins were selected in the Japanese standards: vitamin C, thiamin, and riboflavin [14]. These nutrients were selected as likely to be deficient from the first through the third months after a disaster. The nutritional requirements of vitamin C, thiamin, and riboflavin were calculated based on the recommended dietary allowance (RDA) in the Japanese standards [1439].
Vitamin A was expressed in RAE unit in this study. Vitamin A was expressed in retinol equivalents unit in WHO in 2000 and UNHCR in 2002 because Vitamin A requirements of WHO and UNHCR were derived from a report in 1988; the RAE unit was presented in 2001 [564243].
The reference value of vitamin A for the entire population who were 1-year-old and over was calculated to be 650 µg RAE in this study. This value was over the tolerable upper intake level (UL) for 1–2-year-old children, 600 µg RAE [29]. However, the primary source of vitamin A for South Koreans is a plant-based food, such as carrots and spinach [29]. Pro-vitamin A carotenoids in plant-based food are found in dark green and yellow-orange vegetables and fruits, such as carrots and spinach, which may cause yellowish coloration of the skin but have no harm [42]. Therefore, the reference value above the UL would not be a matter of concern.
The reference value of vitamin C per day for the entire population was calculated to be 95 mg based on KDRIs. In KDRIs, the estimated average requirement (EAR) of vitamin C was set considering the antioxidant activity level [29] as in the Japanese standards [1425]. In the WHO and UNHCR standards, the recommended daily amounts of vitamin C were set at 28 mg to prevent scurvy [5644].
In this study, the reference values of B vitamins per day were calculated based on the RNI for adult males and females per day [29]. In the WHO and UNHCR standards, the thiamin, riboflavin, and niacin requirements were proportional to energy intake and were calculated as follows: 0.4 mg per 1,000 kcal for thiamin, 0.6 mg per 1,000 kcal for riboflavin, and 6.6 mg NE per 1,000 kcal for niacin [5645]. In the Japanese standards [14], the nutrient requirements of B vitamins were calculated based on RDA calculated by EAR [25]. EARs of B vitamins for adults were proportional to energy intake and were calculated as follows: 0.45 mg per 1,000 kcal for thiamin, 0.5 mg per 1,000 kcal for riboflavin, and 4.8 mg NE per 1,000 kcal for niacin [1425].
In this study, the reference value of folic acid for the entire population was calculated to be 350 µg DFE based on KDRIs. In KDRIs, EAR of folic acid for adults was set by the result of a study on the requirement of folic acid for American adults [29]. In the WHO and UNHCR standards, a minimum amount of folic acid was set to be 160 µg which is the minimum level required to prevent deficiency for 3 to 4 months if all folate intake were stopped [5642].
Regarding minerals, calcium and iron were included in this study. The WHO standards included 3 minerals: calcium, iron, and iodine; however, the UNHCR standards included iron and iodine but not calcium [56]. In contrast to the WHO and UNHCR standards, the Japanese standards did not include any minerals [14].
In this study, the iron requirement was calculated as the combination diet of nonheme iron and heme iron (12% of iron absorption) based on KDRIs [3046]. In the case of WHO, the iron requirement was calculated as high-bioavailability diets (22%) for industrialized countries[547]. In the case of UNHCR, the iron requirement was calculated as low-bioavailability diets (7.5%) for developing countries [647].
The nutrient-based nutritional standards during disasters in this study were developed targeting healthy people who do not have chronic diseases, such as diabetes or kidney diseases. Therefore, they are inappropriate for use in medical institutions or medical welfare facilities for the elderly.
Although the nutrient-based standards were developed in this study, food-based standards can be used easily and simply according to the situations and circumstances in the field as nutritional standards. They are useful for dietitians without nutrition software or people who are non-nutrition specialists in disaster situations. Further studies developing food-based nutritional standards during disasters in South Korea are recommended. A validation study of the nutrient-based standards has not been conducted, which is a limitation of this study. A further study should be conducted to validate the feasibility of applying the standards.
In conclusion, nutrient-based nutritional standards for food service at shelters during disasters in South Korea were developed by selecting target nutrients and calculating their reference values. The nutrient-based nutritional standards developed in this study could be used to provide meals for evacuees of temporary residential facilities or to select and combine nutritious relief food during disasters to help maintain the health of disaster evacuees in South Korea. In addition, the procedure and methodology of this study could provide valuable information for other countries when developing nutrient-based nutritional standards during disasters.
 XML Download
XML Download