

 PDF
PDF Citation
Citation Print
Print



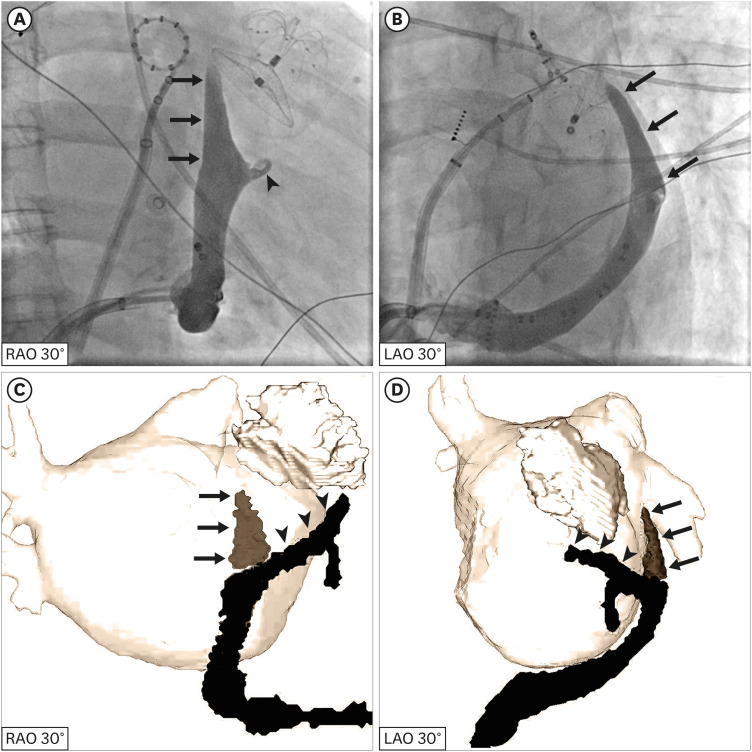
A 58-year-old woman with persistent atrial fibrillation (AF) was admitted for percutaneous left atrial appendage (LAA) occlusion, ethanol ablation of the vein of Marshall (VOM), and conventional AF catheter ablation. After LAA occlusion, a cardiac vein angiography revealed a giant VOM (Figure 1A and B). It was confirmed by the occluder in the LAA and the circular mapping catheter in the left superior pulmonary vein (Figure 1A and B). It was much larger than the great cardiac vein as shown in the right anterior oblique projection (Figure 1A). Its ostium was 13 mm × 10 mm (right anterior oblique projection × left anterior oblique projection), and the coronary sinus ostium was 12 mm × 14 mm. Finally, ethanol infusion was not performed because there were no appropriate balloons, and catheter ablation was successful. A 3-dimensional cardiac computerized tomography (CT) also showed the VOM (Figure 1C and D). The cardiac vein angiography and the cardiac CT both indicated that the large VOM was not a persistent left superior caval vein (Supplementary Videos 1, 2, 3). Additional cardiac vein angiography and three-dimensional cardiac CT figures are also provided (Supplementary Figures 1 and 2).
The VOM, also known as the oblique left atrial vein, is thought to be obliterated in most individuals. It is extremely narrow even when a lumen is present. However, it has been implicated in the pathogenesis and maintenance of AF.1) Ethanol infusion in the VOM in addition to conventional catheter ablation has been proven to increase the chances of maintaining a normal rhythm in patients with AF.2) A giant VOM is uncommon and may be found accidentally on cardiac vein angiography during ethanol ablation for AF.
This study was performed in accordance with the Declaration of Helsinki (2013) and was approved by the Ethics Committee of Fuwai Hospital (Approval Number: 2021-1575) on 06 December 2021. A written informed consent was obtained from the patient.

 XML Download
XML Download