

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The formation of a medical emergency team (MET) is aimed to improve safety in hospitals and prevent adverse events after the sudden deterioration of ward patients [12]. Early response is beneficial in most medical emergencies. In addition, previous studies showed a high risk of mortality in surgical inpatients who required MET activation and improved clinical outcomes from early response within 24 hours of surgical emergencies [345]. The concept of acute care surgery (ACS) was proposed in 2005 and consists of 3 pillars: emergency surgery, trauma, and critical care [6]. The ACS system was introduced in South Korea after the National Trauma Center Project in 2008. Ten years later, the ACS was established in several tertiary hospitals [78]. A previous study suggested a shift to ACS system-optimized scheduling of elective general surgery, allowing enhanced operative productivity and job satisfaction for both ACS and non-ACS general surgeons at the same institution [9]. The concept of “surgical rescue” as another pillar of ACS, was introduced in 2017. In this study, surgical rescue is referred as surgical management for complications caused by invasive procedures and operations [10]. Although the original concept of surgical rescue was confined to the management of operation-related or procedure-related complications, Briggs and Peitzman [11] described an extension of the theme of surgical rescue to medical patients with surgical problems requiring emergency management. Similarly, there may be patients who caught the attention of MET due to surgical problems among hospitalized “medical” patients, and ACS surgeons may improve clinical outcomes especially when rapid surgical intervention is required. Therefore, we designed this study to estimate the clinical significance of ACS as a surgical collaborator for MET in hospitalized patients.
Go to : 
METHODS
The study was approved by the Institutional Review Board of Samsung Medical Center (IRB, No. 2021-02-060) and the requirement for informed consent was waived owing to the noninterventional nature of this study.
Study design and population
This investigation was designed as an observational before-and-after study, conducted in a university-affiliated, tertiary referral hospital between January 2016 and December 2020. Because the ACS system of our institute was established after May 2018, we separated our study period into 2 groups with time gap: January 2016 to December 2017, pre-ACS period; January 2018 to December 2018, window period; and January 2019 to December 2020, post-ACS period.
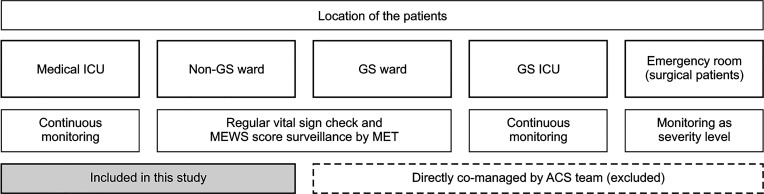
Patients aged >18 years who underwent emergency surgeries performed by board-certified surgeons in the Department of Surgery were included. During the pre-ACS period, emergency surgeries were performed by duty surgeons from various subspecialties. In contrast, during the post-ACS period, emergency operations were mostly performed by the ACS team surgeons. As mentioned above, the purpose of this study was to investigate whether patients with deterioration due to surgical problems, detected by MET activation, could receive improved surgical interventions after ACS implementation; therefore, only inpatient populations were included. Patients hospitalized in the Department of Emergency Medicine or the Department of Surgery of the same institute, which are both directly comanaged by surgeons of the ACS team, were not included. Under our system, ACS surgeons routinely screen inpatients of their own department wards and patients in the emergency room with possibility of surgical etiology, and the decision of emergency operations was directly confirmed by the surgeons. This might have caused measurement errors, so we also excluded such patients from the analysis. Therefore, hospitalized patients from all clinical departments, who were admitted to the general ward and monitored by the MET or intensive care unit (ICU), except for the Department of Surgery, were targeted (Fig. 1).
Data collection, endpoints, and statistical analysis
Patient characteristics were obtained from the electronic medical records (EMR) by the medical record management department under the approval of the IRB. Three investigators separately reviewed the EMR and collected missing data and additional information, such as the level of emergency operations. From the collected data, we excluded nonemergency operations that were miscategorized as “emergency” due to being additionally listed in the operating room schedule during the same day or after 4:00 PM the day before, by policy of the Department of Anesthesiology.
The following data were collected: baseline characteristics including age, sex, time of initial physiologic deterioration, time of surgery initiation, admission department, reason (diagnosis) for surgery, name of the procedure, number of involved duty surgeons, hospital length of stay, length of ICU stay, and in-hospital mortality. The primary outcome was in-hospital mortality after the emergency surgery. The secondary outcome was the time gap between time of alarm recorded by Modified Early Warning Score (MEWS) of >4 within 72 hours and time of initiation of emergency operation, which is defined as an “alarm-to-operation interval” in this study (Fig. 2) [12].
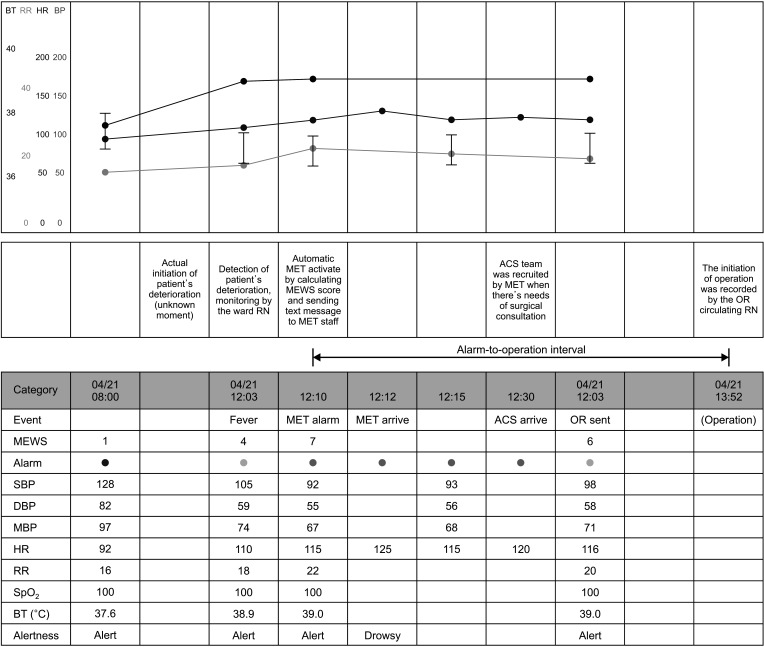 | Fig. 2Patient’s flowchart including Modified Early Warning Score (MEWS) alarm. BT, body temperature; RR, respiratory rate; HR, heart rate; BP, blood pressure; RN, registered nurse; MET, medical emergency team; ACS, acute care surgery; OR, operation room; MEWS, Modified Early Warning Score; SBP, systolic blood pressure; DBP, diastolic blood pressure; MBP, mean blood pressure; SpO2, oxygen saturation.
|
For continuous variables, data were described as mean ± standard deviation if they were normally distributed or as median and interquartile range (IQR) if they were not. Categorical variable data were described as counts (percentages). Student t-test or Mann-Whitney test was used for the analysis of continuous variables; categorical variables were analyzed using Pearson chi-square test or Fisher exact test, where applicable. Statistical analyses were performed using IBM SPSS Statistics for Windows ver. 28.0 (IBM Corp. Armonk, NY, USA), and a P-value of <0.05 was considered statistically significant.
Organization and operation of medical emergency team
The MET at our institute was initiated in March 2009. A set of MET activation criteria was employed. Furthermore, the MEWS of patients is automatically calculated when nurses enter the vital signs of patients into the EMR, and the MET is automatically activated when the calculated MEWS is 7 or higher. The members of the MET consisted of physicians who were on fellowship training in critical care, and either a respiratory therapist nurse or an ICU nurse. The activation criteria and system have been described in previous studies [1314].
Organization and operation of acute care surgery system
In March 2018, the division of ACS was established in the Department of Surgery of our institute. All 5 surgeon-intensivists were certified by the Korean Society of Surgery and the Korean Society of Critical Care Medicine. With this change, the ACS division is responsible for the management of surgical patients in the emergency room, execution of emergency general and trauma surgery, including cooperation of other surgical departments, and surgical critical care for 24 hours Monday through Sunday, except Saturday. The non-ACS divisions of the Department of Surgery continued covering emergency general surgery on Saturday because of significant concerns over the issue of learning opportunities for their fellowship-surgeon training; therefore, Saturday’s operations performed by non-ACS surgeons were not included in the post-ACS group. In addition, division of pediatric surgery, division of vascular surgery, and division of organ transplantation fully covered their respective fields of expertise. Of the 5 surgeon-intensivists, 2 were mainly in the ICU as dedicated intensivists and 3 were mainly in charge of emergency operations with a rotational schedule. Because the ACS division of the institute has no dedicated operating room slot, a similar time latency was required to be assigned to an operating room for emergencies during both periods.
Go to :
RESULTS
Characteristics of patients
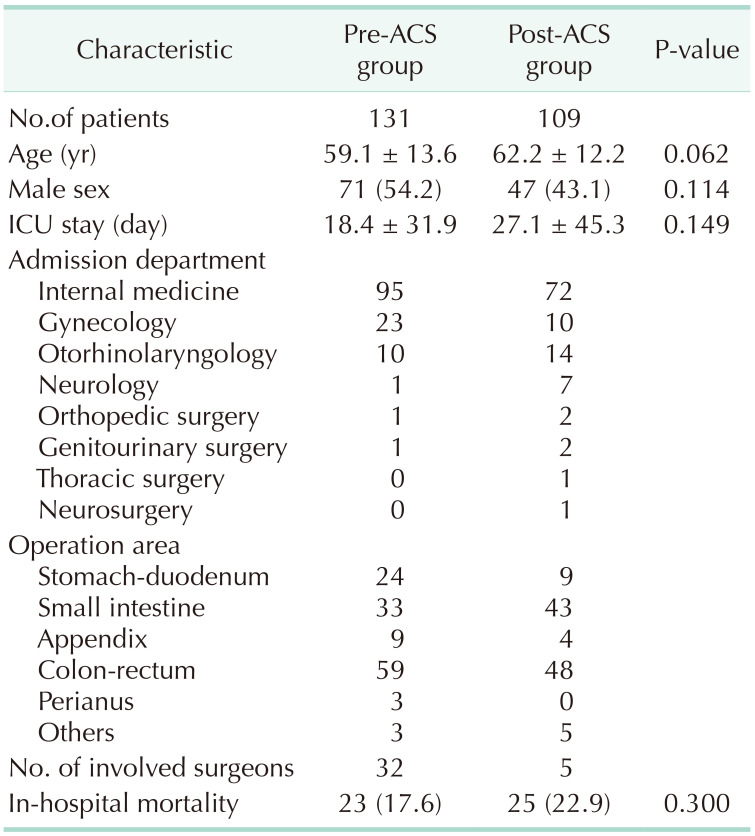
Between January 2016 and December 2020, 1,560 emergency operations on adult patients hospitalized in the clinical departments were included. As mentioned above, patients who underwent surgery during the window period of the system transition (January 2018 to December 2018) were not included. Nonemergency operations that were miscategorized as “emergency” (n = 388), and emergency operations that were planned in the emergency room and performed before ward admission (n = 932) were excluded. Those exceptions were intended to accurately evaluate the alarm-to-operation intervals of the MET and ACS. Finally, 131 patients in the pre-ACS group (January 2016 to December 2017, pre-ACS period) and 109 patients in the post-ACS group (January 2019 to December 2020, post-ACS period) were analyzed. The clinical characteristics of the patients are summarized in Table 1. Among the patients admitted to the Department of Internal Medicine, gastroenterology was the most common subdepartment in the pre-ACS group (47 cases); however, oncology was the most common subdepartment in the post-ACS group (38 cases), followed by gastroenterology (19 cases). Hospital days of each group showed significant differences (37.3 ± 50.6 days in pre-ACS vs. 53.7 ± 53.4 days in post-ACS, P = 0.016). This difference might be due to the higher severity of the post-ACS group; therefore, the duration of ICU days was consequently affected.
Changes of emergency operation after implementation of acute care surgery team
The anatomical areas of operation were divided into the following categories: stomach-duodenum (including gastric resection, gastric or duodenal primary repair, and gastrojejunostomy), small intestine (small bowel resection, small bowel adhesiolysis), appendix (appendectomy), colo-rectum (colon or rectal resection, enterostomy formation), perianus (bleeding control and abscess drainage), and others (hernia reduction, infected chemoport removal, etc.). In both groups, the colorectal area was the most common surgical area.
Before ACS implementation, emergency operations were performed by the duty surgeon of the day, including 22 fellowship surgeons and 10 staff surgeons from every division of the Department of Surgery. However, after the ACS team took responsibility for emergency operations, only 5 dedicated ACS surgeons performed emergency operations, except on Saturdays, as clarified above. Since the Department of Surgery set the duty hour from 6:00 PM to 8:00 AM on the next day, we considered 8:00 AM to 6:00 PM as the reference time for regular working hours. Accordingly, 72 (55.0%) and 51 operations (46.8%) were performed during working hours in the pre- and post-ACS groups, respectively (P = 0.258).
Primary and secondary outcomes
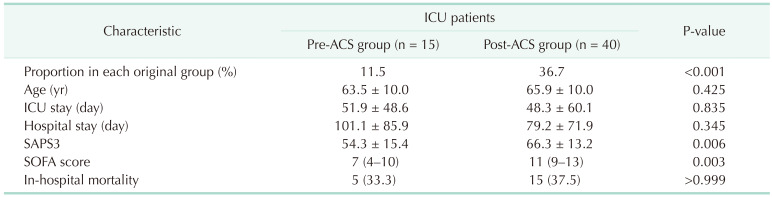
The primary outcome of our investigation revealed no statistical difference in in-hospital mortality after emergency surgery between the 2 groups (17.6% pre-ACS vs. 22.9% post-ACS; P = 0.300, Pearson chi-square test). In addition, the number of patients who were already present in the ICU 72 hours before the emergency operation in each group was significantly different. The Simplified Acute Physiology Score (SAPS) 3 scores [15] of the patients at the time of ICU admission was calculated. Between the 2 groups, a statistically significant difference in the mean SAPS 3 score was identified (54.3 in pre-ACS vs. 66.3 in post-ACS; P = 0.006, Student t-test) (Table 2). The Sequential Organ Failure Assessment (SOFA) score [16] after ICU admission was also analyzed, and the median SOFA score of the pre-ACS group was 7 (IQR, 4–10), and the median of the post-ACS group was 11 (IQR, 9–13), with P = 0.003 by the Mann-Whitney test. We have tried multivariate analysis of mortality; however, none of the other independent variables showed a significant P-value in univariate analysis. Our results suggest that patients in the post-ACS period had more severe clinical conditions, although the overall in-hospital mortality rate was similar between the 2 groups.
The secondary outcome, the alarm-to-operation interval, was defined as the time between the initial vital sign alarm recorded by a MEWS score of >4 within 72 hours and the initiation of emergency operation. Equally, 31 cases in each group of the MEWS alarm were recorded in the EMR and analyzed. The data of the recorded MEWS alarm were only available from the patients in the general ward because continuous monitoring was applied to patients in the ICU, instead of MEWS monitoring by MET, even though the clinical status was worse than patients in the general ward. The mean alarm-to-operation interval in each group was 988 ± 762 minutes (median, 676 minutes; IQR, 408–1,502 minutes) in the pre-ACS group and 584 ± 449 minutes (median, 401 minutes; IQR, 297–781 minutes) in the ACS group. This result showed a statistically significant difference (P = 0.040, Student t-test) (Fig. 3).

Go to :
DISCUSSION
We investigated inpatients who simultaneously required MET intervention and surgical management for decisive treatment at the same time. The main findings of this study are that the collaboration between the MET and ACS may increase the swiftness of management of deteriorated hospitalized patients with surgical etiology. In addition, acute care surgeons tend to perform emergency operations for the management of ICU-admitted patients.
The MET, also known as the rapid response system, has been widely adopted to improve patient safety and reduce hospital mortality [1217]. After the maturation of the system in various medical institutes, many investigators have published reports of specific patient populations in several clinical situations in South Korea. Lim et al. [13], and their follow-up study by Lee et al. [18] suggested that the introduction of the MET improved the time interval from meeting the alert activation criteria to ICU admission, which may improve patient outcomes. Yang et al. [19] suggested that the incidence of preventable cardiopulmonary arrest decreased by 69% after implementation of the system in surgical ward patients. Lee et al. [20] investigated the differences in the clinical characteristics of MET activation between patients admitted to medical vs. surgical services.
Among patients in the medical services, abnormal respiratory rates, abnormal results on blood gas analysis, and low blood pressure were common MET-triggering etiologies. In contrast, low blood pressure, low oxygen saturation, and abnormal heart rate are common causes of MET activation in patients undergoing surgery. These results could be interpreted as those in patients who require surgical intervention with different approaches and management. Additionally, a Canadian study suggested that the occurrence of 2 or more MET assessments conferred the highest odds of mortality in surgical patients [4].
After the development of the ACS system [6], improvements in the surgical department productivity and job satisfaction were suggested [9]. An additional pilar “surgical rescue” was introduced as the distinct role of ACS in the surgical management of complications. Failure to rescue (FTR) was defined as death from unsuccessful management after a major complication [10]. Concern regarding the importance of surgical rescue and FTR continued to emphasize the time interval between the initial deterioration sign and FTR. This concern further emphasized the role of MET [521]. In this study [21], different assessment bundles were applied, such as outreach MEWS score of >3, surgical consultation within 30 minutes, measurement of arterial lactate level, and antibiotics within 1 hour if there was evidence of systemic inflammatory response syndrome or sepsis. The investigators showed that the percentage of patients who entered the operating room within 6 hours was 77.2% in the baseline period. This ratio increased to 80.8% in months 28 to 39 [2122]. Additionally, negative results such as increased morbidity due to delayed management were well described during the coronavirus disease 2019 pandemic [23]. Moreover, the importance of surgical rescue has extended its concept to the emergency management of patients who have surgical diseases that require intervention. A previous study of acute abdominal pathology in medical ICU patients found that 1.3% of patients admitted had acute abdominal symptoms and significant mortality was noted after delays in surgical evaluation and intervention, with 100% mortality in patients who did not undergo surgery. Acute care surgeons should be engaged as a surgical response team to facilitate the management of patients when the MET is concerned about the surgical pathology [1124].
Through the implementation of MET followed by ACS in our institute, we believe that collaboration between the 2 teams improved the safety of hospitalized patients. Patients in the post-ACS group had short alarm-to-operation intervals and high tendency to undergo emergency surgery even when their conditions had already reached the ICU level of care status. However, in-hospital mortality did not improve as expected. This result might be affected by the positive impact of the MET, which had already settled 9 years before the ACS system in the same institute. We tried to investigate the relationship between the time of the day (working hours vs. duty hours) of operation and the alarm-to-operation interval using a concept similar to that of another study [25] to determine the necessity of a dedicated operating room slot; however, our data showed no difference in the time of day between the 2 groups. Additional investigations regarding the availability of surgeons, anesthesiologists, nursing staff, and operating rooms should be conducted to arrive at a conclusion.
Our study had the following limitations: first, the retrospective nature of the study design and selection of patients may lead to some bias in interpretation of the results; second, the result of this study should be carefully considered for generalization because the investigation was conducted in a single institute; third, because the severity of the population was not evaluated except for MEWS, several parameters related to severity might be unexamined.
In conclusion, implementation of the ACS system improved the time delay of surgical intervention in deteriorated hospitalized patients with surgical problems and early detection by the hospital MET. The in-hospital mortality rate after ACS implementation was not significantly different from before.
Go to :
 XML Download
XML Download