

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) before emergence of the omicron variant demonstrated low rate of infectivity and mortality in children compared to that in adults.1 However, a new severe acute respiratory coronavirus 2 (SARS-CoV-2) omicron variant (B.1.1.529) has been reported in South Africa.2 In South Korea, this variant, also referred to as COVID-19 omicron, began to spread from November 25th, 2021. The omicron variant reduced the risk of severe disease compared with the original strain and other variants, but it appeared to be highly infectious, which resulted in an exponential increase in confirmed cases in South Korea.3 As the number of confirmed cases increased, so did the number of pediatric patients’ hospitalization.2
A febrile seizure is characterized by a neurologic event associated with a fever that usually occurs between 6 months and 5 years of age without evidence of a central nervous system infection. Most cases are benign, but some progress to encephalitis and meningitis and thus require differentiation from other diseases.4 Some studies have reported that the correlation between COVID-19 and febrile seizure associated with their ability to affect the central nervous system.567
To the best of our knowledge, the relationship between an increase in the number of febrile seizures in pediatric patients with identified omicron variant infection is unknown and has not been evaluated so far. Thus, this study aims to compare the frequency and clinical features of febrile seizure before and after the emergence of the omicron variant. We also aim to compare the clinical characteristics of febrile seizure between patients with and without COVID-19.
Go to : 
METHODS
Study population and definition
We retrospectively reviewed medical records of children aged under 18 years with febrile seizure who were tested for COVID-19 and visited the emergency department (ED) of Ajou University Hospital, South Korea. We collected data of patients with fever and seizure as the chief complaint or who were diagnosed with International Classification of Disease (ICD)-10 code of R56.0 (febrile convulsion). We also collected data on the total number of pediatric patients who visited ED for medical problems and COVID-19 positive patients.
We defined a simple febrile seizure as a generalized tonic-clonic seizure lasting less than 15 minutes occurring only once in 24 hours in a child between 6 months and 5 years of age with a fever of 38°C. A seizure lasting more than 15 minutes in a child less than 6 months or more than 5 years of age and occurring more than once in a 24-hour period is defined as a complex febrile seizure.4 Febrile status epilepticus is defined as any prolonged seizure or recurrent seizure lasting for more than 30 minutes without return to full consciousness.8
Based on the first confirmed pediatric case in Korea, we defined the pre-omicron period as the period from February 2020 to December 2021.910 In addition, the omicron period was defined as the period from January 2022 to April 2022, where the omicron variant accounted for more than 50% of variant tested in Korea.311 The definition of COVID-19 positive was confirmed by polymerase chain reaction (PCR).
The exclusion criteria were established as follows: patients with central nervous system infection or inflammation, seizure with provocation factor (e.g., trauma, acute systemic metabolic abnormality), history of previous epilepsy or non-febrile seizure, insufficient medical records, and patients with no COVID-19 diagnosis.
Data collection
Clinical characteristics included age (in months), sex, year and month of ED visit, mental status in ED (A, alert; V, verbal; P, painful; U, unresponsive), underlying disease, previous febrile seizure history, and family history. Seizure features included seizure duration (in minutes), total seizure number in a 24-hour period, form (generalized tonic-clonic/tonic/clonic, atonic, focal, others, or unknown), and peak body temperature. Treatment provided in ED, including anticonvulsant therapy, antipyretics, and other medications, were also reviewed. The ED outcomes included frequency of discharge from the ED, hospitalization (overall and intensive care units [ICUs]), transfer to a tertiary hospital, length of hospitalization, and in-hospital mortality.
The primary outcome was comparison of clinical characteristics and ED outcome of febrile seizure between the pre-omicron and omicron period. Furthermore, we compared the patient characteristics according to COVID-19 diagnoses during the omicron period.
Statistical analysis
The continuous variables are described as medians with interquartile ranges (IQR), and the categorical variables are presented as numbers and percentages. The outcomes were compared between the 2 groups using the Chi-square or Fisher’s exact tests for categorical variables and the Mann-Whitney U test for continuous variables. P values less than 0.05 were considered statistically significant. Statistical analyses were performed using Stata software, version 15 (StataCorp LLC, College Station, TX, USA).
Ethics statement
This study was approved by the Institutional Review Board of Ajou University School of Medicine with a waiver for informed consent from the patients (IRB No. AJIRB-MED-MDB-22-182).
Go to :
RESULTS
Clinical characteristics of febrile seizure between pre-omicron and omicron periods
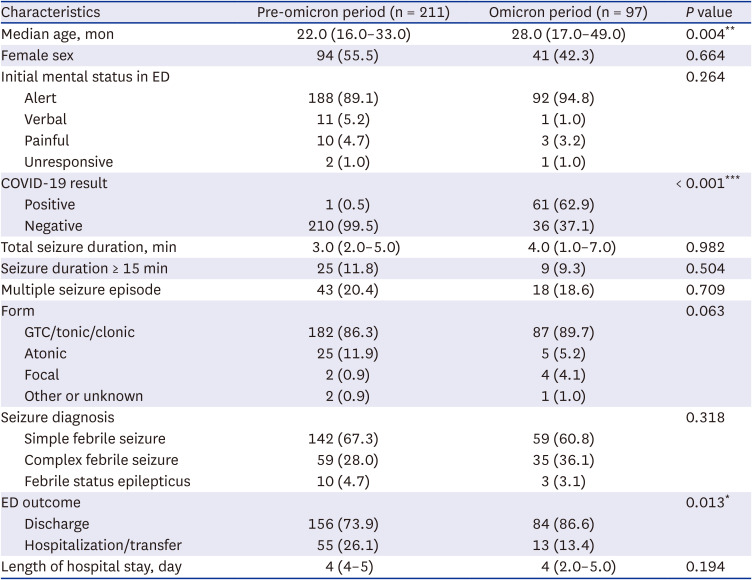
Data of a total of 878 children were reviewed and 308 were included in this study (Fig. 1). Among the excluded cases, one case was excluded because the patient was finally diagnosed with post-COVID-19 autoimmune encephalopathy. The selected 308 children were divided into pre-omicron period (n = 211) and omicron period (n = 97) as per their date of diagnosis. As per the number of months, there were about 9.2 patients of febrile seizure per month in the pre-omicron and 24.3 patients per month in the omicron period. Table 1 shows the difference in clinical characteristics of febrile seizure between the two periods. Compared with the pre-omicron period, patients in omicron period showed significantly higher mean age (pre-omicron vs. omicron, 22.0 vs. 28.0 months; P = 0.004) and COVID-19 positive results (pre-omicron vs. omicron, 0.5% vs. 62.9%; P < 0.001). For ED outcomes, the hospitalization and transfer rate was higher in the pre-omicron period.
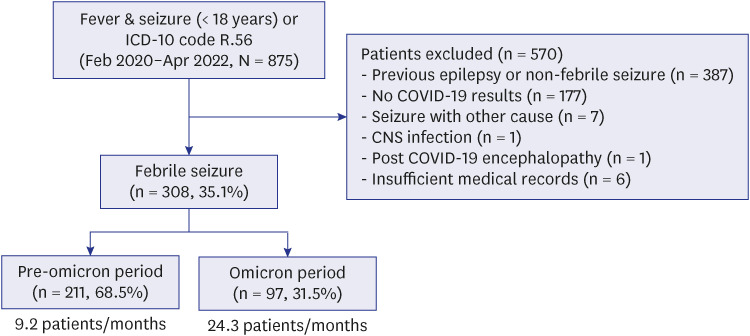 | Fig. 1Flowchart for the selection of the study population.ICD = International Classification of Disease, COVID-19 = coronavirus disease 2019, CNS = central nervous system.
|
Table 1
Clinical characteristics of febrile seizure between pre-omicron and omicron periods
Values are expressed as medians (interquartile rages) or numbers (%).
ED = emergency department, COVID-19 = coronavirus disease 2019, GTC = generalized tonic-clonic.
*P < 0.05, **P < 0.01, ***P < 0.001.
![]()
Total number and frequency of patients with COVID-19 and febrile seizure between the Pre-omicron and omicron periods
Approximately 642 and 789 patients visited the ED monthly during the pre-omicron and omicron period, respectively. The frequency of COVID-19 positive patients increased from 2 patients per month to 219.3 patients per month, while the proportion of COVID-19 positive patients form the total number of pediatric patients was 0.3% and 27.8% in the pre-omicron and omicron period, respectively. In addition, the number of patients with COVID-19-associated febrile seizure increased in the omicron period, and of the COVID-19 positive patients, 7.0% were diagnosed with febrile seizure (Table 2).
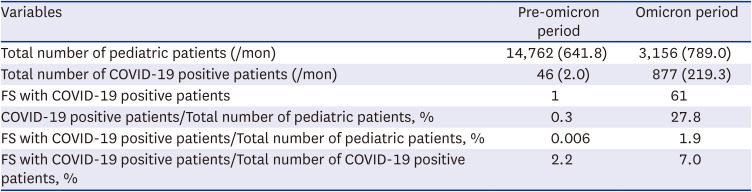
Table 2
Total number and frequency of patients between Pre-omicron and omicron periods
![]()
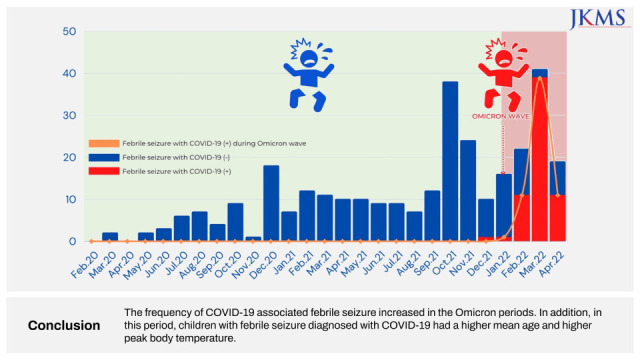
The monthly data on confirmed cases of COVID-19 in patients under 19 years of age in Korea (Fig. 2A) and distribution of COVID-19 associated febrile seizure cases were compared (Fig. 2B). As the number of confirmed cases of COVID-19 in children increased, the cases of number of COVID-19 associated febrile seizure also increased. Monthly distribution showed that most patients diagnosed with febrile seizure with COVID-19 were from February 2022 to April 2022.
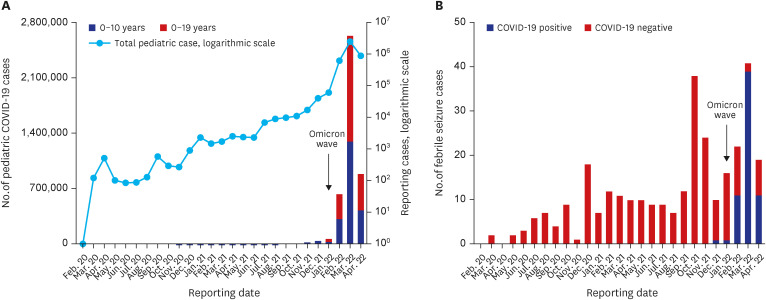 | Fig. 2Title. Numbers of patients with COVID-19 and febrile seizure. (A) Monthly cases of COVID-19 in children aged < 19 years in Korea. Shaded and open bars indicate the number of COVID-19 positive cases for ages 0–10 and 10–19 years, respectively, on a linear scale. Gray lines indicate the total number of pediatric cases on a logarithmic scale. (B) Monthly cases of febrile seizure in children aged < 18 years. Shaded bars indicate the number of febrile seizure cases confirmed to be positive with COVID-19 whereas the sum of the shaded and open bars indicates the total number of febrile seizure cases.COVID-19 = coronavirus disease 2019.
|
Febrile seizure with positive COVID-19 vs negative COVID-19 in omicron period
Among the 97 children with febrile seizure in the omicron period, 62.9% children were confirmed to be positive for COVID-19 (Table 3). The COVID-19 positive group showed statistically significant higher mean age than the COVID-19 negative group (positive vs. negative, 33.0 vs. 23.0 months; P = 0.003). Of the COVID-19 positive group, 15 children were aged more than 6 years, and the oldest patient, aged 11 years, had no history of febrile seizure or neurologic disease. Additionally, the COVID-19 positive group showed higher peak body temperature than the COVID-19 negative group (positive vs. negative, 39.1°C vs. 38.6°C; P = 0.030). Despite the lack of significance, the COVID-19 positive group showed longer seizure time, multiple seizure episodes, and higher prevalence of complex febrile seizure.
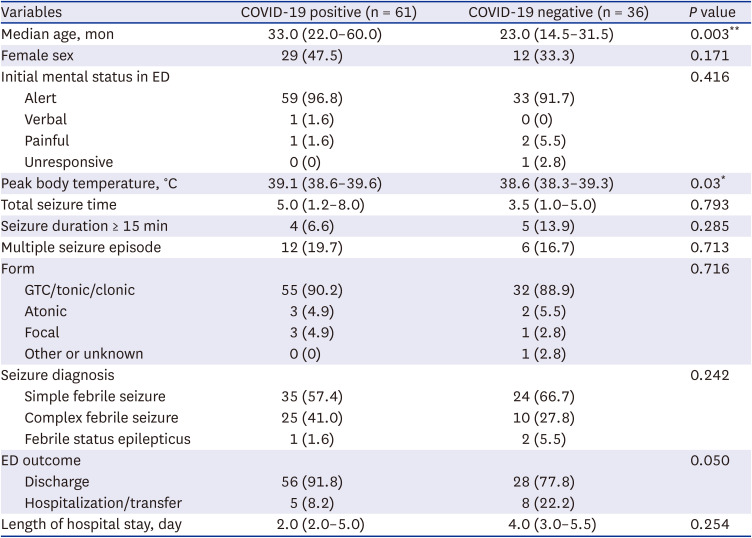
Table 3
Clinical characteristics of febrile seizure with COVID-19 in omicron periods
Values are expressed as medians (interquartile rages) or numbers (%).
COVID-19 = coronavirus disease 2019, ED = emergency department, GTC = generalized tonic-clonic.
*P < 0.05, **P < 0.01.
![]()
For ED outcomes, 3 patients were admitted to the general ward in the COVID-19 positive group. In the COVID-19 negative group, 8 patients were admitted to the general ward. No in-hospital mortality occurred in both groups.
Characteristics of 3 specific cases with febrile seizure and COVID-19
Among 61 children in the COVID-19 positive group, 3 children exhibited a considerable number of clinical features (Table 4). Patients 1 and 2 were girls aged 24 months and 28 months, respectively; they came to the ED with generalized seizures. After seizure cessation, the patients showed Todd’s palsy and recovered to normal status after anti-seizure therapy.
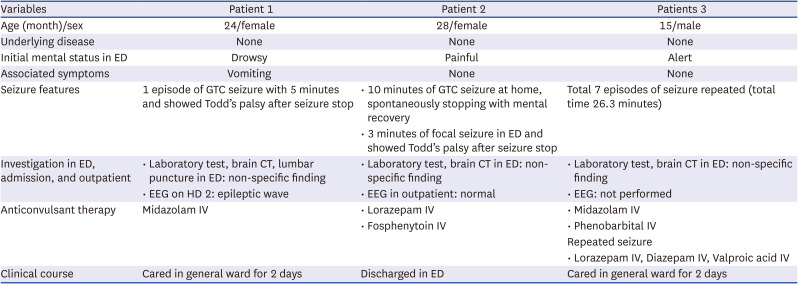
Table 4
Characteristics of three specific cases with febrile seizure and COVID-19
CT = computed tomography, ED = emergency department, EEG = electroencephalography, GTC = generalized tonic-clonic, HD = hospital day, IV = intravenous.
![]()
Patient 3, a boy aged 15 months, with no previous febrile seizure history presented to the ED with 7 episodes of generalized seizure. The patient received 1st and 2nd line anticonvulsant therapy and was admitted to the general ward. Laboratory investigations and brain computed tomography showed no abnormalities.
Go to :
DISCUSSION
This retrospective analysis found that the number of febrile seizures with SARS-CoV-2 infection increased in February 2022, correlating with emergence of the omicron period. Data shows that children with febrile seizure who were COVID-19 positive were of a higher age group and had longer seizure time, multiple seizure episodes, and higher prevalence of complex febrile seizure than COVID-19 negative children.
In the COVID-19 era, many countries practiced social distancing measures to prevent transmission of COVID-19.12 With the help of social distancing and hygiene precautions, the prevalence of febrile seizure decreased by 38% in 2020 compared to that in 2010-2019 in South Korea.13 In a Hong Kong-based study, seizure-related accidental ED visits significantly decreased in 2020 (relative risk, 0.379; 95% confidence interval [CI], 0.174–0.526; P < 0.001); in addition, the rate of febrile seizure-related admissions dropped to less than 20% compared to the previous year, in children aged 0–6 years.7
In a previous study conducted in children aged 0 to 5 years in the pre-omicron period (from March 1, 2020 to April 19, 2021), only 0.5% (44/8,854) of the COVID-19 patients were diagnosed with febrile seizure.6 The median age was 1.5 years, and 68.2% (30/44) were cases of simple febrile seizure. Prognosis of febrile seizure patients was good, and only 25% of the cases required hospitalization and few required critical care. A meta-analysis comparing 20 studies with 3,051 hospitalized patients aged under 18 years with COVID-19 reported that only 4% (95% CI, 2–6%; 2 studies) of the patients presented with seizure from December 31, 2019 to December 15, 2020.14
In the omicron period, the high infectivity and an ensuing rapid increase in the number of both adult and pediatric COVID-19 patients put a large burden on the medical infrastructure of many countries. Especially, hospitalization associated with pediatric COVID-19 rapidly increased.2 In South Africa, convulsion was a symptom in 25/139 (20%) hospitalized patients. In addition, seizure accounted for 20% of clinical diagnosis for hospitalization, which was the most frequent diagnosis along with gastroenteritis.15 In our study, the number and rate of ED visit associated with COVID-19 rapidly increased in omicron period. During this period, the number of COVID-19 associated febrile seizures was increased and 7.0% of COVID-19 positive patients were diagnosed with febrile seizure.
In our study, febrile seizure in the COVID-19 positive group was shown to occur in patients with a higher mean age than that of the COVID-19 negative group. The peak age of incidence of febrile seizure in children is 12 to 18 months.416 In this study, the mean age of febrile seizure in the COVID-19 positive group was 33.0 months, and 15 patients were more than 6 years of age. In a previous study in South Africa, 6 of 25 patients with seizure were outside the typical age range for simple febrile seizure.2 In a Swedish case report, 3 patients were hospitalized for COVID-19 with febrile seizure, and 2 of them were aged 3 months and 14 years, respectively, which was outside the typical age range for simple febrile seizure.5
Based on the observations, we suggest several potential causes for an increase in the number of patients with febrile seizure during the omicron period. First, it is possible that the increase in the total number of COVID-19 positive pediatric patients during the omicron period contributed to the increase in the total number of febrile seizure patients. However, considering the ratio of febrile seizure to the total patients, there are certain features of the omicron variant that may explain why it causes more febrile seizures. Second, the COVID-19 positive group had significantly higher peak body temperature than the negative group. Since febrile seizure is associated with viruses that cause high fever such as human herpes virus and influenza,17 the higher peak body temperature caused by SARS-CoV-2 infection in the omicron period may have potentially caused the increase in prevalence of febrile seizure. Third, the febrile seizures most commonly occurring in fall and winter18 are associated with viruses such as influenza and respiratory syncytial virus, which mainly cause upper respiratory tract infections.4161920 The omicron variant was found to cause more croup in previous studies.321 Emergence of the omicron variant in 2022 may have resulted in an increase in the prevalence of febrile seizure due to more upper respiratory tract infections than that of other variants.
In the general population, complex febrile seizure accounts for approximately 20–30% of febrile seizures.2223 Although statistically insignificant, our study has shown that COVID-19 positive group had a higher ratio of complex febrile seizure (41.0%) and multiple seizure episodes than the negative group. Based on these characteristics, it is important to inform caregivers of seizure recurrence and to educate patients’ caretakers on emergency seizure management at home.
The potential mechanism of COVID-19 causing seizure, as introduced in many studies, is associated with direct viral injury to neural cell and inflammation. The neurotropic and neuroinvasive nature of COVID-19 cause neuronal infection through angiotensin converting enzyme 2 in brain endothelial cells leading to a cascade of inflammation.242526 The inflammation is mediated by cytokines such as IL (interleukin)-1β, IL-6, tumor necrosis factor-α, and IL-17. The cytokines activate glial cells leading to a hyper-inflammatory response causing increased neurologic excitability and putting children at a higher susceptibility to experience febrile seizure.2728 The different prevalence of febrile seizure between adults and children due to COVID-19 is related to the difference in blood-brain barrier and neurovascular unit.29 Owing to the age-based changes in the blood-brain barrier and neurovascular unit, children and adults respond differently to direct neural injury by COVID-19.30 However, it is uncertain whether the omicron variant is more neurotropic and neuroinvasive than the other variants and would require further research to elucidate these results.
In this study, most patients were discharged without neurologic sequelae and no deaths occurred in the hospital. Although excluded from this study, one patient showed a notable clinical course. A boy aged 16 months, presented to the ED with 4 episodes of generalized seizures continuing for a total of 183 minutes. Other complaints were upper respiratory symptoms and respiratory distress. The patient was clinically diagnosed with status epilepticus and severe croup. Despite being treated with an anticonvulsant drug, the seizures continued and caused respiratory suppression which led to intubation and admission to the ICU. The patient received midazolam coma therapy and intravenous remdesivir. During the hospitalization, the patient showed multiple episodes of focal seizure and was finally diagnosed with post COVID-19 autoimmune encephalopathy on brain magnetic resonance imaging and treated with intravenous immunoglobulin. After discharge from the ward, the patient had an episode of focal seizure, motor dysfunction, and blindness. Recently his motor weakness and visual acuity have recovered. The patient undergoes follow-up visit in the outpatient clinic and is on anticonvulsant for partial seizure. Neurological involvement in most patients was known to be transient. Although rare, life threatening COVID-19 related neurological conditions such as encephalopathy, cerebral edema, and Guillain-Barre syndrome must be considered during management.29
This study has several limitations. First, given the single-center and retrospective design, the results might not be widely applicable. Second, not all children who visited the ED were tested for COVID-19 using PCR. Although this might be a potential bias, it is likely to be negligible because the ratio of children tested for COVID-19 PCR was similar in both, the pre-omicron and omicron, periods. Finally, as not all patients undergo complicated tests to diagnose viruses in the ED, we cannot rule out the coinfection with other viruses along with COVID-19 that may have caused febrile seizure. Considering these multiple potential causes, it is difficult to assess the true incidence of febrile seizure in COVID-19 patients. More studies may be needed to delineate the mechanism for occurrence of omicron variant associated multiple febrile seizure episodes in a higher age.
In conclusion, the frequency of COVID-19 associated febrile seizure has increased in the omicron periods. Among children with febrile seizure, those who tested positive for COVID-19 were older and had a higher peak body temperature than the negative group in the omicron period. Clinicians and caregivers must consider the possibility of complex febrile seizure and multiple seizure episodes in patients tested positive for COVID-19.
Go to :
 XML Download
XML Download