

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Stigma and attitudes toward mental disorders are closely related to individuals’ help-seeking behaviors and use of mental health services.1 In contrast, physical illnesses are considered to be treatable, depending on the severity and/or patient distress, by the general population.2 Nationwide surveys on attitudes toward mental disorders have been conducted in many countries, including South Korea.345 Although 65.2% of Korean adults have experienced mental health problems during their lifetime, only 25.3% have sought any help. In addition, 18.9% of Korean adults reported having negative thoughts toward mentally ill individuals, which discouraged them from seeking mental health services.4
Due to recent developments in neuroscience, our understanding of the pathophysiological mechanisms underlying psychiatric diseases is gradually increasing. Accordingly, a biogenetic explanation of mental disorders is commonly provided in public campaigns and mental health education. For example, many anti-stigma initiatives for mental disorders, including the US National Alliance for Mental Illness,67 refer to mental disorders as medical diseases and compare major depression and schizophrenia to the common cold and diabetes, respectively.89 Similar campaigns and studies have been conducted in India10 and New Zealand.11 These biogenetic explanations attribute mental illnesses to biological factors, including genetic predisposition, neurotransmitter imbalances, and functional abnormalities in the brain network. A biogenetic approach can reduce moral and punitive responses to patients by emphasizing that mental illness is unrelated to individual will or personality.12 However, there are several concerns regarding treating mental illness as a biomedical disorder. It is argued that the biogenetic explanation leads to over-diagnosis and over-treatment of mental disorders,13 and that it increases stigma toward mental illness.
Previous studies of the effect of biogenetic explanations on attitudes toward mental illness showed inconsistent results. One study showed that ‘social distance,’ a measure of stigma toward mentally ill people, was increased after providing a biogenetic explanation,14 whereas another study showed a decrease in ‘social distance’ with the biogenetic concept of mental disorders.15 A previous study showed that ‘attitude toward help-seeking’ was increased in those with a biogenetic concept of mental illness,16 whereas another study showed the opposite result.17 Several previous meta-analyses have been conducted to integrate these inconsistent findings.181920 In these previous meta-analyses, some types of stigma, including ‘social distance,’ ‘perceived dangerousness,’ and ‘prognostic pessimism,’ were increased by neuroscientific explanations. Previous researchers suggested that a biogenetic explanation is associated with adverse effects on stigma, although the biogenetic concept is not intrinsically stigmatizing.
Designing an effective strategy for public education and/or discussion of mental health-related issues requires the consideration of several factors in addition to causal explanations. Therefore, different strategies should be used depending on the mental illness being discussed, target audience of the education, and cultural background thereof. Previous meta-analyses181920 reported that a neuroscientific explanation leads to increased stigma toward mental disorders through the promotion of neuroessentialism, and they suggested that caution should be exercised when providing scientific information related to mental disorders. However, it is unclear how the strategies for mental health education can be improved.
Mental disorders differ in terms of severity and prognosis; therefore, individuals may have different attitudes toward different mental disorders. Previous studies showed that biogenetic causal beliefs led to increased blame (a stigma measure) toward patients with schizophrenia21 and reduced blame toward patients with depression.22 In addition, stigmatization by biogenetic explanations depends on the target audience of education, and is particularly different between the general population and patients. In previous studies, a biogenetic explanation of mental illness increased ‘prognostic pessimism’ in the general population,21 and decreased it in patients.23 Finally, cultural background may affect consequences of the biogenetic approach toward mental disorders. Thoughts and attitudes toward mentally ill people are usually acquired from early life education and experiences, and the sociocultural atmosphere significantly affects this process. In general, there are higher levels of stigma and personal attributions toward mental illness in Eastern countries, while Western populations have higher discrimination against minorities compared to the majority with mental illness.24
In the present study, we evaluated the effect of a biogenetic explanation on attitudes toward mental disorders, as well as its various aspects. Based on a previous study,1819 we used four operational concepts of stigma as outcome measures, as well as an additional factor of ‘attitude toward help-seeking,’ which could influence the use of mental health services. We examined the influence of biogenetic explanations on each stigma measure, followed by subgroup analyses according to the mental disorder type (psychotic vs. neurotic vs. general mental disorders), subject characteristics (patients vs. general population), and cultural background (Western vs. Eastern populations).
METHODS
Data source and study selection
The protocol of the present meta-analysis was registered in PROSPERO (CRD42020158656) in March 2020. We searched six databases (PubMed, EMbase, Cochrane, CINHAL, Psyinfo, and Web of Science) for papers published before March 2020. MeSH terms used for the search were selected on the advice of a librarian from the Seoul National University College of Medicine, and included: 1) terms related to specific mental diseases, including ‘alcohol use disorder,’ ‘depression,’ ‘schizophrenia,’ as well as terms related to general mental conditions such as ‘mental health problems,’ ‘mental illness,’ and ‘mental disorder’; 2) terms that refer to ‘biogenetics’ as explanatory expressions (e.g., ‘biogenetic’ and ‘biological’) and causal factors (e.g., ‘brain disorder’ and ‘chemical imbalance’); and 3) five terms for outcome measures related to attitudes toward mental disorders [‘help-seeking,’ ‘blame,’ ‘dangerousness,’ ‘(prognostic) pessimism,’ and ‘social distance’]. The MeSH terms are presented in Supplementary Data 1. Two independent researchers (CH Baek and HJ Kim) screened the studies, and another researcher (JE Park) independently reviewed the screened studies. The included studies were evaluated in terms of study quality and possibility of data extraction. The Joanna Briggs Institute Critical Appraisal Checklist for analytical cross-sectional studies (last amended in 2017) was used to evaluate the risk of bias (Supplementary Table 1).
Study design
The analysis included experimental and correlational studies. Experimental studies were included if they involved an explanation of the causes of mental disorders to subjects, and comparisons of attitudes toward mental disorders before and after the explanation, or a comparison of the attitudes between experimental and control groups after providing a biological or other (e.g., social or psychological etiology) explanation, respectively. The correlational studies evaluated the relationship between beliefs regarding the causes of mental disorders and attitudes toward mental disorders. These studies did not provide an explanation of the causes of mental disorders to the participants. Tables 1 and 2 present the list of included studies.
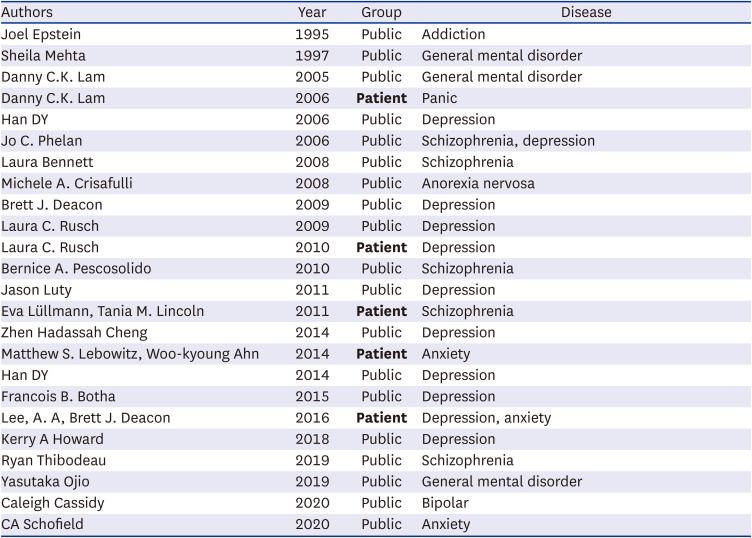
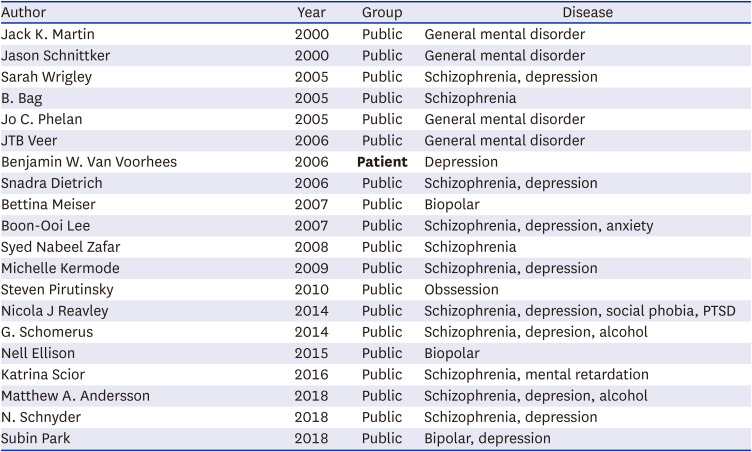
Table 1
List of experimental studies
![]()
Table 2
List of correlation studies
![]()
The attitude toward mental disorders is classified into five concepts. We followed the operational definitions of the four stigma constructs used by a previous study1819: ‘blame,’ ‘perceived dangerousness,’ ‘prognostic pessimism,’ and ‘social distance.’ Mental health stigma is a multifaceted concept, therefore, previous studies have used various measures to represent different aspects of stigma. However, for conducting meta-analysis, it is necessary to simplify and choose the core elements from various concepts. There were three prior meta-analytic studies181920 which have addressed the question similar with ours. The first meta-analysis18 has defined four elements of mental health stigma based on their comprehensive review of previous studies: blame, perceived dangerousness, prognostic pessimism, and social distance, and the following two studies have used the concepts and supplemented the results. These four factors are based on the theory of conceptualizing stigma,25 and the rationale that they are key questions of mental health stigma regarding the attribution of biogenetic explanation can be summarized as follows. First, there has been a strong argument that biogenetic explanation can reduce stigma by diminishing attribution of personal controllability followed by decreased perceived blame. Second, biogenetic concept might endorse stigma of violent patients with mental disorders by promoting the view of patients as individuals with lack of control. Third, biogenetic causal belief could deepen the thinking that mental disorders are rooted on genes or brain abnormalities and therefore are difficult to cure, yielding pessimism. Fourth, biogenetic attribution, such as genetic or brain problems, would separate ‘us’ and ‘them’ by making people reluctant to have close relationships with patients.
Based on the framework of above previous studies, we attempted to conduct further analyses with an increased number of studies, especially focusing on subgroup analyses by target audience, types of mental disorder, and cultural background. In addition, we decided to add the question on the ‘attitude toward help-seeking’ itself as an outcome measure since we assumed that the final goal of this work was to reveal how the stigma becomes an obstacle to mental health service use. In a systematic review and meta-analytic study,26 the attitude toward help-seeking was identified as a key factor affecting use of mental health service.
‘Attitude toward help-seeking’ refers to the perception of the need for help (i.e., willingness to seek help from others if someone develops a mental disorder26). ‘Blame’ refers to the responsibility of the mental disorder on the affected individual. ‘Perceived dangerousness’ refers to fear and an unpredictable risk felt by mentally ill people. ‘Prognostic pessimism’ refers to a negative view of the treatability, recovery, and prognosis of mental disorders. ‘Social distance’ refers to unwillingness to have social relationships with mentally ill persons (e.g., unwillingness to live near them).
Data analyses
The experimental and correlational studies were analyzed separately. We used Review Manager (version 5.4.1) in our analyses. As mental health stigma is a complex and abstract issue, a kind of scale is needed to measure this subjective concept as an objective value. Although our meta-analysis was conducted on five core factors of stigma, each study included in the analyses used different outcome measures for each core factor. Also, each study targeted different kinds of population and mental disorders. Considering that the outcome measure is an abstract and multifaceted concept and the included studies are very heterogeneous, we decided to use a random effect model, and Cohen’s d value was used for the effect size.2728
The mean and standard deviation were processed using the following equation:
 .
.Odds ratios were processed using the following equation:
 .
.Correlation r and regression beta values were processed using the following equation:
 ,
,with r = 0.98β + 0.05ë (If β < 0, then λ = 0; if β > 0, then λ = 1) (Peterson and Brown, 2005).
Subgroup analyses
We performed subgroup analyses to explore whether the outcome measures differed between important categories. We classified the studies by the type of mental disorder (psychotic vs. neurotic vs. general mental disorders), subjects (patients vs. general population), and cultural background (Western vs. Eastern countries). As we mentioned in the introduction section, different effects of biogenetic explanation have been shown in previous studies according to those factors.2930 For the type of mental disorder, the different influence was mainly caused by different severity and prognosis of mental illnesses,29 therefore, we decided to largely divide mental disorders into psychosis and neurosis. Since there were studies in which the target of explanation was just a general mental illness, we set the type of mental disorder into these three categories: psychotic, neurotic, and general mental disorders.
RESULTS
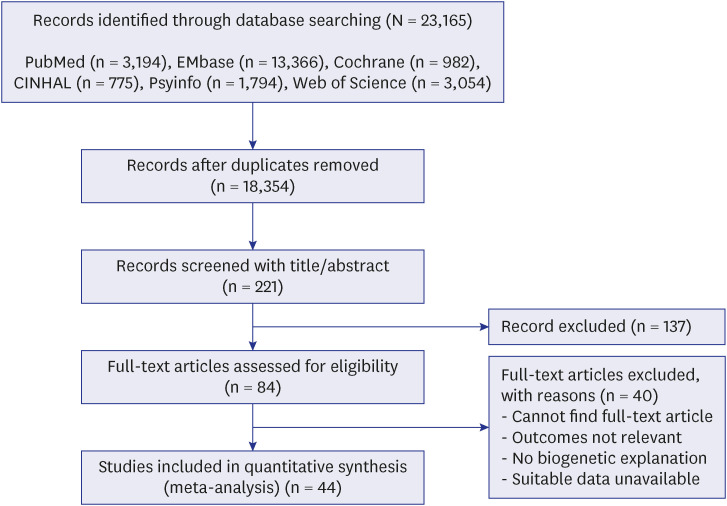
A total of 44 studies were included in the meta-analysis, of which 24 were experimental and 20 were correlational (Fig. 1). The experimental studies evaluated the outcome measures of attitude toward help-seeking (n = 7), blame (n = 11), perceived dangerousness (n = 7), prognostic pessimism (n = 11), and social distance (n = 7). The correlational studies evaluated the outcome measures of attitude toward help-seeking (n = 6), blame (n = 3), perceived dangerousness (n = 5), prognostic pessimism (n = 2), and social distance (n = 11).
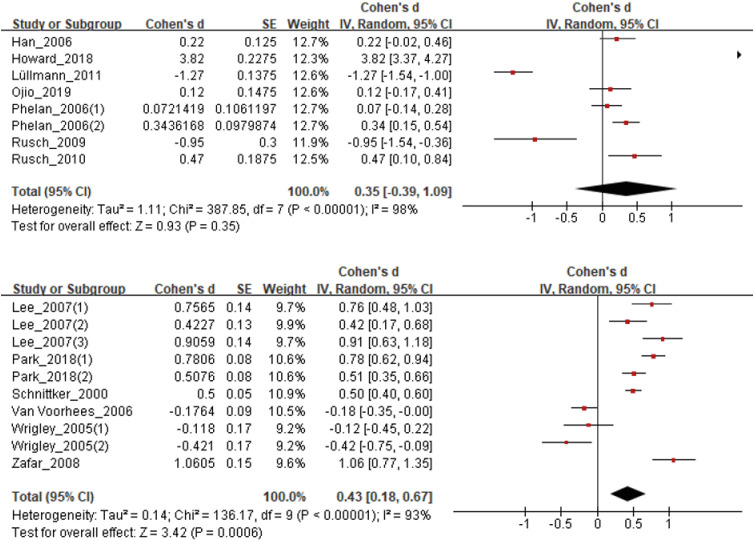
Attitude toward help-seeking
In experimental studies, a positive attitude toward help-seeking behavior was observed in the group provided with biogenetic explanations for mental disorders compared to the control group, albeit without statistical significance (d = 0.35; 95% confidence interval [CI], −0.39 to 1.09; P = 0.352). In correlational studies, a positive attitude toward help-seeking behavior was significantly related to having a biogenetic concept of mental disorders (d = 0.44; 95% CI, 0.21 to 0.66; P < 0.001; Fig. 2). Subgroup analyses of the correlational studies showed differences in the relationship between thoughts related to the cause of mental disorders and attitudes toward help-seeking behavior between Western and Eastern countries (d = 0.73; 95% CI, 0.55 to 0.90; P < 0.001; Supplementary Fig. 1). A positive attitude toward help-seeking was significantly related to having a biogenetic concept in Eastern, but not Western, countries. In experimental studies, a more positive attitude toward help-seeking was observed in the general population, but not among patients, after being provided with a biogenetic explanation (d = 0.60; 95% CI, −0.021 to 1.42).
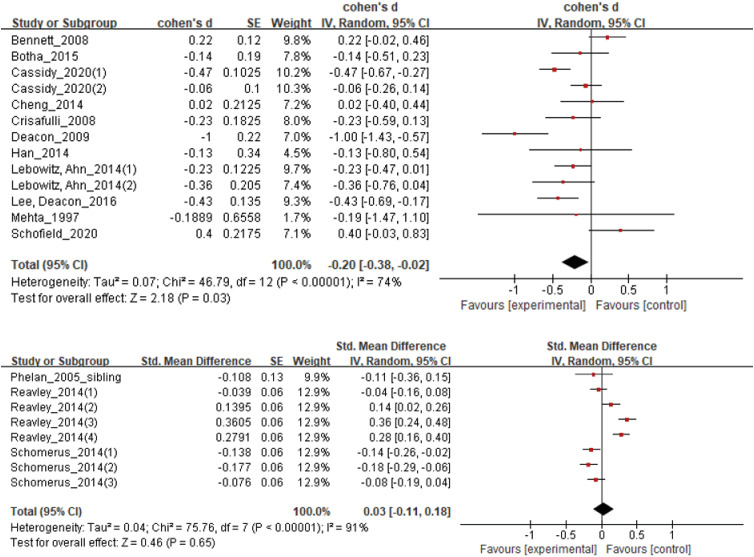
Blame
In experimental studies, a decreased level of blame was significantly related to be provided a biogenetic explanation of mental disorders (d = −0.20; 95% CI, −0.38 to −0.02; P = 0.029). However, in correlational studies, no significant association was observed between the level of blame and having a biogenetic concept of mental disorders (d = 0.03; 95% CI, −0.11 to 0.18; P = 0.646; Fig. 3). Subgroup analysis of experimental studies showed a significant association between the level of blame and being provided a biogenetic explanation of mental disorders in the general population (d = −0.41; 95% CI, −0.63 to −0.19; P < 0.001; Supplementary Fig. 2), but not the patient group. Another result of subgroup analysis of the experimental studies showed a significant relationship between the level of blame and being provided a biogenetic explanation of mental disorders with regard to general mental disorders (d = −0.29; 95% CI, −0.50 to −0.09; P = 0.005; Supplementary Fig. 3), but not for specific mental disorders, including psychotic or neurotic disorders.
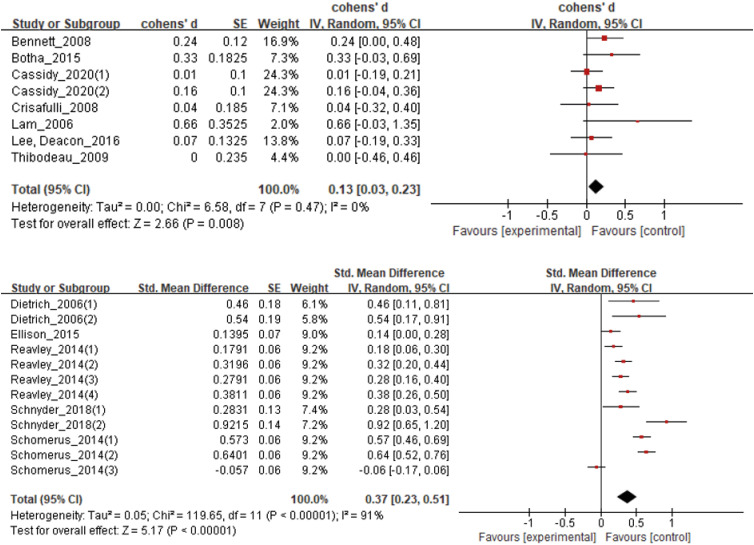
Perceived dangerousness
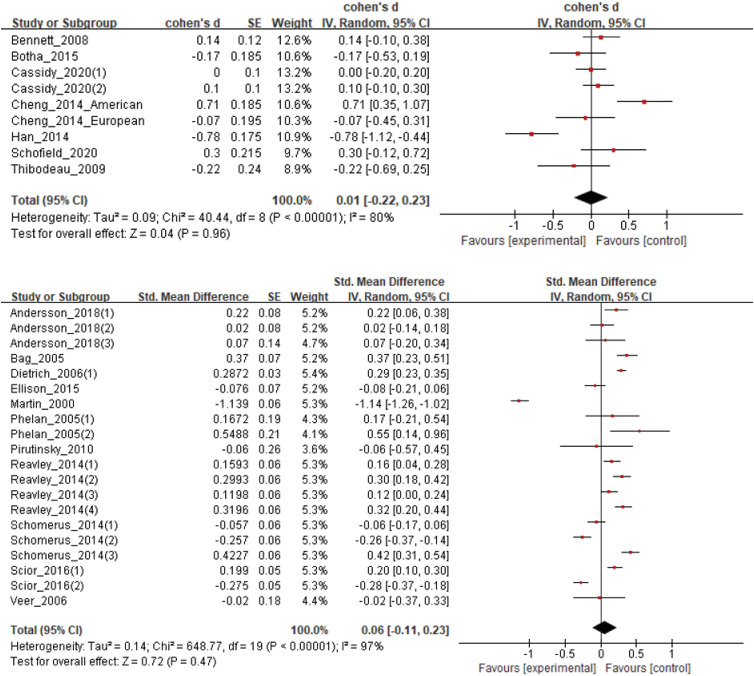
In both experimental and correlational studies, a higher level of perceived dangerousness was significantly associated with the attribution of mental disorders to biogenetic causes (d = 0.13; 95% CI, 0.03 to 0.23; P = 0.008; d = 0.37; 95% CI, 0.23 to 0.51; P < 0.001, respectively; Fig. 4). In subgroup analyses, experimental studies of patients showed that higher perceived dangerousness was significantly related to being given a biogenetic explanation of mental disorders (d = 0.13; 95% CI, 0.02 to 0.23; P = 0.016; Supplementary Fig. 4). Otherwise, no significant difference was observed in the subgroup analyses.
Prognostic pessimism
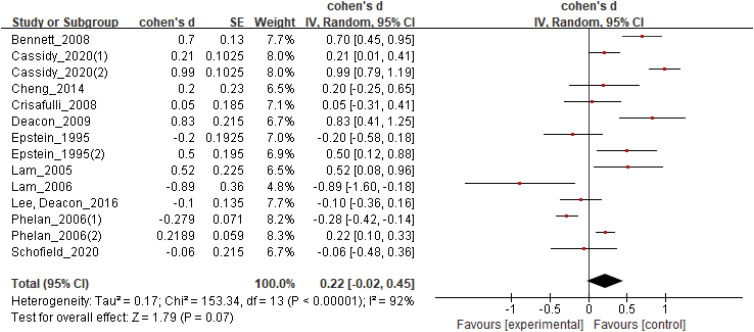
In experimental studies, people who were provided biogenetic explanations tended to show higher levels of prognostic pessimism compared to those who were provided those kinds of explanations, albeit without statistical significance (d = 0.22; 95% CI, −0.02 to 0.45; P = 0.073; Fig. 5). Due to the small number of correlational studies on prognostic pessimism, they were not analyzed. In subgroup analyses, experimental studies conducted in the general population showed a significant association between biogenetic explanation and prognostic pessimism, whereas the studies in patients showed a negative correlation (d = 0.31; 95% CI, 0.05 to 0.56; P = 0.018; d = −0.42; 95% CI, −1.19 to 0.34; P = 0.276, respectively; Supplementary Fig. 5). Otherwise, no significant difference was observed in the subgroup analyses.
Social distance
In correlational studies, the level of social distance was higher in the group with, compared to without, a biogenetic concept of mental disorders, albeit without statistical significance (d = 0.06; 95% CI, −0.11 to 0.23; P = 0.472; Fig. 6). In experimental studies, there was no significant relationship between level of social distance and biogenetic explanation of mental disorders.
DISCUSSION
The present study showed that providing a biogenetic explanation (experimental studies) and having a biogenetic concept (correlational studies) of mental disorders were associated with various categories of stigma related to the use of mental health services. In addition to four categories suggested by previous studies,181920 we evaluated ‘attitude toward help-seeking,’ which is an important component regarding stigma toward mental disorders.26 Our findings are generally consistent with the results of previous studies.
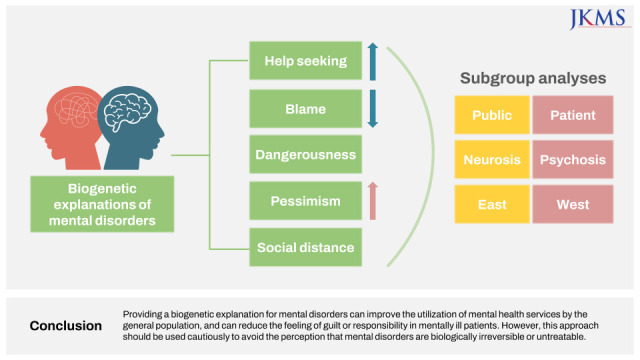
A summary of our results is shown in Fig. 7. Biogenetic explanation was related to a positive attitude toward help-seeking in both experimental and correlational studies, even though the results were significant only for experimental studies. In correlational studies, the association was observed in studies conducted in Eastern, but not Western, populations. Provision of a biogenetic explanation (experimental studies) of mental disorders decreased the level of blame, especially in the patient group, while no such relationship was observed in correlational studies. Perceived dangerousness was positively associated with biogenetic explanation in both experimental and correlational studies while prognostic pessimism showed a tendency of positive relationship close to the level of significance (P = 0.073) with biogenetic explanation in the experimental studies. Furthermore, social distance was not confirmed to be related to biogenetic causal attribution in both study types.
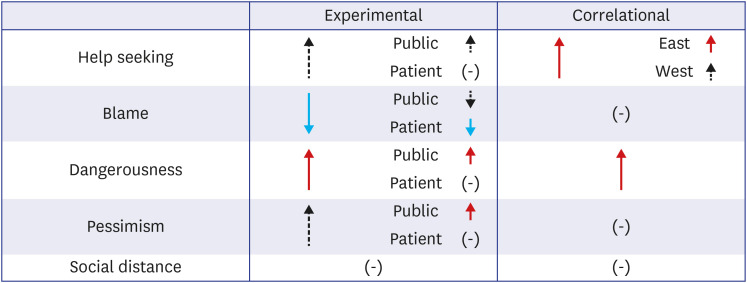
Fig. 7
Outcome of meta-analysis. Solid line arrows denotes a significant results. Red arrows: significantly increased results; Blue arrows: significantly decreased results; Black dotted arrows: increasing or decreasing tendency, while statistical significances were not shown; (-): no any definite tendency.
![]()
Although experimental and correlational studies showed similar results, experimental meta-analyses exhibited more significant findings for the associations between biogenetic explanation and stigma measures. Loughman and Haslam20 suggested that the differences in the results of experimental and correlational studies are because correlational studies include greater numbers of confounding factors and moderator variables. Experimental studies are more useful to detect the influence of causal attribution, including biogenetic explanations, on people’s thoughts regarding mental disorders.
Attitude toward help-seeking is an important factor for the use of mental health services.31 Barker et al.32 studied the individual and structural determinants of help-seeking behavior, including personal beliefs, internalized gender norms, self-efficacy, and perceived stigma. Therefore, seeking help for mental problems reflects individuals’ internalized positive and affective attitudes toward mental disorders,26 as well as thoughts about mental health service use. Several studies have shown the effect of biogenetic explanations or biological causal beliefs on the intention to seek and behavior of seeking help, but no relevant meta-analysis has been conducted. In the present study, we found that having a biogenetic concept was significantly related to a positive attitude toward help-seeking. Only correlational studies showed a significant association between biogenetic concept and positive attitude toward help-seeking, while there was no significant finding in experimental studies. The significance in correlation studies has possibly been influenced by confounding factors related to the familiarity with biogenetic concepts, such as having mental disorder and taking psychiatric medicine. On the other hand, in experimental studies that attempted to see the effect of biogenetic explanation under controlled conditions, the attitude toward help-seeing did not change to a significant level. Differences in results according to research design have been similarly reported in other meta-analysis study.20
Subgroup analysis showed that interventions led to greater help-seeking behaviors in the general population than the patient group. Therefore, providing a biogenetic explanation for mental disorders during public education may promote the use of mental health services. Another subgroup analysis indicated that having a biogenetic concept significantly correlated with help-seeking behaviors in Eastern, but not in Western, countries. In Eastern cultures, people are more likely to believe that mental disorders are a sign of personal weakness, and that having a mentally ill family member brings shame to the entire family.29 Eastern populations generally consider mental disorders to originate from individual or family conflict, rather than as treatable medical problems with biological origins.3334 Therefore, biogenetic explanations can reduce the threshold of help-seeking in Eastern regions, in particular.
In line with a previous meta-analysis,20 the present study showed that a biogenetic explanation lowers the blame toward mentally ill people. This is supported by the attribution theory that the responsibility for diseases can be reduced by legitimizing psychiatric disorders as “real” and rooted in the brain. Weiner3536 suggested that the belief that patients are responsible for their mental disorders can provoke pity and anger toward them, leading stigmatizing behavior. In particular, studies conducted in the patient group showed that a biogenetic explanation significantly lowered blame toward people with mental disorders. This might be because patients’ self-stigma, which reflects internalized negative mental health-related attitudes and beliefs, was reduced by a biogenetic explanation.37 Therefore, providing patients with a biogenetic explanation of mental disorders may help reduce their internalized stigma. For subgroup analysis by the types of mental disorder, only experimental study targeted general mental disorder showed significant relationship between biogenetic explanation and decreased level of blame. The lack of significant results for specific mental disorders may be due to the small number of studies involved. And, there is a possibility that individuals have a more flexible attitude toward person with general mental problems than those with specific mental illness. Further studies on stigma for specific mental disorders are needed.
On the other hand, biogenetic explanation increases perceived dangerousness and tended to increase prognostic pessimism. The belief that a mental disorder has a biomedical basis can lead people to believe that people with mental disorders are less able to control their symptoms. This belief can, in turn, foster the perception that an individual with a mental disorder is dangerous and unpredictable.3839 The present study included a larger number of studies on prognostic pessimism (n = 10) than a previous meta-analysis,20 and showed increased prognostic pessimism with biogenetic explanations, although there was a lack of statistical significance. In particular, these results were found in the subgroup of the general population. Providing a biogenetic explanation might create a perception that mental illness is a “deep-seated” problem in the brain of mentally-ill people, which is less likely to be treatable.40 Therefore, biogenetic explanations should be provided cautiously, and it is necessary to provide adequate and accurate information about the prognosis, as well as emphasize the effectiveness and importance of treatment.
A previous meta-analysis showed that, in experimental studies, biogenetic explanation was significantly related to social distance toward individuals with mental disorders.20 Even though we did not find a similar association in our study, despite including a greater number of studies, we identified a trend toward increasing social distance with biogenetic explanations. When providing biogenetic explanations of mental disorders, it is important to emphasize that people with a mental illness are not different types of people or people who are difficult to get along with.
In the present study, the effect of biogenetic concepts on attitudes toward mental illness was analyzed using five outcome measures. We comprehensively evaluated the effect of biogenetic explanations on various aspects of mental health stigma. This is the first meta-analysis that has evaluated the attitude toward help-seeking for mental health problems and its relationship with a biogenetic explanation. Compared to previous meta-analyses, we included a larger number of studies. In addition, we performed subgroup analyses to compare the results between mental disorder types, audience targeted for education, and cultural background. We expect that our results will be useful for formulating strategies for mental health education.
This study had several limitations. First, the number of studies for certain stigma measures was insufficient to reach statistical significance, although we included a greater number of studies than previous meta-analyses. However, we were able to detect the trend toward association for all measures related to biogenetic explanations. Second, the influence of biogenetic explanations was examined by comparing various study subjects with controls. In some studies, control groups were not provided any causal explanation for mental disorders, whereas in other studies control groups were provided a psychosocial explanation. Therefore, it is possible that our results underestimated or overestimated the effect. Additional studies are needed that have a homogeneous study design to confirm the influence of providing a biogenetic explanation. Third, although we conducted subgroup analyses for different types of mental disorders, populations, and cultural backgrounds, we could not compare the results across different subgroups, and only reported the results for individual subgroups. Additional meta-analyses with a greater number of studies are needed to confirm the differences observed in our study.
Having a biogenetic concept of mental illness increased the positive attitude toward help-seeking and decreased blame toward individuals with mental disorders. However, it also increased perceived dangerousness and prognostic pessimism. Social distance was not confirmed to be related to biogenetic explanation. Providing a biogenetic explanation for mental disorders can improve the utilization of mental health services by the general population, and can reduce the feeling of guilt or responsibility in mentally ill patients. However, this approach should be used cautiously to avoid the perception that mental disorders are biologically irreversible or untreatable.
 XML Download
XML Download