

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The International Agency for Research on Cancer reported a total of 19,292,789 cancer cases worldwide in the year 2020. Of these, 2,261,419 (11.7%) were breast cancer cases, making it the most common cancer. Breast cancer was also the most common cancer among women in 2020, accounting for 24.5% of cases [1]. In Korea, there have been 28,032 new female breast cancer cases reported so far in 2022, and 2,890 deaths are expected to occur this year [2]. The 5-year relative survival rate was 93.3% from 2015 to 2019 [3]. In-depth study and research have increased survival over the last decade due to advances that promote screening, early diagnosis, treatment, and surveillance.
Adjuvant chemotherapy (CTx) and/or hormonal treatment (HT) are standard practices to reduce the risk of relapse according to histological, pathological, and immunohistochemical staining characteristics of the tumor following surgical treatment [45]. Adjuvant HT is routine in hormone receptor-positive breast cancer, which has the best prognosis among the subtypes. While the National Comprehensive Cancer Network suggests CTx in select high-risk patients, several studies have shown that some of these women do not need such adjuvant CTx. The side effects and toxicities of CTx have made it less favorable as routine treatment for breast cancer patients.
The current approach to breast cancer has been tailored according to individual risk of relapse and predicted sensitivity to a particular treatment (e.g., estrogen receptor [ER], progesterone receptor [PR], and human epidermal receptor-2 [HER2] status). With the advent of gene profiling, personalized treatment was refined, and is now more accurate than clinicopathologic factors in predicting the risk of distant recurrence following surgery [6789]. Given these data, this study aims to evaluate the trends and practice patterns in treatment of breast cancer in hormone receptor-positive and HER2-negative patients with limited nodal disease in Korea over time and to verify whether adjuvant CTx and HT differ in terms of overall survival (OS).
METHODS
The protocol of this study was approved by the Institutional Review Board of Korea University Anam Hospital (No. 2019AN 0062). This study was performed in accordance with the Declaration of Helsinki and written informed consent was waived due to its retrospective nature.
Korean Breast Cancer Society Registry
The Korean Breast Cancer Society (KBCS) established a registration system in 1996. Since 2001, the KBCS has maintained an online registration system to collect and distribute nationwide breast cancer information. These data include not only physical parameters of breast cancer patients, such as sex, age, height, and weight, but also other valuable data for breast cancer research, such as molecular subtype, stage, and type of surgical procedure [10]. This study analyzed the characteristics of breast cancer in Korea using the data registered by the KBCS and Korea Central Cancer Registry (KCCR) in 2017 and investigated breast cancer treatment over the prior 17 years.
Patients
Inclusion criteria for this study were women entered into the database from January 1, 2000 to December 31, 2018 with newly diagnosed hormone receptor (ER/PR)-positive and HER2-negative invasive breast cancer that was nonmetastatic (pT1-2N0-1) and who were treated with mastectomy or breast conservation surgery with radiation therapy along with adjuvant HT and/or CTx. The Ki-67 level was not considered due to the lack of reported data. Patients with unknown histologic grades and incomplete personal data were excluded.
Statistical methods
OS was based on the operative date and the date of death or the date of the last follow-up from the data of the KBCS and KCCR. Cox regression was used for both univariate and multivariate analyses. Differences were considered significant at P < 0.05. IBM SPSS Statistics ver. 25 (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
RESULTS
A total of 40,938 patients from a pool of 75,730 patients in the KBCS Registry were included in the study (Fig. 1). There were 20,880 in the CTx + HT group (51.0%) and 20,058 in the HT-alone group (49.0%). The mean age was 50.49 years, and the median follow-up time was 65 months.
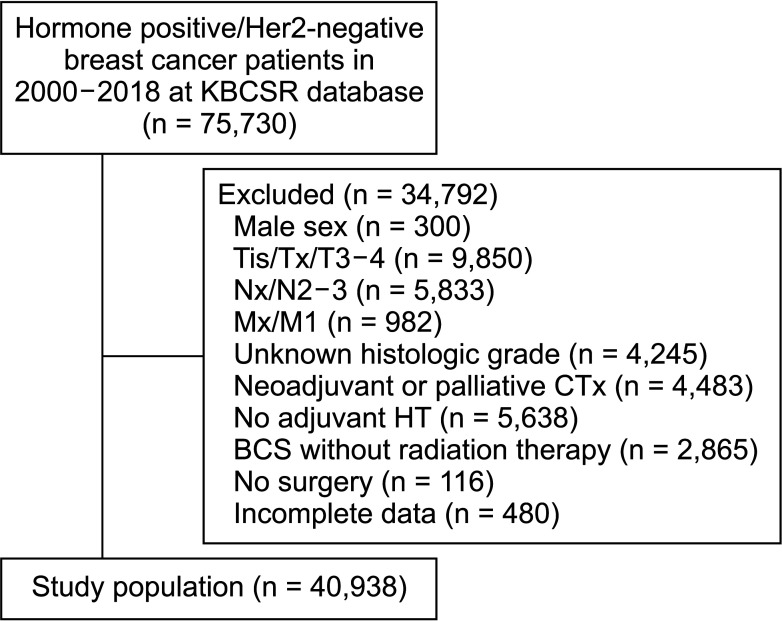
Fig. 1
Study flow diagram. HER2, human epidermal receptor-2; KBCSR, Korea Breast Cancer Society Registry; T, primary tumor stage; Tis, T stage in situ; Tx, T stage not determined; N, regional lymph node stage; Nx, N stage not determined; M, distant metastasis stage; Mx, M stage not determined; CTx, chemotherapy; BCS, breast-conserving surgery.
![]()
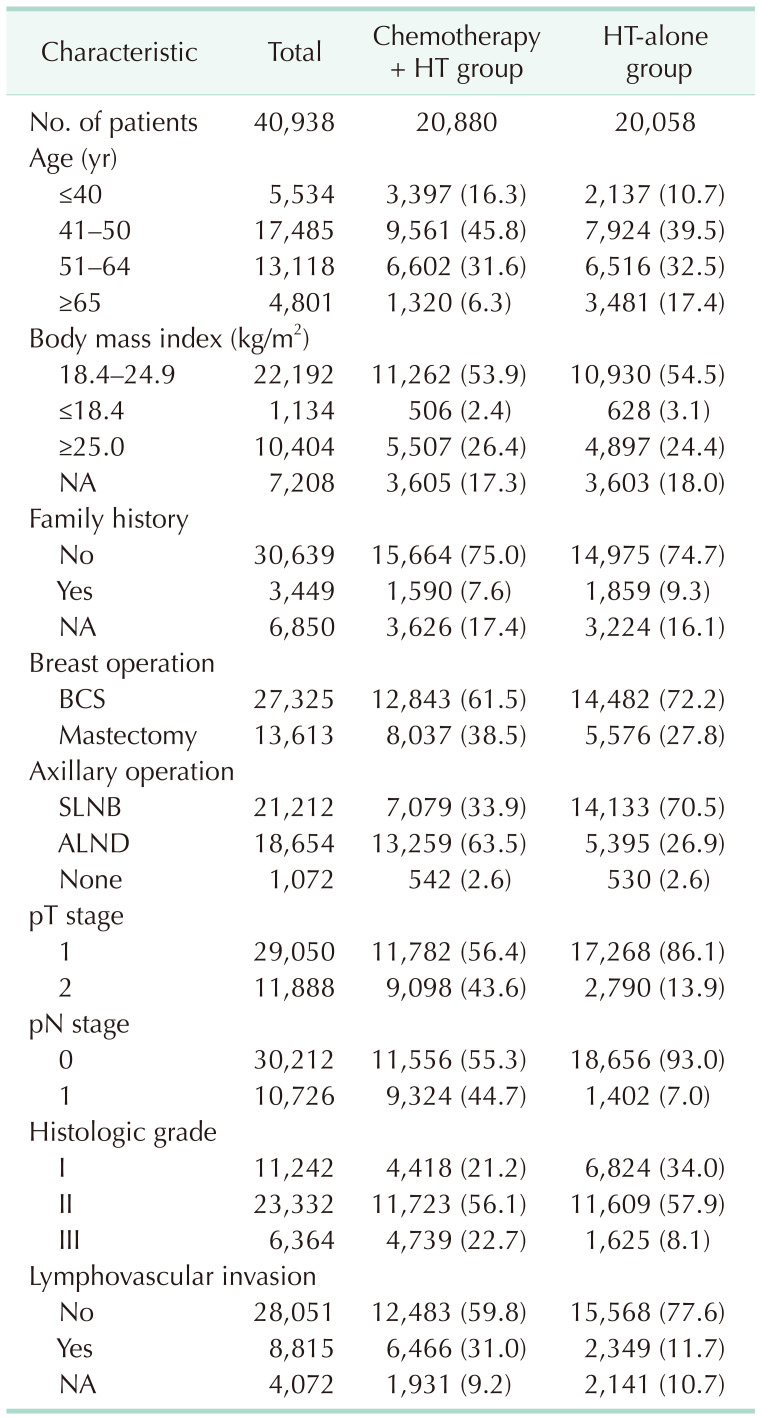
In the CTx + HT group, most of the patients (45.8%) were 40 to 50 years old. The majority had a normal body mass index (BMI) (65.2%) and no family history of breast cancer (90.8%). Large proportions of women in this group underwent breast-conserving surgery (BCS) (61.5%) or axillary lymph node dissection (63.5%) and had a pT1 tumor stage (56.4%), pN0 stage (57.53%), and histologic grade of II (56.1%) with no lymphovascular invasion (LVI) (65.9%).
In the HT-alone group, the largest proportion of women was 40–50 years old (39.5%). The majority also had a BMI within the normal range (66.4%), had no family history of breast cancer (89%), and underwent BCS (72.2%) with sentinel lymph node biopsy (SLNB) (70.5%). On histopathology, most had pT1 (86.1%) or pN0 stage (93.0%) with a histologic grade of II (57.9%) and no LVI (86.9%) (Table 1).
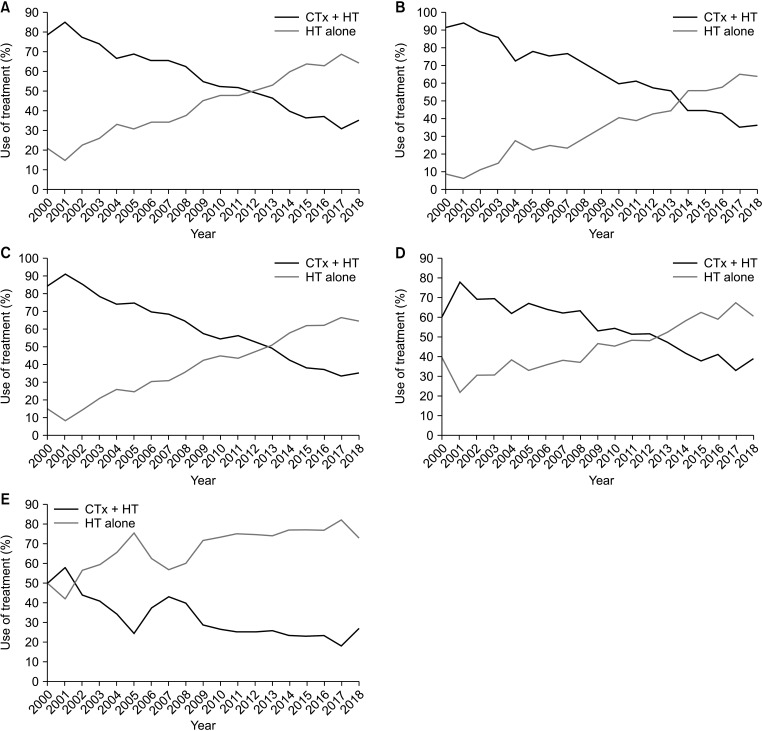
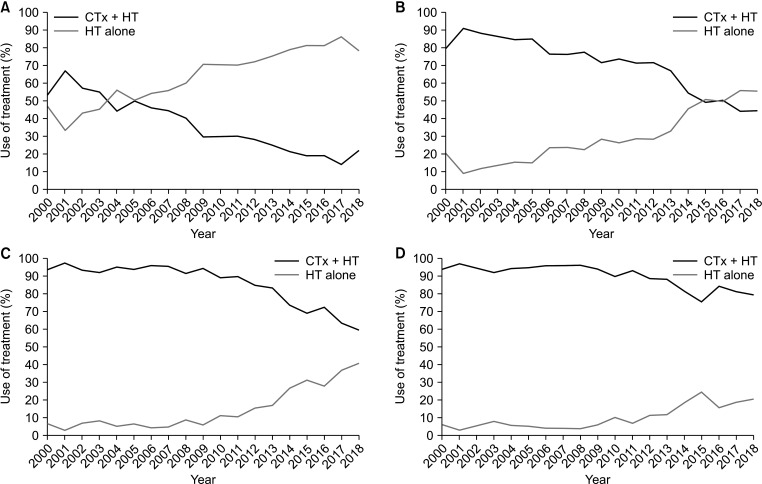
Over time, the number of patients who underwent CTx + HT decreased, and the number who underwent HT alone increased (Supplementary Table 1). Fig. 2 shows the trends of CTx + HT and HT alone over the past 18 years. Omission of CTx steadily increased from 21.0% (2000) to 64.6% (2018) and was evident in all age groups. For the whole cohort, HT-alone treatment for breast cancer surpassed CTx + HT multimodality treatment after 2011, and there was a similar crossover for all age groups. Although, there was no crossover in the node-positive group, patients who underwent CTx steadily decreased over time. Fig. 3 shows the change in treatment over time according to tumor size and nodal status.
In a univariate analysis for OS, survival decreased as age increased, except for women aged 51–64 years (P = 0.639). Women who had high BMI and had undergone mastectomy and axillary lymph node dissection showed poorer prognosis compared to women who had normal BMI and had undergone BCS and SLNB. Higher T and N stages, poor histologic grades, and LVI were associated with poor OS (Table 2).
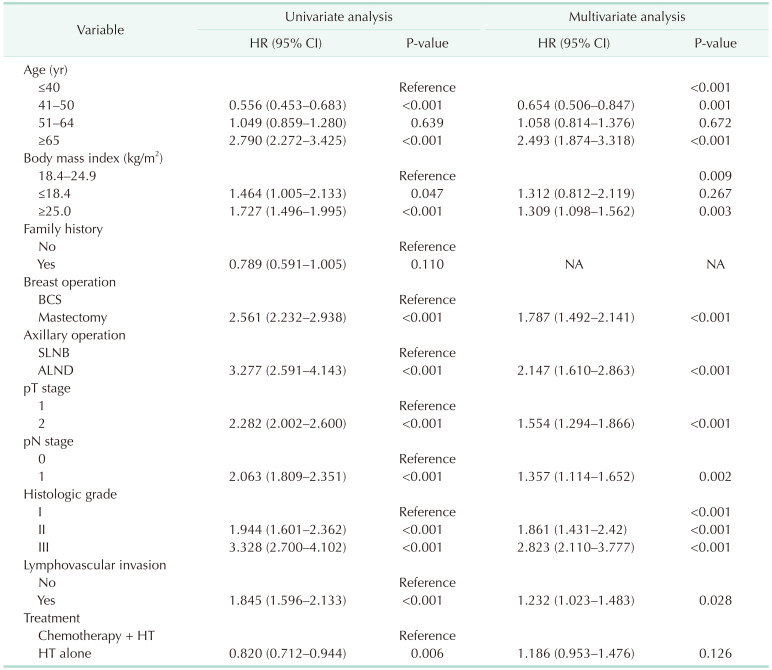
In multivariate analysis adjusted for breast operation, axillary operation, T stage, N stage, BMI, family history of cancer, histologic grade, LVI, and treatment, we found that women 65 years and older who underwent mastectomy, and who had a higher T stage, N stage, and BMI with poor histologic grade and LVI showed a poorer prognosis (Table 2, Fig. 4).
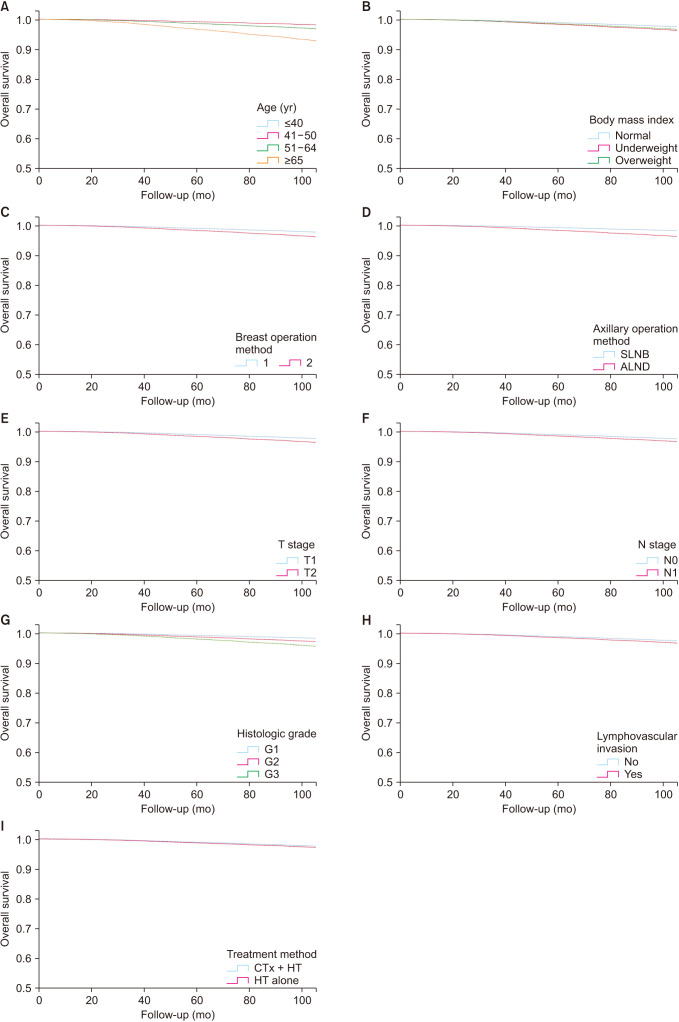
Fig. 4
Overall survival graphs by multivariate analysis using Cox regression analysis. (A) By age (P < 0.05). (B) By body mass index (P < 0.05). (C) By breast operation methods (P < 0.05). (D) By axillary operation method (P < 0.05). (E) By T stage (P < 0.05). (F) By N stage (P < 0.05). (G) By histologic grade (P < 0.05). (H) By presence of Lymphovascular invasion (P < 0.05). (I) By treatment methods (P = 0.130).
![]()
The adjuvant treatment method showed a difference in OS, with the HT-alone group having a hazard ratio (HR) of 0.820 (95% confidence interval [CI], 0.712–0.944) in the univariate analysis. However, after adjusting for other factors in multivariate analysis, there was no difference in OS (95% CI, 0.953–1.476; P = 0.126). As patient groups had a wide range of follow-up periods, we divided and analyzed OS into 3 groups: before crossover (2000–2010), during crossover (2011–2012), and after crossover (2013–2018). There were no significant differences between these 3 groups (2000–2010: HR of 1.22 [95% CI, 0.97–1.54], P = 0.080; 2011–2012: HR of 0.98 [95% CI, 0.40–2.33], P = 0.950; 2013–2018: HR of 0.39 [95% CI, 0.05–3.11], P = 0.380).
DISCUSSION
This study of Korean patterns of breast cancer treatment evaluated the trends of adjuvant HT or CTx + HT for the past 18 years in low-burden, hormone receptor-positive, and HER2-negative invasive breast cancer in women. This particular group is inclined to overtreatment with CTx, with the risks outweighing the benefits of such adjuvant therapy.
Currently, selection of adjuvant systemic treatment in patients with primary breast cancer depends on genomic cancer subtype as well as clinical parameters such as grade, tumor size, and nodal status [11]. In the last decade, use of adjuvant CTx in general has become more popular as a more specific and precise application based on tumor biology. It is well accepted that luminal B, HER2-positive, as well as triple negative or HER2-overexpressing breast cancer patients should undergo (neo-)adjuvant CTx. In addition, there is consensus that nodal negative luminal A (hormone receptor-positive, HER2-negative, and low Ki-67) cancer patients only need adjuvant endocrine therapy. Although there have been several reports about the CTx benefit in node-positive luminal A cancer [12], we studied the change in treatment pattern and survival benefit for a large cohort of patients over 18 years in Korea. Although we could not conduct a subgroup survival analysis for node-positive patients because of the small number of patients and short follow-up times, the number of node-positive patients who underwent CTx also decreased with time.
The results of this paper demonstrate that omission of CTx is increasing over time, with a shift to HT alone. This pattern was seen in all age groups. Although CTx + HT demonstrated an advantage over HT in univariate analysis, in multivariate analysis adjusted for age, breast and axillary operation, tumor and nodal stages, and BMI, this treatment showed no difference in OS from those who received HT alone. Because CTx targets fast-dividing cells, luminal A tumors, which have low proliferation indices, are less appropriate for CTx.
A study by Haque et al. [13] showed the same results. Their study on low-grade, luminal A, N1 breast cancer demonstrated a steady decline in CTx use, primarily in older patients and at academic centers. Although CTx is associated with an OS advantage in all age groups, their subgroup analysis revealed no OS benefit in women >50 years old. While their study data were collected from the United States National Cancer Database in over 10 years (2004–2014) with a population of 8,548 cases, the current study focused on cases from the Korean national database from 2000 to 2018 with a larger study population (40,938 cases). Another similar study using data from the Korean national database was that of Kim et al. [14] which only included 3,076 cases of mucinous breast cancer from 1990 to 2016. This study also showed no survival benefit of adjuvant CTx on most ER+ mucinous breast cancer, regardless of axillary lymph node metastasis.
The elderly population in the present study had the highest risk for mortality compared to its younger counterparts and showed a significantly superior prognosis for CTx + HT rather than HT alone. Breast cancer in elderly women is postulated to have a less aggressive biology than that in younger patients, as indicated by a higher rate of hormone-receptor-positive tumors, lower grade, and lower proliferation rate [15]. On the other hand, tumor stage at primary diagnosis in the elderly is commonly more advanced [16], probably because of nonparticipation in physical exams and screening strategies. Although the elderly population has the best response to CTx + HT, this particular group poses a major challenge for treatment as there are several age-specific factors that need to be considered during decision making. Comorbid states and compliance should be major considerations for decision making, and these factors could have introduced bias into the survival analysis. On the other hand, mortality could be due to non-breast cancer-related causes, which is very likely in this age group. Therefore, patients in this treatment arm should be healthy and able to tolerate the prescribed regimen.
We found that the types of breast and axillary surgery were also significant factors for OS. Mastectomy has a 1.79-fold higher risk compared to BCS on multivariate analysis. Although the current standard of treatment for early breast cancer is BCS, recent studies have shown an increasing number of patients receiving mastectomy who are otherwise amenable to conservation. One likely contributing factor is the perceived worse outcomes if BCS was to be offered in “high-risk” groups (e.g., young age, ER-negative disease, HER2-positive disease) [17]. Hwang et al. [18] further explained that there may have been confounding immeasurable patient and tumor characteristics not reported in the registry that influenced the recommendation for mastectomy over BCS. SLNB had a better prognosis than axillary lymph node dissection as this approach correlates with a lower nodal stage. Axillary lymph node dissection is performed when axillary lymph node metastasis is confirmed via SLNB.
Both high histologic grade and presence of LVI were independent significant predictors for poor OS. Assessment of histologic grade, a composite of tubular differentiation, nuclear features, and mitotic activity, is important in evaluation of breast cancers and is a required parameter in pathologic reporting of breast cancers. It is generally assumed that histologic tumor grade plays an important prognostic role in early-stage cancers with no or few metastatically involved axillary nodes. Presence of LVI in a primary tumor has been used as an indication of the ability of the tumor to metastasize outside the breast and was recognized to impact the treatment plan according to the 2005 St. Gallen consensus meeting [19]. The presence of LVI is correlated with lymph node involvement, local recurrence, and poor survival in breast cancer, and 20% of patients with node-negative breast cancer will experience recurrence and die of systemic disease [20212223].
BMI is expected to have an adverse effect on OS. In our study, a high BMI showed an HR of 1.3. Berclaz et al. [24] reported that being obese or overweight is associated with a poor prognosis after breast cancer treatment, and other studies have suggested that obesity at the time of cancer diagnosis or prediagnosis is associated with poor prognosis for breast cancer patients [2526]. In postmenopausal patients with higher BMI, increased synthesis of peripheral estrogen in adipose tissue and reduced sex hormone binding globulin might be responsible for the poor breast cancer prognosis due to enhanced aromatase activity, which may induce and stimulate the growth of abnormal mammary cells [2728].
There are several limitations to this study. The KBCS Registry has recorded data since the year 2000, though its retrospective nature results in a number of unknown details such as contraceptive use, history of breastfeeding, and Ki-67, especially in the early years of the registry. This study did not consider the type of invasive breast cancer (ductal, lobular, etc.) or the type of CTx administered. These missing data may have affected the results. Also, there was a wide range of follow-up times, which could have introduced bias into the survival analysis for different time periods. We divided the patients into 3 groups: before, during, and after crossover (2011–2012). There were no statistically significant differences. The main purpose of this study was to observe trends in the treatment pattern and survival for a large cohort registry over a long time period. We did not match patients into groups based on characteristics such as propensity score. Nevertheless, a treatment trend was observed over the years, and OS was analyzed using a large national cohort data set.
In conclusion, for a selected group of women with hormone receptor-positive and HER2-negative early breast cancer and low disease burden, adjuvant CTx may not be needed, and HT alone can, even in T2N1, achieve the same OS. Given the toxicity profile of systemic CTx, shared decision making between the physician and patient is needed to individualize treatment options.
 XML Download
XML Download