

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Appendectomy for acute appendicitis is one of the most common surgeries in children [12]. It is performed in more than 250,000 cases, and 59,000 cases in patients under 15 years old annually in the United States [3]. One-third of patients with appendicitis are under the age of 19 years [4]. Most of the patients visit the emergency room and are diagnosed by a combination of symptoms, signs, laboratory tests, and imaging studies [567]. Abdominal ultrasonography (USG) is generally preferred as the first diagnostic tool for appendicitis in the pediatric population for the avoidance of radiation exposure [89]. However, recently, low-dose CT has been recognized as a contributive tool in diagnosing appendicitis. It was not inferior to abdominal USG with a lesser radiation dose compared with standard-dose CT in the diagnosis of appendicitis [101112].
Although various studies exploring the effectiveness of radiological methods in diagnosing pediatric appendicitis have been done, their findings were often ambiguous or equivocal [11]. Patients with appendicitis often represent vague symptoms, signs, and laboratory findings that interfere with the clinician’s ability to make a conclusive diagnosis [5]. Though the definition of equivocal appendicitis may vary depending on the study, the prevalence of equivocal appendicitis is generally reported to be 5%–13.1% [13]. Further evaluation and management for equivocal appendicitis also vary widely from study to study. Sim et al. [13] and Jang et al. [14] recommended adding abdominal USG when the CT findings for appendicitis were equivocal because it could reduce the rate of overall negative appendectomy. Cavuşoğlu et al. [15] suggested active observation rather than emergency surgery when the diagnosis of appendicitis is not certain.
In this study, we will investigate the clinical course of equivocal appendicitis, identify the factors associated with the course of appendectomy, and suggest appropriate management of these patients.
Go to : 
METHODS
After the Institutional Review Board of Seoul National University Bundang Hospital (SNUBH) approved the study protocol (No. 1707-043-868), retrospective data analysis was conducted on patients under 19 years of age, who visited SNUBH with clinical symptoms of appendicitis from January 2013 to December 2017. Informed consent was waived due to its retrospective nature.
A total of 1012 patients had appendiceal CT, of which 857 patients were included, excluding the patients with normal findings (88 patients) or other diseases (67 patients). Of these, 143 patients with 2–4 scores were enrolled as the final study population, except for patients with scores of 1 (494 patients) or 5 (220 patients) (Fig. 1).
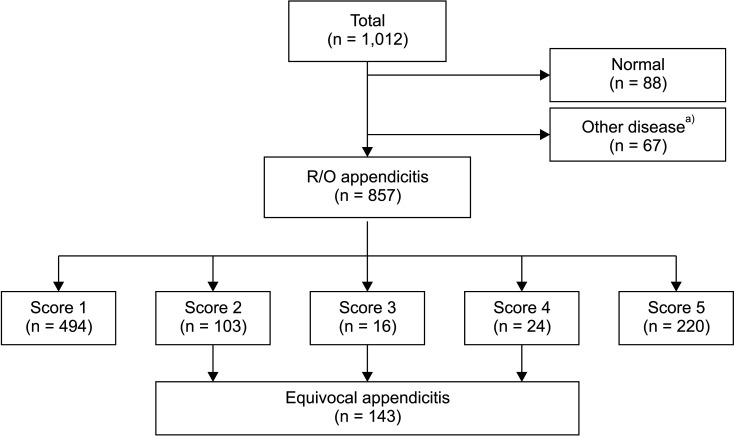 | Fig. 1Patient collection. Patients with appendicitis CT scores of 2 to 4 were enrolled in the study. R/O, rule out. a)Enterocolitis, 24; ovary cyst, 8; urinary abnormality, 6; ileus, 6; diverticulitis, 3; pancreatitis, 2; superior mesenteric artery syndrome, 2; upper gastrointestinal perforation, 2; intussusception, 2; omental infarction, 2; intestinal duplication, 1; hepatitis, 1; pancreatitis, 1; Meckel’s diverticulitis, 1; juvenile polyp, 1; foreign body, 1; solid pseudopapillary tumor, 1; uterine myoma, 1; psoas myositis, 1; empyema, 1.
|
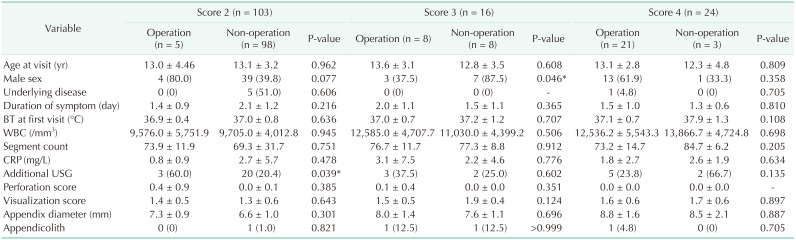
In SNUBH, patients who were suspected to have appendicitis on physical examination and lab results had “appendiceal CT.” If the CT scan findings were ambiguous, an additional abdominal USG test was performed according to the physician’s opinion. The rationale for deciding on applying the USG test is listed in Table 1.
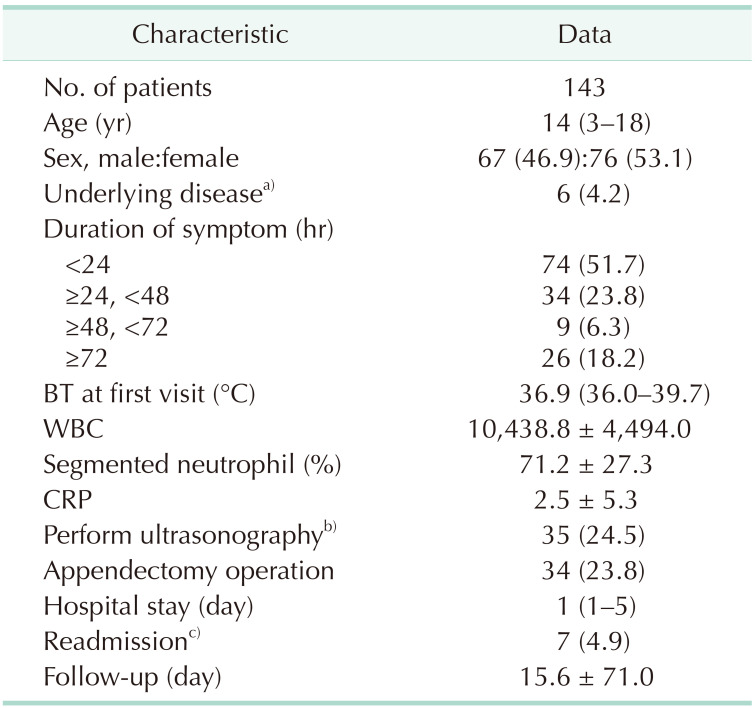
Table 1
Demographics of patients
Values are presented as number only, median (range), number (%), or mean ± standard deviation.
BT, body temperature.
a)Underlying disease: obsessive-compulsive disorder, migraine, autosomal dominant polycystic kidney disease, irritable bowel syndrome, acute lymphoblastic leukemia, and failure to thrive. b)Cause of performing ultrasonography: non-visualization of appendix (n = 17), relapse of abdominal pain (n = 8), clinical suspicion of acute appendicitis (n = 7), recommendation of radiologist (n = 2), and change of tenderness point (n = 1). c)Readmission: for surgery (n = 4) and conservative management (n = 3).
![]()
The appendiceal CT results were classified using the grading system reported by Kim et al. [16]. The grading system scales 1–5 for the probability of appendicitis were 0–2 for appendiceal visualization and 0–1 score for perforation (Fig. 2). The criteria for appendiceal CT scores in the study are as follows. Score 1: Fully or partially visualized normal-looking appendix without dilatation (<6 mm) should be noted without any evidence of phlegmon or abscess. Score 2: No visualization of the appendix without evidence of phlegmon or abscess. Otherwise, mild dilatation of the appendix (6–7 mm) or wall thickening should be present as a secondary change that result from enterocolitis. Score 3: Fully or partially visualized appendix with mild dilatation (6–7 mm) with mural enhancement or wall thickening is present. Score 4: Moderate dilatation (8–10 mm) of the appendix with mural enhancement or wall thickening is present. Otherwise, mild dilatation (6–7 mm) of the appendix with the presence of overt periappendiceal phlegmon (thickness of >2 mm) should be noted. Score 5: Definite dilatation (>10 mm) of the appendix with mural enhancement or wall thickening or moderate dilatation (8–10 mm) of the appendix with overt periappendiceal phlegmon (thickness of >2 mm) is present. Otherwise, a perforated appendix should be identified. We defined equivocal appendicitis as score of 2–4 on the 5-point scale for appendicitis (Fig. 3). The higher the score, the higher the likelihood of radiologic diagnosis of appendicitis.
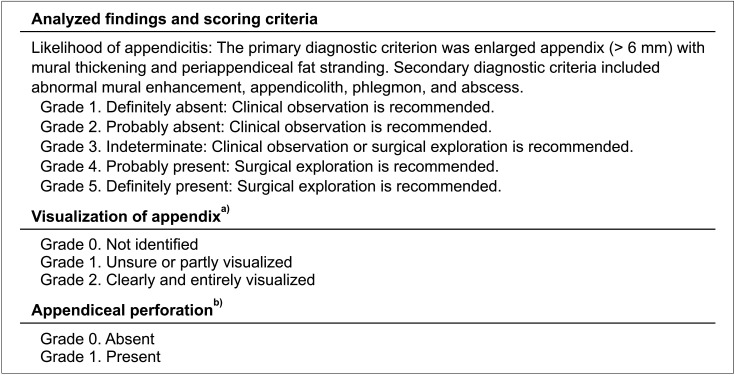 | Fig. 2Appendiceal CT report format. a)In cases with phlegmon or abscess, grade 2 was assigned if there was clear continuity between the lesion and the remaining appendiceal base, indicating that the lesion had originated from the appendix. b)Based on findings of extraluminal gas or appendicolith, periappendiceal fluid or phlegm on, severe periappendiceal fat stranding, and defect in the appendiceal wall.
|

The data collected through the retrospective review of medical records include sex, age, underlying disease, duration of symptom, body temperature at the first visit, WBC count (/mm3), segmented neutrophil percentage (%), CRP (mg/L), abdominal USG test (yes or no), operation (yes or no) for equivocal appendicitis, pathology report, readmission, follow-up period, and duration of hospital stay.
Negative appendectomy is defined as a case in which surgery resulted in normal pathologic report of appendix even when clinical symptoms and radiologic reports indicated appendicitis.
The demographics of the patients and clinical course of patients for each score were analyzed retrospectively with medical records. We investigated the factors associated with surgical intervention of equivocal appendicitis by dividing groups who underwent surgery and those who did not during the follow-up period. The median follow-up period was 15.6 ± 71 days.
Nominal data were compared using the chi-square test and continuous data was compared using the Student t-test. P-values less than 0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
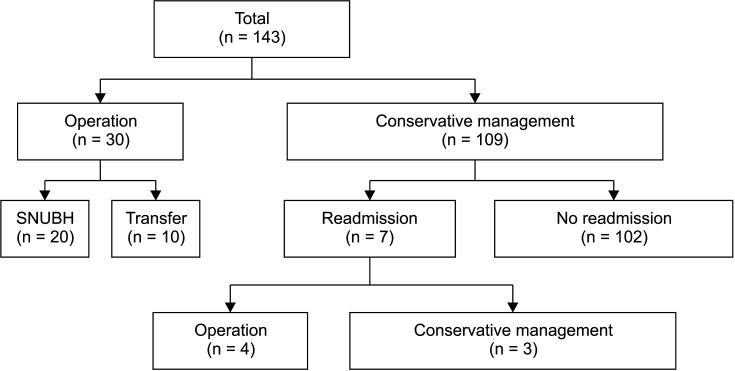
The number of study population who were classified as equivocal appendicitis was 143 of 857 (16.7%) who underwent appendiceal CT. The median age at the first visit was 14 years (range, 3–18 years). The number of male patients was 76 (53.1%). The onset of symptoms was within 24 hours prior to the emergency room visit in 51.7% of all study population. Thirty-four (23.8%) patients underwent appendectomy operation, and, among them, 4 patients underwent surgery at readmission (Table 1, Fig. 4). Out of 30 patients who underwent surgery following the first visit, 20 had an appendectomy at SNUBH. The other 10 had surgery at other hospitals, due to insufficient hospital beds.
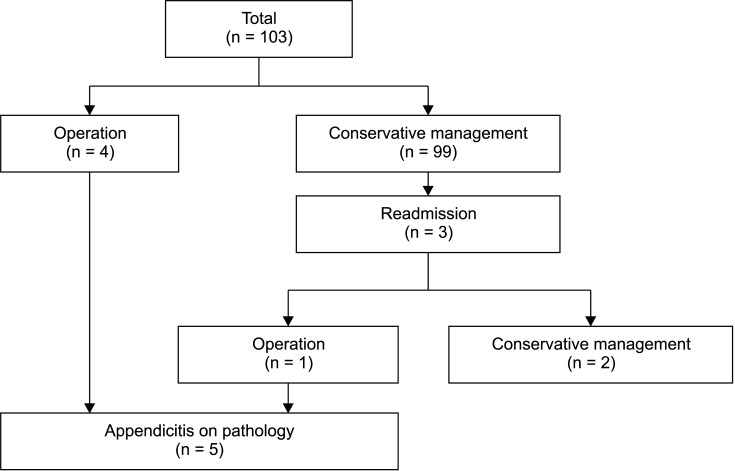
The number of patients who scored 2 in appendiceal CT was 103 of 143 (72.0%), and 5 of them underwent appendectomy. Negative appendectomy was not found among them (Fig. 5). The associated factor of surgical intervention was the complementary abdominal USG test in patients with appendiceal CT score 2 (P = 0.039) (Table 2).
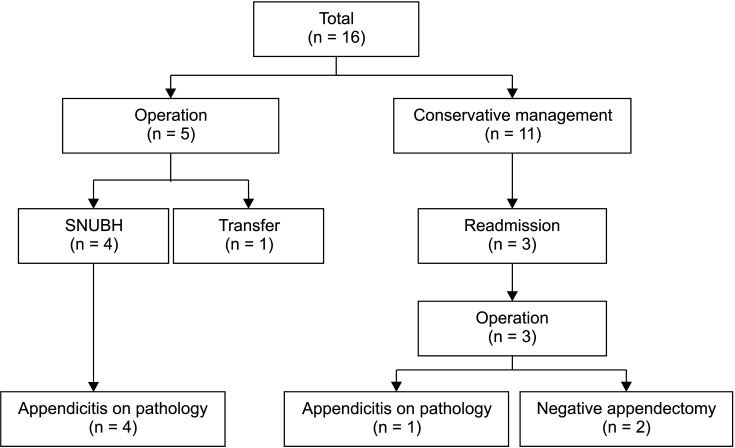
Patients who scored 3 accounted for 16 of 143 (11.2%), and 8 of them underwent appendectomy. Among them, 5 patients underwent appendectomy on their first visit and the other 3 at readmission. The rate of negative appendectomy among the patients who scored 3 on the scale was 28.6% (2 of 7) (Fig. 6). The factor associated with surgery was female sex (P = 0.046) (Table 2).
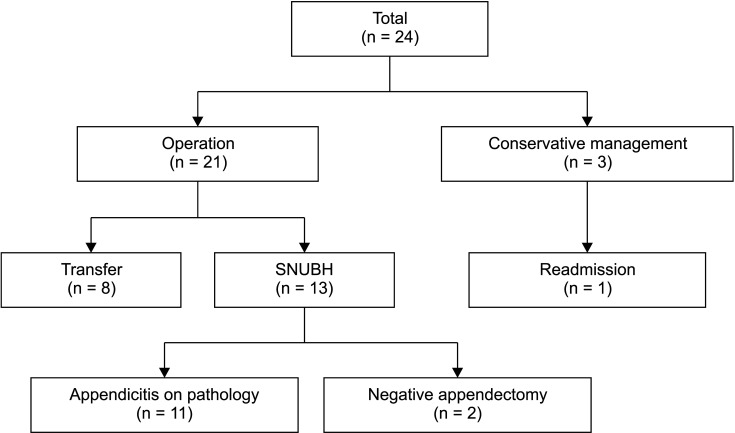
The patients who scored 4 were 24 of 143 (16.8%), and 21 (87.5%) underwent appendectomy. Among them, 15.4% had negative appendectomy (Fig. 7).
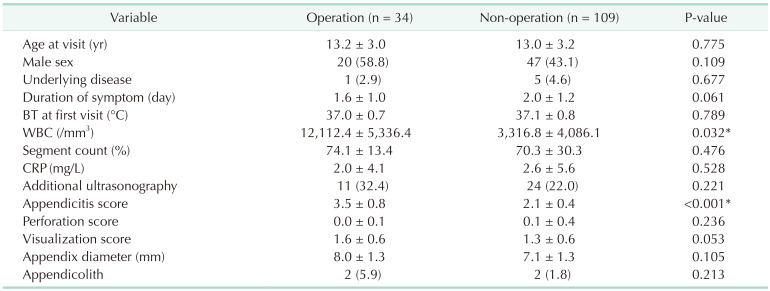
Patients who underwent appendectomy were significantly more likely to have a higher WBC count (12,112.4 ± 5,336.4 mm3
vs. 3,316.8 ± 4,086.1 mm3, P = 0.032), and to have a higher appendicitis score (3.5 ± 0.8 vs. 2.1 ± 0.4, P < 0.001) than those who did not (n = 109) (Table 3).
Go to :
DISCUSSION
In this study, patients with equivocal appendicitis were more likely to have an appendectomy when their appendiceal CT scores were higher. Different treatment modalities are required for equivocal appendicitis depending on the appendiceal CT score. Our findings show that patients with appendicitis CT scores 2 or 3 were more likely to not require appendectomy. However, for those with score 4, appendectomy should be considered as first-line treatment.
The definition and management of equivocal appendicitis have been presented in previous literature. Thompson et al. [1] suggested that when the appendix of the borderline size was 6–7 mm on CT, appendiceal wall thickening, hyperemia, and periappendiceal fat stranding with an absence of intraluminal air may give more weight to the possibility of appendicitis. However, Taylor et al. [17] state that an appendix enlarged exceeding 6 mm in diameter or minimal fat stranding is not a sufficient sign for the diagnosis of appendicitis. Although the diameter of appendix did not show a significant relation with appendectomy (yes or no) in our study, the mean appendiceal diameter of total appendectomy patients was larger than non-operational treatment patients (8.0 mm vs. 7.1 mm). In a single-centered study in Korea, setting the definition of enlarged diameter of appendix at 8 mm improved the accuracy of diagnosis [18]. Combining previous studies, one can conjecture that an enlarged appendix diameter may indicate appendicitis, but it is not completely reliable.
Keating et al. [19] noted that in children with suspected appendicitis for whom CT scan results were equivocal, abdominal USG provided a definitive diagnosis in almost 90% of cases. In this study, 35 of 143 patients (24.5%) underwent additional USG examination after CT scan. The reason for performing additional USG includes non-visualization of the appendix (n = 17), relapse of abdominal pain (n = 8), clinical suspicion of acute appendicitis (n = 7), recommendation of a radiologist (n = 2), and change of tenderness point (n = 1). Among them, patients with appendiceal CT score 2 who were selected for further abdominal USG were significantly more likely to undergo surgery. Therefore, it is presumed that USG was suitable in deciding whether to perform the surgery. Moreover, negative appendectomy rate was lowest of all score groups. Although this tendency was only observed in the score 2 group, it is encouraged to perform USG in patients with vague diagnostic yields in CT as in previous literature [7].
Half of the study population with an appendiceal CT score of 3 underwent surgery. Although abdominal USG was applied at the highest rate among all groups, score 3 group had the highest rate of negative appendectomy (28.6%). A possible hypothesis is that with a higher appendiceal CT score, surgeons might have chosen to operate rather than actively observe the patients because appendectomy for uncomplicated appendicitis is a relatively safe treatment option. Moreover, in a retrospective study with a study population of 192 in Korea, those who had surgical intervention 36 hours after the onset of symptoms due to appendicitis were significantly more likely to experience postoperative complications than those who had an earlier appendectomy [20]. Furthermore, in a systematic review with meta-analysis of 5 randomized controlled trials including 1,351 adult patients, those who underwent appendectomy showed higher treatment efficacy (98% vs. 76%) compared to those who were only treated with antibiotic therapy alone at 1-year follow-up [21]. However, Cavuşoğlu et al. [15] compared the patients who underwent surgery immediately after a definite diagnosis of appendicitis and those who underwent surgery after 1 to 2 days of observation with equivocal imaging findings and clinical symptoms. They found that the duration of symptoms, postoperative complications, and negative appendectomy rate were similar except for the length of hospital stay. In our study, the real need for appendectomy in the score 3 group was 6 of 16 patients or less. Considering the cost of medical resources and unnecessary exposure to surgical complications for patients with non-appendicitis, careful surveillance along with nonsurgical management may be a feasible treatment option in the score 3 group. However, in respect to the large heterogeneity of equivocal appendicitis cases in real clinical practice, the attending surgeon should decide whether to operate or not.
Among the patients who scored 4, 87.5% underwent surgical treatment. Interestingly, in the score 2 and 3 groups, the rate of abdominal USG examination was higher among those who underwent surgery; whereas in the score 4 group, the rate of abdominal USG examination was higher among those who did not undergo surgery. It is presumed that additional abdominal USG test was performed to rule out negative appendectomy in score group 4. We assumed that abdominal USG would have been performed in score group 4 if the clinical results did not correlate with the appendiceal CT exam results. Further analysis is warranted that could reveal the rationale of this hypothesis.
Subsequently, among patients with appendiceal CT score of 2 to 4, higher appendicitis score and a higher level of WBC count was significantly associated with surgical treatment. This can provide grounds to assert the benefit of appendiceal CT in diagnosis of appendicitis. There are some limitations to this study. First, this is a retrospective study, which depends on past medical records. Second, the total number of negative appendectomies could not be collected because the postoperative pathology results cannot be confirmed in patients who have been transferred to other hospitals for surgery. However, since the transfer was not selective, random extraction of samples might have a limited impact on statistics. Third, the mean difference in thickness of the appendix according to age could not be considered in this study due to the small-scale sample study. Additional data analysis with stratification of age is warranted with a larger sample size in further study design. Finally, since the study classified the patients solely by appendiceal CT score, it is not possible to confirm the effect of other clinical symptoms and signs on the patient's treatment decision. Further study design should take them into account because diagnostic methods such as abdominal USG were used for certain patients in the same score group. Analysis of conditions that influenced the modality of diagnosis and treatment is warranted.
In conclusion, the incidence of equivocal appendicitis was 16.7% when the CT scoring system was used. The probability of surgery was higher in the patients with higher appendicitis scores and higher level of WBC. Careful observation can be a valid treatment method in groups with appendicitis scores 2 or 3. However, surgical intervention should be the first line of treatment for patients with appendicitis score 4. Additional abdominal USG test is advisable for determining treatment modality with equivocal appendicitis in children.
Go to :
 XML Download
XML Download