

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cigarette smoking is the leading cause of preventable death worldwide, killing more than 8.7 million people each year and about 10% of deaths related to cardiovascular disease (CVD) are attributed to smoking.1)2) The most effective method of reducing the risk of CVD caused by smoking is to quit smoking.3) Smoking cessation before 35–44 years prevents most of the risk of dying from a smoking-related disease, although smoking cessation at any age is beneficial.4) Public health strategies that specifically target adults aged 45 years and older are implemented to increase quit attempts; however, smokers younger than 45 years of age are less likely than older smokers to be advised to quit.3) Furthermore, long-term follow-up studies conducted on young adults are insufficient. Since the incidence and mortality of CVD among young adults below 40 years are relatively low, a big data study analysis is required to confirm this relationship.
Potential risk modifiers for CVD among lifestyle habits include smoking, lack of physical activity, obesity, and mental illness related to depression or stress.5)6) These risk factors tend to cluster, and many of them increase the risk of hypertension, diabetes mellitus, hypercholesterolemia, metabolic syndrome, and CVD.7)8)9) Approximately 70% of all individuals at risk have multiple risk factors that interact synergistically to increase the total risk.10) In particular, the management of risk factors in young adults have great health implications because these risk factors become habits over time, especially those with an early age onset. Therefore, it is important to understand the prevalence of risk factors and the effect of each factor on CVD in young adults. It is also of public health significance to present the effect of each combination of risk factors that tend to be clustered on CVD.
This study aimed to: 1) investigate the impact of smoking continuation, cessation, and late-onset smoking on early-onset CVD in young adults; 2) present the prevalence of potential risk modifiers such as cigarette smoking, obesity, and depression and their individual effects on CVD; and 3) confirm the clustering effect of each combination of obesity and depression using the Korean National Health Insurance Services (NHIS) data.
METHODS
Ethical statement
This study was approved by the Institutional Review Board of the Seoul National University Hospital (IRB No. E-2111-116-1273). The review board waived the requirement for written informed consent from patients because the data are public and anonymized under confidentiality guidelines.
Data source and study setting
The Korean NHIS is a mandatory universal health insurance system managed by the Korean government and recommends that all citizens aged ≥40 years and all employees, regardless of age, undergo a national health examination at least biennially. The health examination included: 1) past medical history and current medications; 2) lifestyle habits such as cigarette smoking, alcohol consumption, and physical activity; 3) anthropometric measurements; and 4) laboratory tests. The data of individuals from the health examinations were deposited in the Korean NHIS database and used for epidemiological studies.
Study population
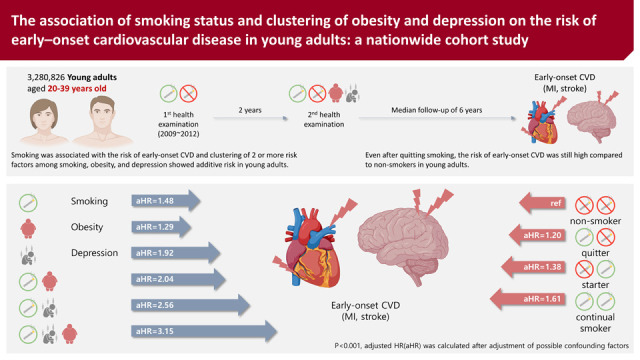
Using the Korean NHIS data, we collected participants aged 20–39 years old who had undergone their first health examination between 2009 and 2012 (n=6,891,399). We included participants who had undergone a second health examination 2 years after the first health examination to determine changes in smoking status (n=3,694,708). Patients with missing information (n=387,440) were excluded. Participants diagnosed with myocardial infarction (MI) (n=15,703) or stroke (n=8,845) before the second health examination were also excluded. To reduce the effect of reverse causality, a 1-year lag time was applied by excluding participants diagnosed with CVD (n=845) or who died (n=1,049) within 1 year of the second health examination. In total, 3,280,826 participants were included in the analysis (Supplementary Figures 1 and 2).
Definition of smoking status and smoking behaviors
Current cigarette smokers were defined as those who smoked at least 100 cigarettes in their lifetime and smoked every day or on some days at the time of the second survey. Based on the changes in the smoking status from the first and second health examinations, the participants were divided into four groups as follows: non-smokers (no/no), quitters (yes/no), starters (no/yes), and continual smokers (yes/yes). The current smokers consisted of starters and continual smokers, and the non-current smokers consisted of non-smokers and quitters.
Smoking intensity was defined as the number of cigarettes smoked per day and categorized as light smokers (<10 cigarettes/day), moderate smokers (10–19 cigarettes/day), and heavy smokers (≥20 cigarettes/day). The age of initial cigarette smoking was calculated as current age minus the number of years of smoking. The pack-years of cigarette smoking were calculated by multiplying the number of cigarettes smoked per day by the number of years of smoking.
Other potential risk modifiers of cardiovascular disease
Body mass index (BMI) was calculated as weight (kg) divided by height in meters squared (m2), and BMI over 25 was considered obese according to the Asia-Pacific obesity guidelines.11) The presence of depression was defined by medical claims data before screening based on the International Classification of Diseases, 10th Edition (ICD-10) codes (F32 depressive episode or F33 recurrent major depressive disorder) and relevant prescriptions of at least one claim per year. Heavy alcohol consumption was defined as the consumption of more than 30 g of alcohol per day.12) Regular physical activity was defined as high-intensity physical activity for 3 days per week or moderate-intensity physical activity for 5 days per week.13)
Covariates
Information on covariates was based on the answers provided to the questionnaire from the second health examination. Demographic characteristics, including sex, age, residence, and household income, were collected. The presence of hypertension, diabetes mellitus, or hypercholesterolemia was defined by medical claims data before screening based on the ICD-10 codes and relevant prescriptions of at least one claim per year: 1) hypertension (I10–I13 or I15 and antihypertensive medication or blood pressure ≥140/90 mmHg), 2) diabetes mellitus (E11–E14 and antidiabetic medication or fasting glucose level ≥126 mg/dL), and 3) hypercholesterolemia (E78 and lipid-lowering medications or total cholesterol level ≥240 mg/dL).14) Chronic kidney disease was defined based on the glomerular filtration rate of <60 mL/min/1.73 m2 as estimated by the Modification of Diet in the Renal Disease equation.15)
Study outcomes and follow-up
The study end points were incident CVD (MI and ischemic stroke). MI was defined by ICD-10 codes (I21–I22) during hospitalization. Ischemic stroke was defined by ICD-10 codes (I63–I64) for diagnoses made during hospitalization plus claims for brain imaging tests including magnetic resonance imaging and computerized tomography. The study population was followed-up till the date of MI or ischemic stroke or the end of follow-up period (31 December 2018), whichever was earlier.
Statistical analysis
Continuous variables were compared using Student’s t-test or Mann-Whitney U test and were presented as mean±standard deviation or median with the interquartile range. Categorical variables were compared using the χ2 test and were presented as numbers and percentages. The risk of CVD incidence was expressed as hazard ratio (HR) and 95% confidence interval (CI) using a Cox proportional hazard regression model adjusted for age, sex, current smoking, BMI, depression, drink, regular physical activity, income, hypertension, diabetes mellitus, hypercholesterolemia, and chronic kidney disease. The proportional hazards assumption was verified using Schoenfeld residuals. The chronological trend for the probability of CVD, MI, or stroke incidence according to the status of risk factors was obtained by Kaplan-Meier analysis and compared between the groups using the log-rank test. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), and a p value <0.05 (2-sided) was considered statistically significant.
RESULTS
Characteristics of study participants and smoking behaviors in current smokers
Table 1 shows the baseline characteristics of the study population (n=3,280,826) according to changes in smoking status. The proportion of male participants was 62.9%. The mean age of participants was 32 years. The proportion of those aged <30 years was 30.4%, and that of those aged 30 to 39 years was 69.6%. The proportion of non-smokers, quitters, starters, and continual smokers was 60.9%, 5.6%, 4.0%, and 29.5%, respectively.
Table 1
Baseline characteristics of study population according to smoking habit changes
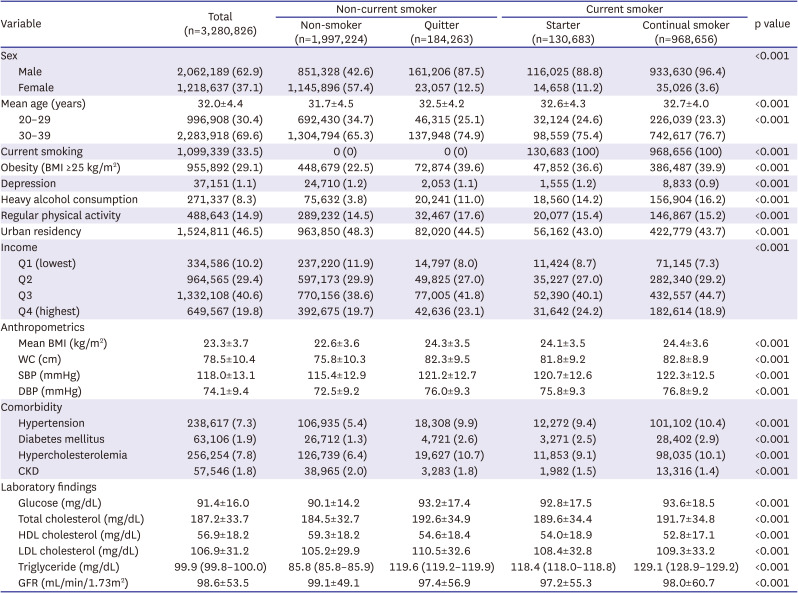
Continuous variables were compared using Student’s t-test or Mann-Whitney U test and were presented as mean ± standard deviation or median (interquartile range). Categorical variables were compared using the χ2 test and were presented as number (%).
BMI = body mass index; CKD = chronic kidney disease; DBP = diastolic blood pressure; GFR = glomerular filtration rate; HDL = high-density lipoprotein; LDL = low-density lipoprotein; SBP = systolic blood pressure; WC = waist circumference.
The proportion of current smokers was 33.5% and that of female smokers was 4.5%. Mean age at cigarette smoking initiation was 20.5 years, and it was significantly lower in continuous smokers than in starters (20.2 vs. 22.3 years, p<0.001). The proportion of smokers who commenced cigarette smoking before 15 years was significantly higher in continuous smokers than in starters (7.2% vs. 4.5%, p<0.001). The mean number of cigarettes smoked per day was 13.9 cigarettes/day for current smokers, and it was significantly higher in continuous smokers than in starters (14.2 vs. 11.3 cigarettes/day, p<0.001). The proportion of heavy smokers was significantly higher among continuous smokers than among starters (33.1% vs. 20.7%, p<0.001). The proportion of smokers who smoked > 10 pack-years was significantly higher in continuous smokers than in starters (41.6% vs. 24.8%, p<0.001) (Supplementary Table 1).
Association between smoking and the risk of cardiovascular disease, myocardial infarction, or stroke
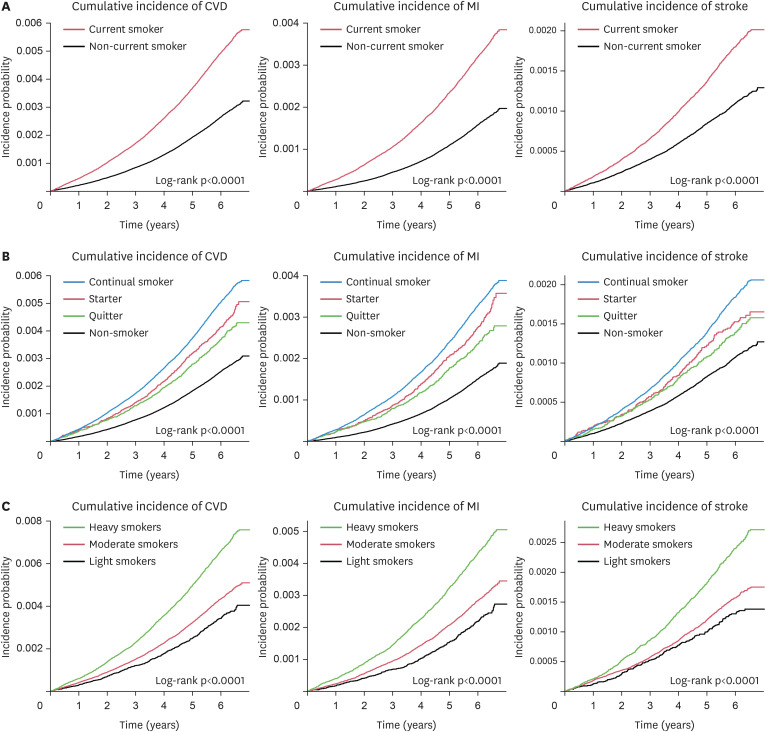
During a median follow-up of 6 years, there were 9,780 early-onset CVD events (mean age 33.8±4.1 years; male 77.0%). The baseline characteristics of the study population according to the CVD outcomes are shown in Supplementary Table 2. There were 4,828 CVD, 3,143 MI, and 1,765 stroke events among current smokers. The cumulative event rates for CVD, MI, and stroke were significantly higher in current smokers than in non-current smokers in the Kaplan-Meier curve (log-rank p<0.001 in Figure 1A).
Figure 1
Cumulative incidence of CVD, MI, and stroke according to the smoking status (A), change in smoking status (B), and smoking intensity (C).
CVD = cardiovascular disease; MI = myocardial infarction.
Multivariable analysis showed that current smokers had a significantly higher risk of CVD (adjusted HR [aHR], 1.53; 95% CI, 1.46–1.60; p<0.001), MI (aHR, 1.66; 95% CI, 1.57–1.76; p<0.001), and stroke (aHR, 1.35; 95% CI, 1.26–1.45; p<0.001) than non-current smokers after adjustment for possible confounders (Table 2).
Table 2
Association between smoking habit changes and risk of CVD, MI, or stroke
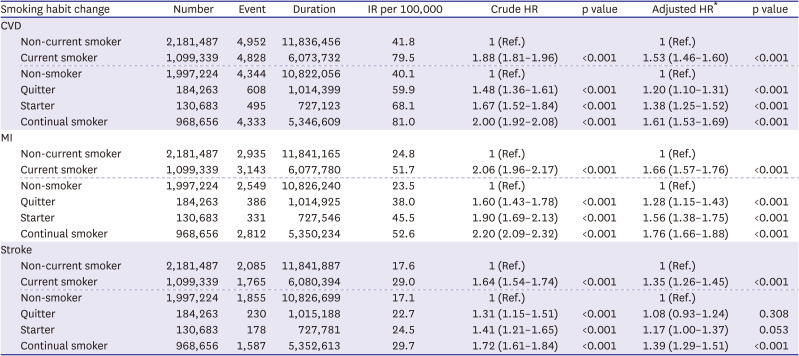
HR and 95% CI using a Cox proportional hazard regression model.
CI = confidence interval; CVD = cardiovascular disease; HR = hazard ratio; IR = incidence rate; MI = myocardial infarction.
*Adjusted HRs have been adjusted for age, sex, body mass index, depression, drink, regular physical activity, income, hypertension, diabetes mellitus, hypercholesterolemia, and chronic kidney disease.
Association between smoking habit changes in smoking status and the risk of cardiovascular disease, myocardial infarction, or stroke
The cumulative risks for CVD, MI, and stroke events were highest in continuous smokers, followed by starters, quitters, and non-smokers (Figure 1B). Smoking was more strongly associated with CVD in patients with MI than in those with stroke. Multivariable analysis showed that continuous smokers had a significantly higher risk of CVD (aHR, 1.61; 95% CI, 1.53–1.69; p<0.001), MI (aHR, 1.76; 95% CI, 1.66–1.88; p<0.001), and stroke (aHR, 1.39; 95% CI, 1.29–1.51; p<0.001) than non-smokers. Smoking starters had a significantly higher risk of CVD (aHR, 1.38; 95% CI, 1.25–1.52; p<0.001), MI (aHR, 1.56; 95% CI, 1.38–1.75; p<0.001), and higher HRs than quitters. Even after quitting smoking, the risks of CVD (aHR, 1.20; 95% CI, 1.10–1.31; p<0.001) and MI (aHR, 1.28; 95% CI, 1.15–1.43; p<0.001) were still higher in quitters than in non-smokers. The results of sex-stratified analysis are shown that the risk of MI (aHR, 1.27; 95% CI, 1.13–1.42; p<0.001) among males were higher in quitters than in non-smokers. However, the risk of MI (aHR, 1.30; 95% CI, 0.91–1.88; p=0.152) among females were not significantly different between quitters and non-smokers. Otherwise, similar results are shown between male and female (Supplementary Table 3).
Unlike continuous smokers, the risk of stroke did not significantly increase in smoking quitters (p=0.308) and starters (p=0.053) (Table 2).
Association between smoking behaviors and the risk of cardiovascular disease, myocardial infarction, or stroke
Multivariate analysis after adjustment for possible confounders showed that light smokers (aHR, 1.21; 95% CI, 1.10–1.33), moderate smokers (aHR, 1.41; 95% CI, 1.33–1.49), and heavy smokers (aHR, 1.86; 95% CI, 1.76–1.97) had a gradually increased risk of CVD in accordance with the degree of smoking intensity than non-current smokers (p for trend<0.001) The risks of MI and stroke followed the similar pattern with stepwise increased risks according to smoking intensity (all p for trend<0.001). The impact on the risk of MI was greater than that of stroke. (Supplementary Table 4). The cumulative risks for CVD, MI, and stroke events were highest in heavy smokers, followed by moderate smokers and light smokers (Figure 1C).
Multivariate analysis after adjustment for possible confounders, including the number of cigarettes smoked per day, showed that those who initiated smoking between the ages of 16 and 18 years (aHR, 1.08; 95% CI, 1.01–1.16) and those who initiated smoking before the age of 15 years (aHR, 1.16; 95% CI, 1.03–1.32) had a significantly higher risk of CVD than those who initiated smoking after the age of 19 years (p for trend=0.011) (Supplementary Table 5).
Association between smoking and potential risk modifiers and the risk of cardiovascular disease, myocardial infarction, or stroke
To evaluate the association between CVD and potential risk modifiers of CVD, univariate and multivariate Cox analyses for CVD development are shown in Table 3. Multivariable analysis showed that smoking, obesity, and depression were significantly associated with CVD incidence. However, heavy alcohol consumption and exercise showed modest associations with risk of CVD. Obese participants had a significantly higher risk of CVD (aHR, 1.33; 95% CI, 1.27–1.39; p<0.001), MI (aHR, 1.35; 95% CI, 1.27–1.42; p<0.001), and stroke (aHR, 1.31; 95% CI, 1.22–1.40; p<0.001). Participants with depression had a significantly higher risk of CVD (aHR, 1.71; 95% CI, 1.48–1.98; p<0.001), MI (aHR, 1.89; 95% CI, 1.58–2.25; p<0.001), and stroke (aHR, 1.50; 95% CI, 1.18–1.92; p=0.001) (Supplementary Table 6).
Table 3
Univariable and multivariable Cox analysis for developing cardiovascular disease in the entire study population
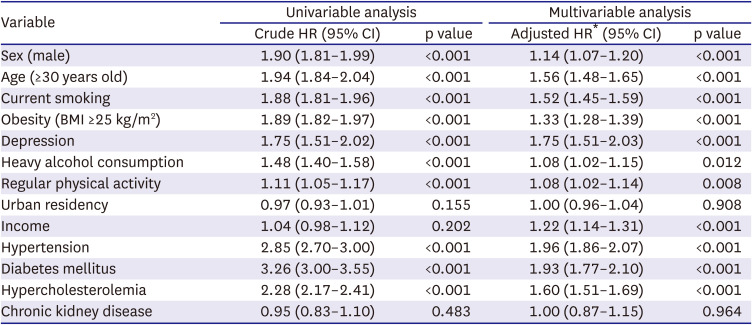
HR and 95% CI using a Cox proportional hazard regression model.
BMI = body mass index; CI = confidence interval; HR = hazard ratio.
*Adjusted HRs have been adjusted for age, sex, current smoking, BMI, depression, drink, regular physical activity, urban residency, income, hypertension, diabetes mellitus, hypercholesterolemia, and chronic kidney disease.
Association between clustering of smoking, obesity, and depression and the risk of cardiovascular disease, myocardial infarction, or stroke
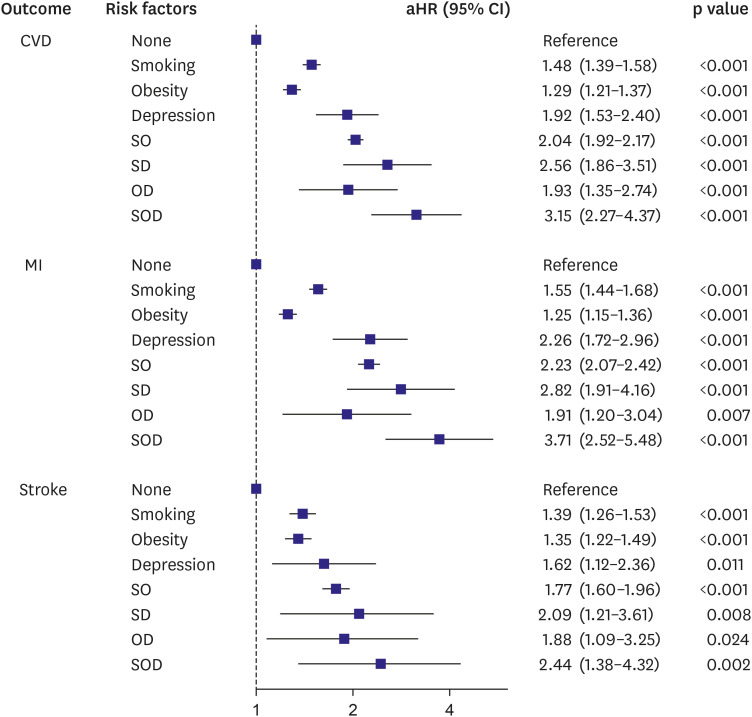
Smoking (aHR, 1.48; 95% CI, 1.39–1.58; p<0.001), obesity (aHR, 1.29; 95% CI, 1.21–1.37; p<0.001), and depression (aHR, 1.92; 95% CI, 1.53–2.40; p<0.001) had an increased risk of CVD incidence. Clusters of two or more risk factors were associated with a higher risk of CVD (aHR, 2.04; 95% CI, 1.92–2.17; p<0.001 for smoking and obesity; aHR, 2.56; 95% CI, 1.86–3.51; p<0.001 for smoking and depression; aHR, 1.93; 95% CI, 1.35–2.74; p<0.001 for obesity and depression; aHR, 3.15; 95% CI, 2.27–4.37; p<0.001 for smoking, obesity, and depression). Clusters of 2 or more risk factors were also associated with a higher risk of MI and stroke (Figure 2, Supplementary Table 7).
Figure 2
HRs and 95% CIs of CVD, MI, and stroke by clustering of smoking, obesity, and depression. aHRs have been adjusted for age, sex, current smoking, body mass index, depression, drink, regular physical activity, income, hypertension, diabetes mellitus, hypercholesterolemia, and chronic kidney disease.
aHR = adjusted hazard ratio; CI = confidence interval; CVD = cardiovascular disease; MI = myocardial infarction; OD = obesity and depression; SD = smoking and depression; SO = smoking and obesity; SOD = smoking, obesity, and depression.
DISCUSSION
In this large, population-based, nationwide study, we showed that current smoking, early age of smoking initiation, and smoking intensity in young adults aged 20–39 years are associated with an increased risk of early-onset CVD (<50 years). Smoking, obesity, and depression were independently associated with an increased risk of CVD, and clustering of 2 or more of risk factors was associated with an additive risk of CVD in young adults.
CVD that develops at a young age carries a poor long-term prognosis. The burden of CVD in young adults is important for public health, with a negative impact on physical, social, and financial aspects. In Korea, the incidence rate of hospitalised acute MI in the past 10 years (from 2007 to 2016) remained relatively constant in young adults aged <50 years, in contrast to the decreasing trend in older adults aged >50 years.16)
Cigarette smoking is more common in younger adults than older adults.17) Cigarette smoking contributes to CVD in numerous ways, including the promotion of inflammation and atherosclerosis. Atherosclerosis begins in early adulthood, with symptoms occurring later in life.18) Our results showed that current smoking status, early age at smoking initiation, and smoking intensity in young adults were associated with an increased risk of CVD. A study in the United States showed that the risk and burden of heart disease mortality were 2- to 4-fold higher in current smokers than in never smokers among young adults aged 18–44 years.19)
Earlier onset of smoking initiation is associated with higher nicotine dependence and lower abstinence rates.20) A recent Korean study with a 23-year follow-up reported that the risk of CVD among young adult men aged 20–29 years increased linearly with a higher number of cigarettes consumed per day and a longer duration of smoking.21) Another study in Australia reported that heavy smoking increases the risk of CVD mortality almost five-fold, even though light smoking almost doubles the risk of CVD mortality.22)
Smoking cessation reduces the risk of morbidity and mortality related to CVD as the number of years since smoking cessation increases.3) Even after quitting smoking in young adults, our results showed that the risk of CVD and MI was still high compared to that in non-smokers during a median follow-up of 6 years. Our findings suggest that aggressive education regarding the harmfulness of smoking and the need for smoking cessation should be provided as soon as possible to young adults. In addition, not starting smoking at all is more important than quitting after smoking since the risk of CVD and MI remains high for a long period, regardless of how quickly they quit smoking compared to non-smokers.
Cigarette smoking and other potential risk modifiers of CVD, including lack of exercise, heavy alcohol consumption, obesity, and mental illness related to depression or stress, are associated with an increased risk of CVD in young adults, and these risk factors for CVD tend to cluster.5)6)7)8)9) Our results showed that cigarette smoking, obesity, and depression were independently associated with a 1.3–1.7 times increased risk of CVD, and clustering of 2 or more of these risk factors was associated with a 2–3 times higher risk of CVD in young adults.
Obese people experience CVD events at an earlier age, live with CVD for a greater proportion of their lifetime, and have a shorter average life span than normal-weight individuals.23) Obesity accelerates atherosclerotic changes through insulin resistance and inflammation. A recent study presented at the ESC Congress 2021 reported that the occurrence of acute MI at 45 years or below was more likely to be in smokers and the obese with hypertension or diabetes mellitus.24)
Our results showed that current smokers with depression had a higher risk for CVD than those without depression. According to the 20-year trends in health behaviors and chronic diseases using data from the Korean National Health and Nutritional Examination Survey (KNHANES), the prevalence of current smoking was higher in people with high stress (44.4% in male smokers with high stress vs. 33.8% in male smokers with low stress; 7.7% in female smokers with high stress vs. 4.2% in female smokers with low stress).25) Mental illness is associated with alterations in myocardial blood flow, and chronic exposure to stress is associated with alterations in the inflammatory signalling pathways. Smokers with co-occurring mental illnesses or substance use disorders have higher levels of nicotine dependence, longer durations of smoking, and limited access to cessation treatment than the general population.26)27) In the Coronary Artery Risk Development in Young Adults (CARDIA) study, cumulative smoking exposure and cumulative depressive symptoms had a synergistic association with subclinical heart disease.28)
The strength of this study is large, population-based study aimed to investigate the association between potential risk modifiers of CVD such as smoking, obesity, and depression and the risk of early-onset CVD in young adults aged 20–39 years. In addition, the analyses performed after adjusting for multiple potential confounders. However, due to the nature of this study, several limitations should be considered when interpreting the results. First, smoking starters defined operationally in this study may include people who start smoking for the first time and those who repeat re-smoking after quitting between the first and second health examination. Second, the proportion of female smokers was very low (n=49,684, 4.5% of the total study population). The reported smoking rate in Korean women has been very low due to cultural reasons, and it is possible that the smoking rate of female smokers is underestimated when considering the high discrepancy between self-reported and actual smoking status.29) Third, despite the significant effect of second-hand smoke on CVD events, we could not reflect this information because we lacked information. Fourth, the follow-up duration was relatively short (median follow-up of 6 years), and changes in smoking behavior between the first and second health examinations or changes in smoking behavior after the second health examination were not considered. Fourth, data on the study end points, that is, MI or stroke, were obtained only from administrative data, which can be misleading. However, the accuracy of NHIS claims data for the diagnosis of MI and stroke has been previously validated.30) Finally, misclassification of bias and underreporting could have existed because smoking, obesity, and depression were based on self-reported questionnaires.
In conclusion, cigarette smoking was associated with the risk of early-onset CVD, and the clustering of two or more risk factors, including smoking, obesity, and depression, showed an additive risk of CVD in young adults. Even after quitting smoking, the risk of CVD and MI in young adults was still high compared to that in non-smokers. We suggest aggressive education in young adults on the harmful effects of smoking, not trying to start smoking in the first place, and the need to quit smoking early. Additionally, support for tailored lifestyle modification and therapeutic interventions, such as treatment for smoking cessation, lowering body weight, and management of depression, could have a great impact on reducing the risk of CVD.
 XML Download
XML Download