

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Postoperative problems including dysfunction of the sphincter or bowel in patients with rectal cancer have been a challenging issue for patients and clinicians, especially in older patients or those with underlying disease [12]. Patients with rectal cancer who undergo surgery are susceptible to morbidity [34]. In addition, patients have the fear that the anus would disappear and that they experience discomfort from an ostomy or sphincter dysfunction [56], which may contribute to resistance to rectal cancer surgery. Therefore, organ-preserving treatment strategies have been considered by colorectal surgeons [78]. Recently, interest in preserving the sphincter has increased, and greater efforts have been undertaken to maintain the rectum. Many studies concerning the preservation of “quality of life” without diminishing oncologic outcomes have been published [910].
Therefore, the application of neoadjuvant chemoradiotherapy (nCRT) has been gradually expanded with the assumption that it can improve sphincter preservation and local control in rectal cancer patients [11]. Moreover, a number of studies indicate that total neoadjuvant therapy (TNT), which tended to limit early distant metastasis, had a good influence on the local tumor response. Due to the fact that the clinical good responder rate rose in the setting of TNT without altering oncologic outcomes, the “watch-and-wait (WW)” strategy is considered more frequently with TNT, resulting in a longer preoperative treatment period [1213].
Although interest in the WW strategy has increased, it is difficult to select who to apply it to in actual clinical practice because of the lack of data and the limited accuracy of clinical response evaluation. Many studies have applied WW to patients with clinical complete responses (cCR). WW was not inferior to radical resection (RR) in terms of overall survival (OS) and recurrence-free survival (RFS) in patients with cCR following nCRT [1415]. However, the accuracy of tumor response evaluation was limited for practical application [16]. There is interobserver variability due to the varied diagnostic methods and criteria for the diagnosis of cCR. In addition, because the response improves as time passes after the completion of therapy, the appraisal of the response may differ based on the evaluation period [17]. In addition, the number of patients diagnosed with cCR was quite low. Rather than cCR, therefore, WW is explored for patients with substantial tumor response.
Therefore, we evaluated oncologic outcomes for WW in good responders after nCRT who were diagnosed as ycT2 or lower, with MRI, and compared those after RR. Additionally, we employed propensity score matching (PSM) analysis to eliminate the inherent bias in the selection of patients for each treatment. To apply the WW strategy to clinical reality, it was important to study ≤ycT2, as a good responder. Therefore, we evaluated the difference in oncologic outcomes between patients with WW and RR.
Go to : 
METHODS
Patients population
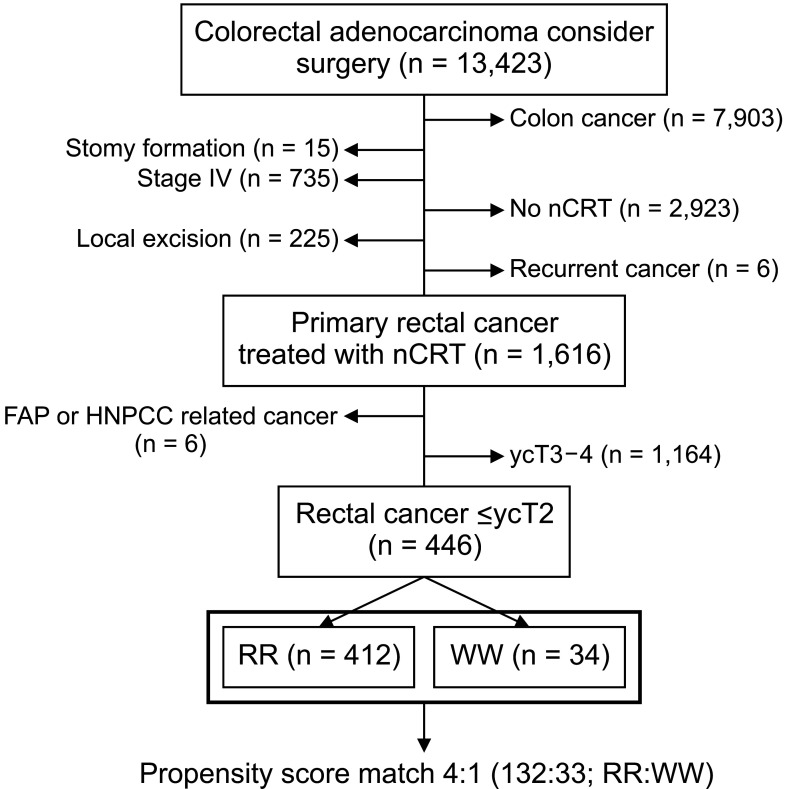
We enrolled nonmetastatic patients diagnosed as ≤ycT2 after nCRT in Asan Medical Center between 2008 and 2016. Following nCRT, 412 patients were treated with RR, while 34 patients were treated with the WW strategy; 446 patients were ultimately enrolled in this study.
Patients who were lost to follow up had only colon cancer, stomy formation, distant metastasis, recurred cancer, had undergone local excision, or had not received nCRT were excluded. In addition, patients with familial adenomatous polyposis or hereditary nonpolyposis colon cancer and ycT3–4 stage were excluded from the study (Fig. 1).
Medical records including patients’ sex, age, clinical stage, pathological stage, and treatment strategy were obtained. The protocol for this retrospective study was approved by the Institutional Review Board of the Asan Medical Center and the requirement for informed consent was waived (No. 2017-0955).
Response evaluation, treatment, and surveillance
All patients received nCRT. A dose of 45–50.4 Gy of radiation therapy was administered in 25–28 fractions to a target volume comprising the primary tumor, the perirectal adipose tissue, the lateral pelvis, and the presacral lymph node.
At 4–6 weeks after nCRT completion, all patients underwent physical examination, rectal MRI, abdominopelvic CT, chest CT, and sigmoidoscopy. Tumor response was evaluated with rectal MRI. Two experienced radiologists with a minimum of 5 years of training in abdominal imaging determined the ycT/ycN stage following nCRT.
WW strategies were carefully considered for patients with ≤ycT2 and no evidence of radiologic lymph node metastasis or distant metastasis because it is not a standard treatment yet. Considering the patient’s medical condition, age, and socioeconomic circumstances, a multidisciplinary team decided on the WW strategy after a discussion among the physicians and patients. The patient’s desire for surgical intervention was also crucial. Additionally, medical conditions such as underlying disease, exercise level, and patient’s age were taken into account. The mental health of the patient was also considered.
RR was done 6 to 8 weeks following the completion of nCRT. Pathologic evaluation was conducted by pathologists with expertise in colorectal cancer pathology. All medically fit patients treated with nCRT were recommended adjuvant chemotherapy. The standard adjuvant regimen consisted of 4 cycles of 5-fluorouracil and leucovorin monthly or 6 cycles of capecitabine. Patients were also treated with oxaliplatin at the discretion of the attending physician.
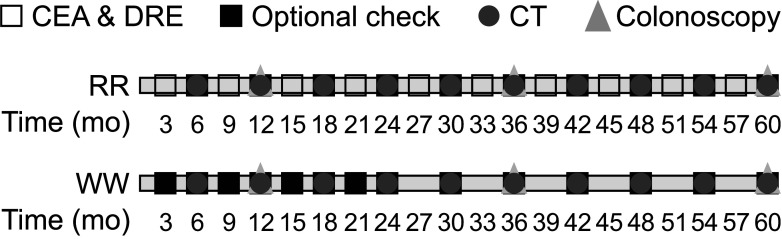
Patients who got RR had a physical examination and CEA tests every 3–6 months. Abdominopelvic and chest CT scans were performed every 6–12 months. A colonoscopy was performed every 2–3 years. After 3–6 months postoperatively, a colonoscopy was done on patients with preoperative obstruction who could not be examined throughout the entire colon. For patients managed by WW, digital rectal examination, sigmoidoscopy, CEA measurement (every 3 months during the first 2 years and then every 6 months), CT scan of the chest, abdomen, and pelvis (every 6 months for 5 years), and colonoscopy (every 2–3 years) were performed after the initial post-nCRT assessment (Fig. 2).
Clinical, endoscopic, or radiologic evidence of intraluminal tumor was defined as local regrowth. Local recurrence was defined as the existence of a tumor in the rectal wall or mesorectum following resection. A distant metastasis is the recurrence outside the pelvis.
Statistical analysis
Clinicopathologic characteristics were compared between groups on variable type using the chi-square test, Fisher actual test, and independent-sample t-test. RFS was measured from the date of surgery or decision to implement the WW plan to the date of the first recurrence. OS was calculated from the date of diagnosis till death (all-cause mortality) or the last day of follow-up. Local RFS (LRFS) was measured from the date of diagnosis to the date of local recurrence or regrowth. Distant metastasis-free survival (DMFS) was defined as the interval between the date of surgery or WW treatment decision and the date of radiological or pathological identification of distant metastasis.
The primary endpoints for this study were 5-year RFS and OS. The secondary endpoints were 5-year LRFS and DMFS.
In addition, we matched patients based on propensity score with sex, age, initial clinical stage, ycT stage, and interval from rectal MRI for response evaluation from the completion of nCRT. In the 1:4 matched cohort, 33 patients in the WW group and 132 patients in the RR group were included.
Using the Cox proportional hazards model, univariate and multivariate survival analyses were done to examine hazard ratios, from which the 95% confidence intervals (CIs) were derived. All assessments were conducted using a 2-sided test; the P-value of <0.05 was considered statistically significant. All statistical analyses were conducted using R software ver. 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria).
Go to :
RESULTS
Clinicopathological characteristics of patients with pT3N0 colorectal cancer
A total of 446 patients were included in this study. After nCRT, 412 patients (92.4%) were treated with RR and 34 patients (7.6%) underwent the WW strategy.
In the WW group, 5 patients refused surgical interventions due to their circumstances such as religion or socioeconomics. And other 29 patients were included in the WW group because of their medical conditions about old age, previous laparotomy history, and underlying diseases such as diabetes mellitus and cerebrovascular disease.
Median follow-up was 61.1 months (interquartile range, 54.7–69.8 months). There were no differences regarding sex, CEA, and N stage at diagnosis between groups (Table 1). Patients in the WW group were older, and the interval between the last nCRT and MRI evaluation date was longer. Patients with RR had a considerably advanced pre-nCRT cT/cN stage. The RR group had more ycT2 stage (P < 0.001) after nCRT. There are 236 patients with <ycT2 stage, of which 73 (30.9%) were diagnosed as having a cCR. Thirteen patients with cCR were treated with the WW strategy, while 60 patients received RR. The status of sphincter preservation was examined on the final day of follow-up. In the RR group, 334 patients had their sphincters preserved. Thirty patients in the WW group had sphincter preservation. There was no significant difference between these groups in sphincter preservation status (P = 0.365).
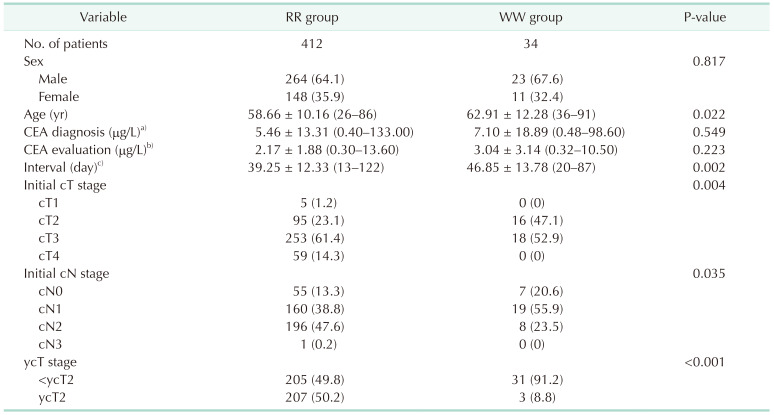
Table 1
The clinicopathological characteristics of patients with ≤ycT2 rectal cancer after nCRT
Values are presented as number only, number (%), or mean ± standard deviation (range).
nCRT, neoadjuvant chemoradiotherapy; RR, radical resection; WW, watch-and-wait.
a)CEA evaluated at diagnosed date (155 in the RR group and 34 in the WW group were evaluated); b)CEA evaluated at MRI evaluation date after nCRT (154 in the RR group and 8 in the WW group were evaluated); c)days of evaluation clinical tumor response with MRI from completion of nCRT (161 in the RR group, 33 in the WW group were evaluated).
![]()
Oncologic outcomes between treatment strategies
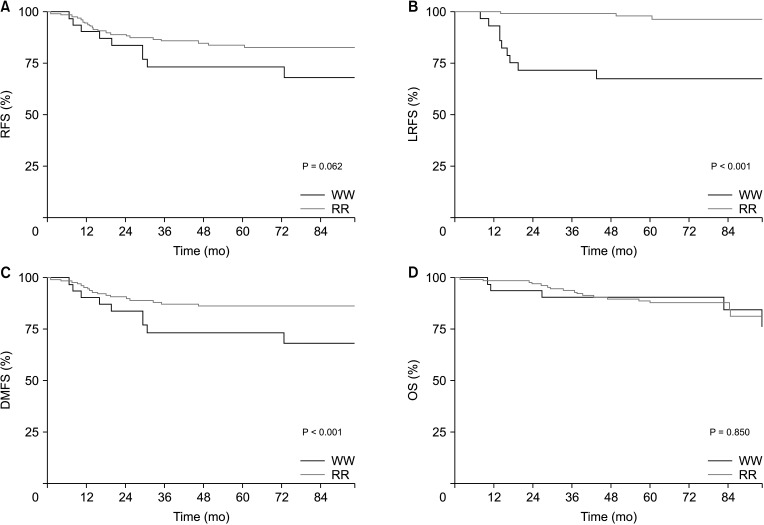
The 5-year RFS (74.1% vs. 79.5%) (Fig. 3A), DMFS (74.1% vs.. 81.6%) (Fig. 3C), and OS (90.4% vs. 87.7%) (Fig. 3D) were not statistically different between the WW and RR groups. However, the LRFS (65.1% vs. 97.0%) was statistically different in those groups (Fig. 3B).
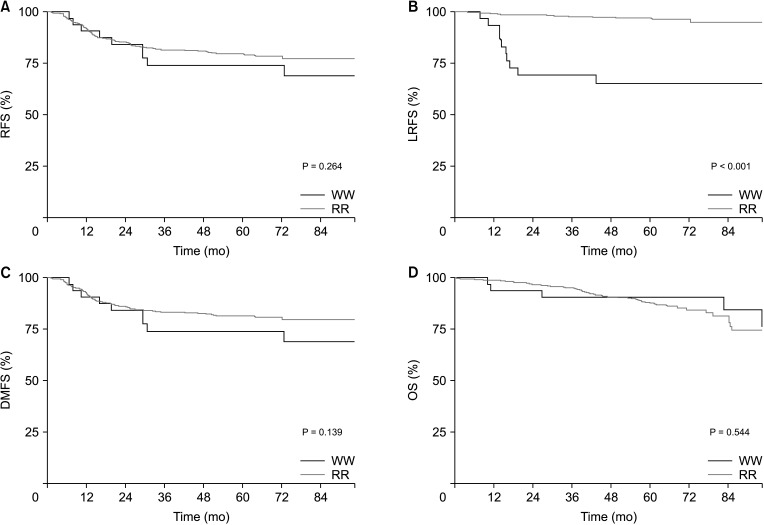 | Fig. 3Oncologic outcomes according to treatment strategies; watch-and-wait (WW) vs. radical resection (RR). (A, C, D) Recurrence-free survival (RFS), distant metastasis-free survival (DMFS), and overall survival (OS) did not differ between WW and RR groups. (B) Local recurrence-free survival (LRFS) was significantly low in the WW group.
|
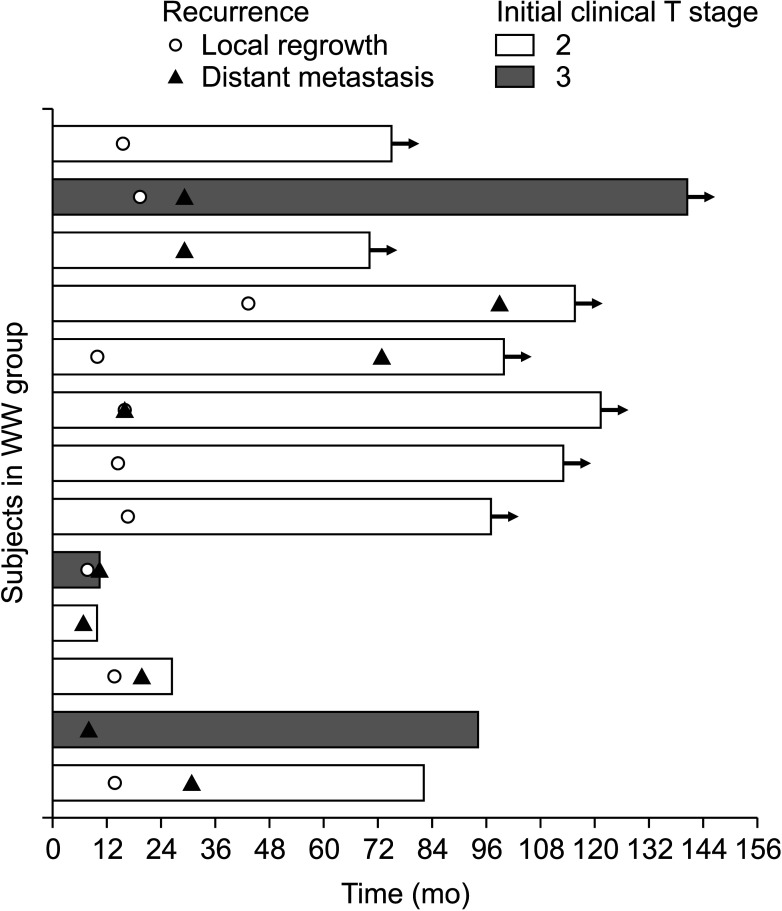
In the WW group, 13 patients (38.2%) experienced a recurrence and 10 patients had local regrowth. Seven of 10 patients with local regrowth were subsequently diagnosed with distant metastases. After local regrowth, 3 lung metastases, 3 distant lymph node metastases, and 1 liver metastasis developed. After local regrowth, the duration to distant metastases ranged from 3 to 80 months (Fig. 4). Nine of 10 patients with local regrowth underwent salvage resection, while 1 refused surgery. Four patients underwent abdominopelvic resection (APR) and 5 patients had a sphincter-saving resection. Two patients had postoperative complications after APR. One patient was undergone small bowel resection due to mechanical ileus at the postoperative 6th date; another patient was treated with conservative treatment because of ileus after 1 month of surgery. Both were discharged without other morbidities after treatment.
In the RR group, 83 patients reported tumor recurrence. The lung was the most prevalent location of recurrence (n = 46, 55.4%), followed by the liver (n = 11, 13.3%), and bone (n = 4, 4.8%). Local recurrence developed in 12 patients (14.5%).
We examined factors associated with RFS, LRFS, DMFS, and OS. Multivariate analysis revealed that treatment methods (odds ratio [OR], 16.47; 95% CI, 6.84–39.68; P < 0.001) and cT stage prior nCRT (OR, 3.34; 95% CI, 1.08–10.38; P = 0.037) were risk factors for LRFS. The pre-nCRT cT stage was also related to RFS in multivariate analysis. For the DMFS, treatment strategy and pre-nCRT cT stage were statistically significant factors. Only the pre-nCRT cT stage was related negatively to OS (Table 2).

Oncologic outcomes between radical resection and watch-and-wait according to propensity score matched group
The PSM group comprised 165 patients. Thirty-three patients were in the WW group and 132 patients were in the RR group.
Among these matched patients, 5-year RFS (73.2% vs. 84.0%) and OS (90.1% vs. 88.3%) did not differ between the WW and RR groups. In contrast, 5-year LRFS (67.5% vs. 96.5%) and DMFS (73.2% vs. 86.4%) rates demonstrated a statistically significant difference between the 2 groups (Fig. 5).
 | Fig. 5Oncologic outcomes according to the treatment strategies in the propensity score matched group. (A) Recurrence-free survival (RFS) and (D) overall survival (OS) were not different between groups. But, (B) local recurrence-free survival (LRFS) and (C) distant metastasis-free survival (DMFS) were significantly lower in the watch-and-wait (WW) group than in the radical resection (RR) group.
|
Initial cT stage was a negative factor for RFS (P = 0.019). Treatment strategy was the only significant covariate in LRFS (P < 0.001) and DMFS (P = 0.024), but there were no statistically significant covariables in OS.
Go to :
DISCUSSION
Our study revealed that there were no statistically significant differences in RFS and OS between WW and RR treatment groups of patients with rectal cancer who were diagnosed ≤ycT2 stage following nCRT. However, for LRFS, the WW strategy was inferior to RR. In DMFS, there was no difference in the survival graph, but in the multivariate analysis, the WW strategy was a risk factor. The initial cT stage was a risk factor in RFS, LRFS, DMFS, and OS. Local regrowth was the sole notion applicable to the WW group, as there was no regrowth of tumors on the intact rectum in the RR group. Thus, we did not access only local regrowth. LRFS was computed utilizing local regrowth and local recurrence. RFS and OS were not statistically different between the WW and RR groups using the PSM method. DMFS and LRFS both demonstrated that the WW strategy was a risk factor in the PSM group.
In cCR patients with rectal cancer following nCRT, the WW strategy was comparable to surgery. The 3-year RFS and OS were comparable in the WW and RR groups. In addition, colostomy-free survival was greater in the WW group [18]. Moreover, systemic reviews of WW demonstrated that it was not inferior to surgical resection [141518]. In addition, there were no significant differences between WW and surgery in terms of non-regrowth cancer recurrence [15]. However, these studies and others only included patients with cCR [19]. Our study included patients with ≤ycT2 stage, which may account for the disparate results. Our study found a substantial difference between DMFS and LRFS. As a result of local regrowth, the WW strategy was inferior to RR, demonstrating the difficulty of implementing WW.
Near cCR is comparable to ≤ycT2 stage after nCRT. There were studies conducted on patients with near cCR following nCRT [2021]. However, the status of lymph node metastasis cannot be verified, and complications also occurred in local excision [22]. However, it has a distinct advantage in terms of pathologic confirmation of tumor response and residual tumor, and it can be used in a subgroup of patients whose primary tumor status needs to be determined.
According to some investigators, the WW strategy lacks evidence and is still difficult to implement as a treatment. In a retrospective review study, all patients who received nCRT underwent resection [23]. This study showed that the pathologic complete response rate among clinical complete responders was 25%. Therefore, the authors recommended basing treatment decisions not on the absence of clinical tumor following nCRT, but on underlying conditions and comorbidities of patients. Other studies have also found insufficient evidence to prove the oncological safety of WW [1824]. In another study, 3 out of 5 patients with ypT2 experienced local regrowth, and salvage surgery was recommended [21]. Our study also indicated that the WW alone strategy for patients with ≤ycT2 stage lacked sufficient oncologic safety. Successful salvage rate and complication following salvage surgery are important issues in the era of WW for rectal cancer. Local regrowth developed in 10 patients, and 9 patients underwent salvage surgery was indicated in the present study. R0 resection was possible in 88.9%. Complications occurred in 2 patients (22.2%). Ileus is the most frequent complication. Four patients had APR, other 5 patients had sphincter-saving surgery. Only 1 patient was done R1 resection after APR, but 3 patients were not performed sufficient lymph node dissection (<12 lymph nodes). Salvage resection for local recurrence is associated with high rates of R1 resection [20]. But, our results showed high rates of R0 resection. These differences may become from patient selection and appropriate timely intervention. So, WW solely strategy was not an appropriate treatment. Proper intervention such as salvage surgery was needed for WW strategy.
In the WW group, 7 out of 10 patients with local regrowth developed distant metastasis. The WW treatment strategy was a risk factor for DMFS. Asan Medical Center has not used additional chemotherapy such as induction or consolidation chemotherapy. In fact, patients of the WW group included in this study did not receive adjuvant chemotherapy. However, in this study, patients who underwent RR got adjuvant chemotherapy. The difference in chemotherapy would account for the difference in DMFS.
The inferior DMFS in the WW group treated with nCRT in the present study would support the use of TNT for organ preservation strategy in rectal cancer patients. In a recent report, TNT enhanced the proportion of good responders (cCR or near cCR) and made organ preservation successful for more than half of the patients [2526]. Considering the worse DMFS in the WW group in this study, TNT followed by the WW strategy appears to be an effective treatment for maintaining oncologic safety.
The clinical T stage prior to nCRT has been recognized as a key risk factor in the WW strategy [2728]. Comparing cT3 to cT4, patients with cT2 rectal cancer at baseline were more likely to continue an organ preservation pathway after local regrowth through transanal local excision. Our study also showed that the pre-nCRT cT stage was a significant risk factor in RFS, LRFS, DMFS, and OS. As the initial cT stage is a risk factor, it must be taken into account when developing a treatment strategy.
It is difficult to discern the clinical stage following nCRT because it is interpreted by a human and is not a numerical indicator like a laboratory test, therefore there may be individual variation. Despite the difficulty in determining the stage of rectal cancer, there have been many studies on the classification of rectal cancer stages using MRI [162930]. If the clinical stage is split too precisely, there may be an issue with accuracy. Recently, it has more acceptable for clinical practice to classify patients roughly as responders and nonresponders [21]. Therefore, the application of the WW strategy to solely cCR patients may be limited. Extensive studies are required to confirm this strategy.
Our study has several limitations. First, this study was conducted retrospectively. In addition, patient selection bias was not removed from our study because surgeons considered the tumor growth pattern, stage, age, and comorbidities while selecting patients for the WW group. Patients with less advanced cancer stage or were in better healthier were selected for the WW group. However, 5 patients were chosen for the WW group due to their adamant refusal of surgery. Patient selection was not randomized. Thus, we matched age, pretreatment clinical stage, and sex using PSM methods by matching. PSM was performed to minimize bias. Applying the WW strategy itself can cause selection bias. Therefore, in order to minimize the bias, the variables were matched and compared. After matching patients with similar clinical characteristics, 1:4 matching was performed to include as many patients as possible.
In our study, the WW strategy for patients with ≤ycT2 stage following nCRT demonstrated poorer LRFS and DMFS than the RR group. Although LRFS would be expected due to the inclusion of local regrowth, the interpretation of the inferior DMFS in WW requires caution. Some causes might be suggested. Among the patients with ycT2 stage who were included in WW, some may have an inadequately responsive tumor. In addition, many patients in the WW group were not treated with adjuvant chemotherapy. Consequently, we need to study how to improve diagnostic accuracy and distant control. In terms of organ preservation, the combination of WW and TNT is a promising treatment. In addition, by showing that the initial cT stage is a risk factor, it is vital, when determining a treatment strategy, to evaluate whether invasive treatment should be administered based on the degree of the pre-nCRT clinical stage.
In patients with ≤ycT2 stage, a WW-only strategy did not assure oncologic safety. The initial cT stage was a risk factor for every survival graph. Consider a more intrusive treatment and short-term surveillance should be considered if the initial cT stage is high.
Go to :
 XML Download
XML Download