

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Parkinson’s disease (PD) is one of the most common neurodegenerative diseases worldwide. Deep brain stimulation (DBS) is an effective procedure for improving motor function in patients with PD.12 Long-term outcomes of DBS, with a focus on mortality, have been reported in previous studies from various countries.34567
Several studies have also reported the risk factors for mortality in PD patients undergoing DBS. Regarding sex-related differences, Bang Henriksen et al.6 reported that men had a 9-fold higher mortality rate than women when comparing survivors with those who died after DBS. Ryu et al.7 also reported that the mortality rate after DBS was three times higher in men than in women. Ngoga et al.8 reported that the mortality rate in women was significantly higher than that in men in both the DBS and medication groups. However, some previous reports found no significant sex-related differences.3459 Concerning age, previous papers reported that the age at the time of surgery was higher in those who died than in those who did not.45910 However, only one previous study dealt with socioeconomic status (SES) in PD patients with DBS.11 Furthermore, there is only one report of mortality according to comorbidity in patients with DBS12; Merola et al.12 divided PD into normal cognitive and mild cognitive impairment (MCI) groups and investigated the mortality after DBS, and a slightly higher mortality rate was reported in the MCI group.
Previous studies were performed at a single center or in a subset of regions, with a small sample size, or in a subset of the population but not in a representative population. Therefore, we used a large nationwide cohort in Korea to investigate 1) the long-term outcomes of DBS, such as mortality after DBS and the causes of death, 2) demographic and socioeconomic factors influencing mortality, and 3) comorbidities affecting mortality after DBS in patients with PD.
METHODS
Data source
This study used the National Health Insurance Service (NHIS)-National Health Information Database (NHIS-2022-1-102). South Korea operates a single national health insurance system for all citizens, and in 2022, health insurance and medical aid were provided to 51,396,000 and 1,513,000 people, respectively.13 The NHIS collects usage information from medical institutions and diagnosis code prescription records according to the International Classification of Diseases (ICD), 10th Revision. Since 2002, the NHIS has made all insurance data publicly available through the health insurance data-sharing service. In addition, the Korean government operates a special registration system for rare diseases and severe intractable diseases, and the out-of-pocket rate was reduced to 10% for these diseases. PD is subject to the special registration system, and eligibility for this system is determined by an NHIS review of the doctor’s diagnosis according to the diagnostic criteria distributed by the NHIS.
Cause of death
Data on the causes of death were obtained by linking the NHIS data with the micro data integration service of Statistics Korea. The causes of death were classified based on the 8th Korean Standard Classification of Diseases (2020).14 Specific deaths, such as suicide, could not be classified because related data were not provided.
Study population
This study was conducted using NHIS data for 12 years (2005 to 2017), and all claims data, except for non-covered treatment performed in Korea during this period, were considered. PD was defined as a case in which the ICD-10 code (G20) and special registration code (V124) coexisted; this definition was used in previous epidemiologic studies of PD in Korea.1516 The incident date (index date) was defined as the date when G20 or V124 was first entered. DBS was first performed for patients with PD in Korea in 2000, and medical insurance benefits have been applied from the NHIS since 2005. Subjects with treatment codes S4738 and S0471 were selected as DBS-treated subjects among the PD patients (subjects with G20 and V124).
Demographics and SES
Age at the time of PD diagnosis and DBS was classified into four groups: < 50, 50–59, 60–69, and ≥ 70 years. Data on SES were obtained for residence, income, and health insurance qualifications. Residents were divided into Seoul, metropolitan area, and rural area.17 If the residence was located in Seoul in terms of the administrative district, it was defined as Seoul. In Korea, patients living in six metropolitan cities with a total population of ≥ 1 million, including Busan, Incheon, Daejeon, Daegu, Gwangju, and Ulsan, were classified as living in “metropolitan areas.” Patients living outside Seoul and the metropolitan areas were classified as living in “rural areas.”
Since Korea’s monthly insurance premium is determined by income level, it can be used as a proxy for SES. Income status was classified by insurance premium (lowest group: 0–20th percentile of NHI enrollees + all medical aid enrollees, lower-middle group: 21st–50th percentile of NHI enrollees, upper-middle group: 51st–80th percentile of NHI enrollees, highest group: ≥ 81st percentile of NHI enrollees). The medical insurance system in Korea is divided into health insurance and medical aid, and the medical aid system is defined as a public assistance-type medical insurance system in which the nation assists with the medical problems of low-income people.18
Comorbidity
For comorbidities, the Charlson comorbidity index (CCI) was used.19 CCI scores were classified into four categories: 0, 1, 2, and ≥ 3. In addition to CCI, ICD-10 codes were used to extract data on several diseases that are prevalent in geriatric patients or that may be clinically associated with death. Comorbidities included hypertension (I10–15), diabetes (E11–14), dyslipidemia (E78), depression (F32–34), pneumonia (J12–18), and osteoporosis (M800, M808–810, and M818–819). PD dementia (F023) and fractures were limited to those that developed after DBS in the present study. Fractures included femoral fractures (S720–722) and vertebral fractures (S120–122, S220–221, S320, M485).
Statistical analysis
Descriptive analysis of the DBS group was performed. Demographic characteristics are presented as mean values ± standard deviation or as numbers (%) when applicable. The Kaplan-Meier method was used for survival analysis, and the log-rank test was used to compare survival rates and survival curves. Univariate and multivariate Cox regression analyses were used to estimate hazard ratios (HRs) and their 95% confidence intervals (CIs). Regarding PD dementia and fracture, which did not satisfy the assumption for the proportional HR, time-dependent cox analysis was used.20 First, a univariate time-dependent Cox regression model was implemented, and a multivariate time-dependent Cox regression model was then used after adjusting for confounding variables including sex, age at diagnosis, income, insurance type, CCI index, and comorbidities. The effect of PD dementia and fracture on survival was tested using the Mantel-Byar method with a time-dependent covariate for comparison of survival data to adjust for immortal time bias.20 SPSS version 20 (IBM Corp., Armonk, NY, USA) and R ver. 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria) were used for all statistical analyses, and a P value < 0.05 was considered significant.
RESULTS
Baseline clinical characteristics
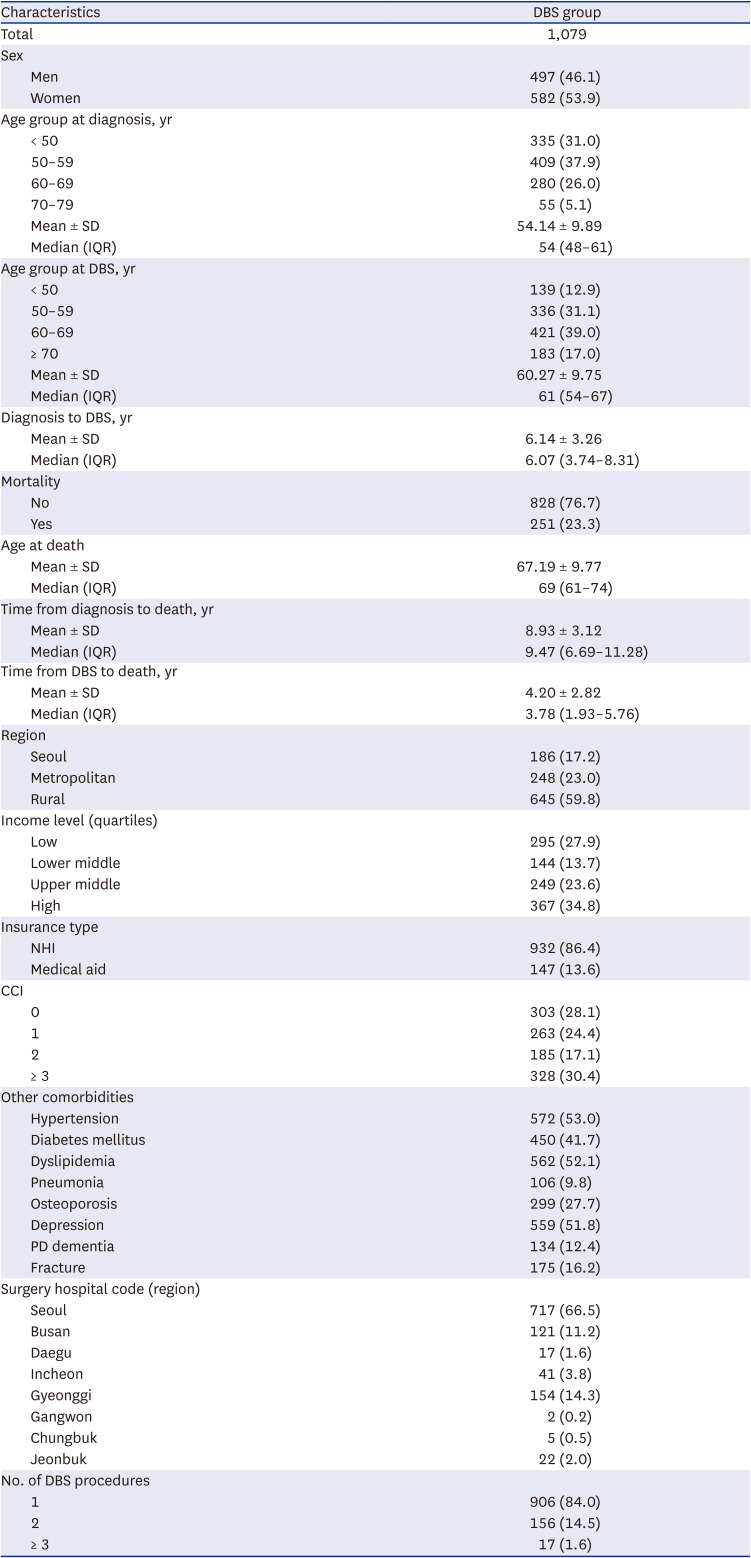
Table 1 shows the demographic and baseline clinical characteristics of the PD patients who underwent DBS surgery (Table 1). Of the 1,079 patients, 582 (53.9%) were female (Table 1). The mean age at diagnosis was 54.14 ± 9.89 years, and the mean age at surgery was 60.27 ± 9.75 years, and the mean time from diagnosis to surgery was 6.14 ± 3.26 years. Regarding the age distribution at diagnosis, 335 people (31.0%) were under 50 years, 409 people were in their 50s (37.9%), 280 people were in their 60s (26.0%), and 55 people were in their 70s and above (5.1%). Regarding the age distribution at DBS, 139 patients were under 50 (12.9%), 336 were in their 50s (31.1%), 421 were in their 60s (39.0%), and 183 (17.0%) were over 70 years old. Regarding SES, 17.2% lived in Seoul, 23.0% in metropolitan areas, and 59.8% in rural areas. The low, lower middle, upper middle, and high income groups accounted for 27.9%, 13.7%, 23.6%, and 34.8%, respectively. Regarding insurance coverage, health insurance accounted for 86.4% and medical aid accounted for 13.6%. Among comorbid diseases, 28.1% had a CCI index of 0, while 24.4%, 17.1%, and 30.4% had CCI indices of 1, 2, and ≥ 3, respectively. Hypertension was found in 53.0%, diabetes mellitus in 41.7%, dyslipidemia in 52.1%, pneumonia in 9.8%, osteoporosis in 27.7%, depression in 51.8%, PD dementia in 12.4%, and fracture in 16.2%. Concerning the regions where DBS was performed, Seoul had the most (66.5%), followed by Gyeonggi-do (14.3%), Busan (11.2%), and Incheon (3.8%). Regarding the number of times DBS was performed, 84.0% underwent DBS once, 14.5% two times, and 1.6% three or more times.
Table 1
Demographics and clinical characteristics of patients with Parkinson’s disease who underwent DBS
Mortality and risk factors
Of 1,079 PD patients, 251 (23.3%) died, with a mean follow-up period of 10.55 ± 0.21 years after surgery. The mean age at death was 67.19 ± 9.77 years. The survival curve for all patients is shown in Fig. 1A. The results showed 1-, 3-, 5-, 10-, and 12-year survival rates of 96.9%, 90.8%, 81.1%, 59.7%, and 52.5%, respectively, for PD patients that underwent DBS (Fig. 1A).
Fig. 1
Kaplan-Meier curves. (A) Kaplan-Meier curve of the total DBS group. (B) Kaplan-Meier curve by age at diagnosis. (C) Kaplan-Meier curve by age at surgery. (D) Kaplan-Meier curve by presence of PD dementia. (E) Kaplan-Meier curve by presence of fracture.
DBS = deep brain stimulation, PD = Parkinson’s disease.
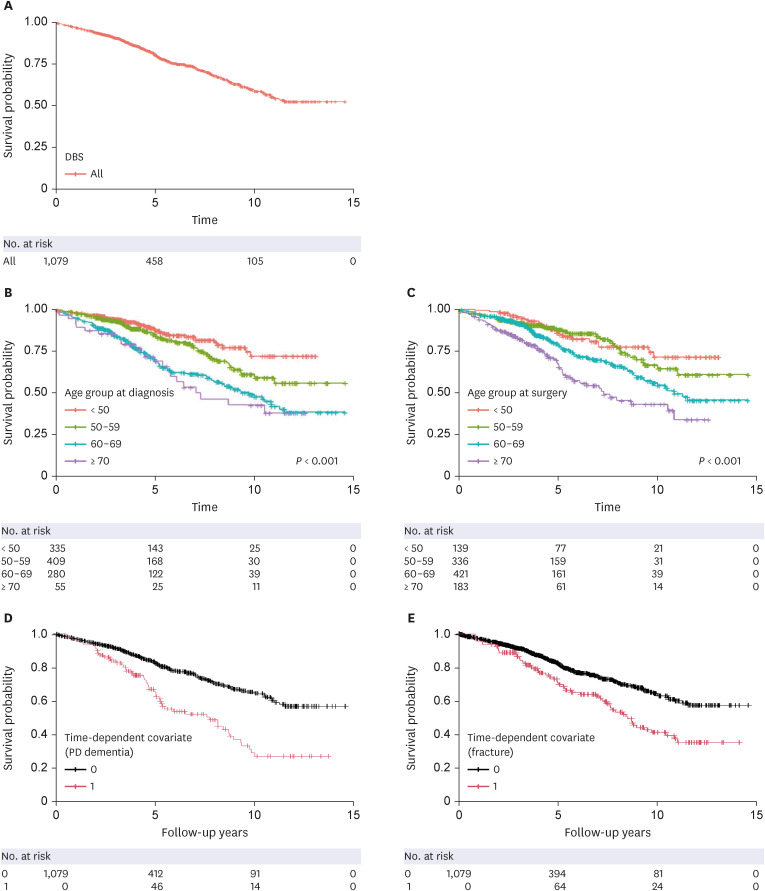
Kaplan-Meier plots illustrating survival probability with statistical significance are presented in Fig. 1B and C by age at diagnosis and age at surgery, respectively. Other Kaplan-Meier plots showed no statistical significance (figures not shown). The effects of PD dementia and fracture on survival using the Mantel-Byar method are shown in Fig. 1D and E, respectively.
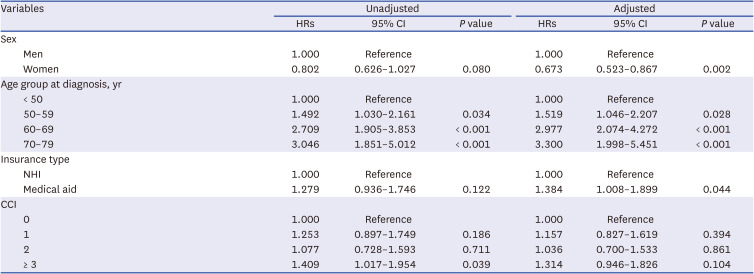
Table 2 shows unadjusted and adjusted HRs for mortality among the DBS group. After adjusting for confounding variables such as age group at diagnosis, insurance type, and CCI, Cox proportional-hazard regression model showed an HR of 0.673 (95% CI, 0.523–0.867) for mortality in women although univariate HR showed no statistical significance. Regarding the age group at diagnosis, patients in their 60s and 70s showed significantly different mortality rates compared to patients under 50 (HR, 2.977, 95% CI, 2.074–4.272; HR, 3.300, 95% CI, 1.998–5.451, respectively) in a graded manner. When age group at surgery was substituted for age group at diagnosis, patients in their 60s and 70s showed significantly different mortality rates compared to patients under 50 (HR, 2.075, 95% CI, 1.314–3.276; HR, 3.446, 95% CI, 2.120–5.600, respectively) in a dose-response relationship (not shown in Table 2). According to insurance type, the HR for mortality was 1.384 (95% CI, 1.008–1.899) in the medical aid group. When health insurance type was replaced by income level, there was no significant difference in mortality rate (not shown in Table 2). There are no significant difference in mortality rate according to CCI. In summary, being male, older age at diagnosis, older age at surgery, and the use of medical aid were associated with a higher risk of mortality (Table 2).
Table 2
Unadjusted and adjusted HRs for mortality in the deep brain stimulation group
Comorbidity
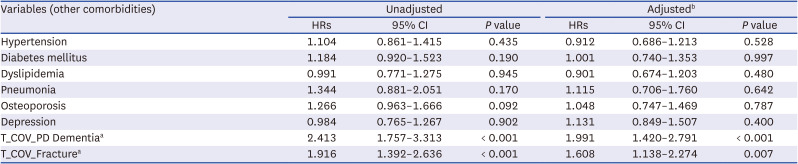
Table 3 shows unadjusted and adjusted HRs for mortality among the DBS group according to comorbidity. After adjusting for confounding variables such as demography and SES, the time-dependent Cox hazard regression model showed a HR of 1.991 (1.420–2.791) for mortality in the PD dementia group, and HR of 1.608 (1.138–2.274) for mortality in the fracture group. Other comorbidities showed no statistical significance.
Table 3
Unadjusted and adjusted HRs for mortality in the deep brain stimulation group with regard to specific comorbidities
Cause of death
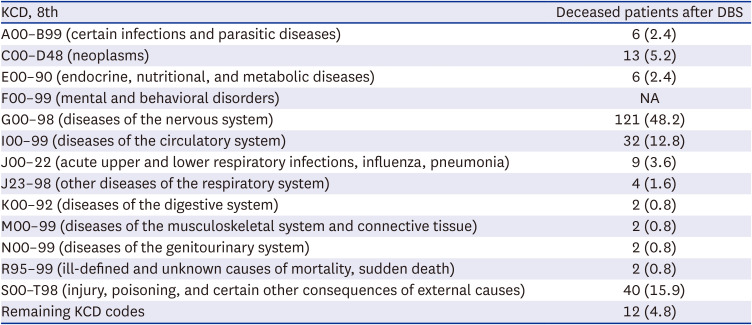
The causes of death are listed in Table 4. PD was the most common cause of death (118, 47.1%). Forty patients (15.9%) died of S00–T98 (injury, poisoning, and certain other consequences of external causes). Thirty-two patients (12.8%) died of I00–99 (diseases of the circulatory system). Thirteen patients (5.2%) died of C00–D48 (neoplasms).
Table 4
Cause of death after DBS
DISCUSSION
This study is the first to present the long-term outcomes of DBS in PD patients in a representative population in a country. We studied the national cohort with PD for a long duration (10.55 ± 0.21 years) after DBS surgery in Korea. The present study showed that 251 (23.3%) of 1,079 PD patients died, with a mean time to death of 10.55 ± 0.21 years after surgery, and that PD was the most common cause of death. The mortality rate in the present study was 23.3%. The study was compared with previous studies reporting the overall mortality of the DBS patients, which ranged from 8.2% to 34.0% in different groups and countries.569 In the present study, our cohort had a survival rate of 81.1% at 5 years, which is lower than that described in the studies by Schüpbach,3 Toft,4 and Ryu7 (89.0%, 90.0%, and 85.0% at 5 years, respectively). However, 10-year survival rates after surgery were not available in these previous studies. These results may be explained by the fact that DBS has been performed in different countries and races. Thus, it is difficult to directly compare the results because these studies were conducted on a different population with different disease durations before surgery, and the survival curve depends on when surgery is performed.
In Korea, 16.96% of DBS surgeries were performed on patients over 70 years old. The mean duration from diagnosis to surgery was 6.14 ± 3.26 years. These findings demonstrate the current situation of DBS surgery in Korea, which suggests that DBS is liberally performed.
In the present study, older age at diagnosis and older age at surgery were associated with a higher risk of mortality. These findings are compatible with those of previous studies.4591012 Being male was associated with a higher risk of mortality compared to being female in the present study. These findings are not comparable to those of previous studies, which showed conflicting results.3456789 There is no clear explanation of the mechanism for the sex-related differences; however, additional research is needed in the future.
In the present study, the use of medical aid was associated with a higher risk of mortality, whereas income level and residence were not associated with mortality. Only one previous study has investigated the influence of SES on DBS. Genc et al.11 found that PD patients with higher household incomes had better functional improvement 1 year after DBS.
After adjusting for confounding variables, the time-dependent Cox hazard regression model with the Mantel-Byar method showed HRs of 1.991 and 1.608 for mortality in the PD dementia and fracture groups, respectively, whereas other comorbidities showed no statistical significance. This finding on PD dementia is similar to that in a previous study, where a slightly higher mortality rate after DBS was reported in the MCI group compared to the normal cognition group.12 Previous studies also reported a higher mortality rate in PD patients with dementia who did not undergo surgery.2122 These studies support the results of the present study. The reasons for the increased mortality in dementia are unclear, although malnutrition, swallowing difficulty, and bedridden status, which may be due to dementia, may be involved.23
No previous research has been conducted regarding the comorbidity of fractures in PD patients with DBS. However, several previous studies have reported the comorbidity of fracture in PD patients without DBS; mortality after fracture is substantially increased among those with PD without DBS surgery.1624 As the disease progresses in PD, the risk of falls increases, and falls lead to fractures and serious dysfunction.25 Thus, the burden of comorbidities such as dementia and fracture are important prognostic factors for mortality in PD with DBS, but further study is needed.
PD was the most common cause of death (47.1%) in the present study. This finding is similar to the results of Lau et al.,26 who reported that most patients died due to PD progression. Weaver et al.27 also found that in a study comparing DBS and medication treatment groups, most people who died after DBS died from PD. Schüpbach et al.3 also reported death due to progression of PD after cancer. However, pneumonia was reported to be the most common cause of death in several previous studies.5712282930 Swallowing-related disorders in PD patients have been reported to have a high prevalence, and their severity is related to the duration and severity of PD.31 Most swallowing disorders show symptoms as PD progresses, resulting in frequent aspiration pneumonia. Therefore, it can be assumed that pneumonia was one of the most common causes of death in other studies. In the present study, pneumonia, which was selected as the main diagnosis, was reported in 3.6% of the participants, which might be originated from the intrinsic carelessness of the physicians when registering death records. Thus, PD may be possibly the main diagnosis at the time of death instead of pneumonia in the present study.
The present study had several strengths. Our study examined a large nationwide cohort that was followed for a longer period of time than in previous studies.
The present study also had some limitations. First, information on the severity of the disease was not available because of the nature of the data. Data on the Hoen-Yahr scale or Unified Parkinson’s disease rating scale, which is used to determine the severity of the disease, was not available. Second, the exact onset time of PD and the duration of the disease were not available due to the nature of the data.
In conclusion, older age at diagnosis and surgery, being male, the use of medical aid, and the comorbidity of dementia and fractures were associated with a higher risk of mortality after DBS in patients with PD. Neurologists should consider these risk factors in assessing the prognosis of PD patients undergoing DBS.
 XML Download
XML Download