

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
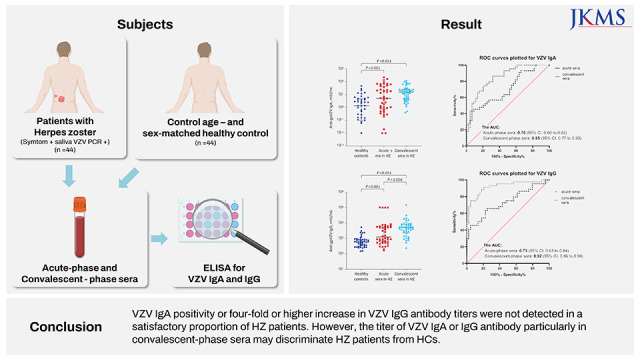
Primary infection with varicella zoster virus (VZV) results in chickenpox, and reactivation of latent VZV may lead to infection manifestation in the form of a painful vesicular rash called herpes zoster (HZ).1 The diagnosis of HZ is relatively accurate based on the characteristic rashes and vesicles that appear before and after the onset of neuropathic symptoms. However, diagnostic confirmation may be warranted in some cases. Polymerase chain reaction (PCR) has been used for the diagnosis of VZV reactivation from the characteristic vesicles, cerebrospinal fluid, plasma, and saliva.234567 Serological diagnosis of VZV reactivation is useful to confirm clinical diagnosis, especially when vesicle specimens are of poor quality or are not available at all. Serological testing of VZV-specific antibodies has been widely used for the diagnosis of zoster sine herpete or subclinical reactivation without rash.8 VZV IgM and immunoglobulin G (IgG) have been widely investigated in VZV infection,7910 while the clinical significance of VZV immunoglobulin A (IgA) has not been well elucidated.11 Thus, in the present study, we investigated the diagnostic usefulness of VZV serology, especially VZV IgA from the plasma of patients with confirmed VZV reactivation. In addition, we evaluated if the titers of VZV IgA and IgG antibodies could discriminate HZ patients from healthy controls (HCs) and determined the cut-off values to identify patients with HZ during the acute phase and after 4 weeks.
METHODS
Study patients
Subjects aged ≥ 18 years with confirmed HZ were enrolled between May 2017 and April 2018.
During the study period, 88 (44 with HZ and 44 with HCs) subjects were prospectively enrolled. Saliva and blood samples were concurrently collected from the two groups of subjects. The diagnosis of HZ was established from the presence of a dermatomal distribution rash and pain at the time of enrollment by attending physicians along with positive saliva VZV DNA PCR result. HCs were sex- and age-matched healthy volunteers without known underlying disease or evidence of active HZ. All HCs had never been previously diagnosed with HZ before and had no history of HZ vaccination.
Saliva was collected from 44 patients, and concurrent blood samples were obtained from all HZ patients on the first visit day (acute phase) and after 4 weeks (convalescent phase). All 44 healthy volunteers (group 2) provided blood and saliva samples for once.
VZV PCR of saliva DNA
Saliva samples (1 mL or more) were collected with an Omnigene-Oral kit (DNA Genotek, Ottawa, Canada) at any time of day, at least 1 hour after a meal. The samples were vigorously shaken for at least 10 seconds and then incubated in a water bath at 50°C for 1 hour. DNA was extracted with a QIAamp DNA mini kit (Qiagen Inc., Chatsworth, LA, USA) as described by the manufacturer. VZV was quantified with a VZV real-time PCR kit (GeneProof, Brno, Czech Republic) using a LightCycler 96 System (Roche, Basel, Switzerland). VZV DNA copy numbers were determined by comparing the cycle threshold values of the test samples to the value of the reference VZV DNA supplied with the PCR kit.
VZV antibody level
Paired sera from group 1 patients with acute HZ were analyzed for the presence of VZV IgG and IgA antibodies. Serum samples from HCs were analyzed for VZV antibodies once. Anti-VZV IgG and IgA antibodies were detected using glycoprotein enzyme-linked immunosorbent assays (ELISAs) (Institut Virion/Serion GmbH, Würzburg, Germany) according to the manufacturer’s protocol. Data were acquired using a Spark microplate reader (Tecan Trading AG, Männedorf, Switzerland). VZV IgA and IgG positivity was defined as ≥ 50 and 100 mIU/mL, respectively, as recommended by the manufacturer. All plasma pairs were examined in parallel at the same time.
Statistical analysis
Statistical analyses were performed using SPSS v20 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as median and interquartile range (IQR) and compared using the Mann-Whitney U test. Categorical variables were compared using the Pearson χ2 test. Paired data were compared using the Wilcox test. Receiver operating characteristic (ROC) curves were plotted for VZV IgA or IgG to assess its diagnostic performance for discriminating HZ-positive samples from HZ-negative samples. We determined the optimal cut-off value for VZV IgA and IgG by constructing ROC curves, followed by calculation of the Youden index.12 A two-tailed P < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics
The study subjects included 44 patients with HZ and 44 healthy volunteers. No differences were observed in the baseline characteristics of the two groups. The demographic characteristics of the patients with HZ are shown in Table 1. Among 44 patients with HZ, 10 (22.7%) were immunocompromised. The most common viral sites were V1 (34.1%) and the thoracic nerve area (31.8%). Disseminated zoster was identified in three patients (6.8%). Twelve of 44 HZ patients (27.2%) developed postherpetic neuralgia. Salivary VZV DNA was detected in all patients at the first visit, and the median salivary VZV DNA load was 2.44 log copies/mL. However, none of the saliva samples from HC with non-stress conditions was positive for VZV DNA.
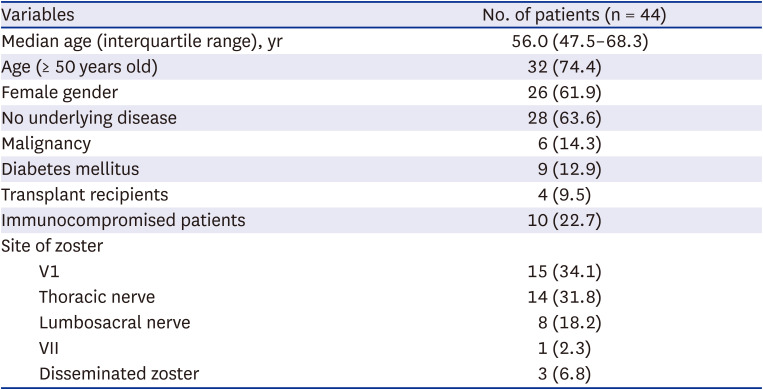
Table 1
Baseline characteristics of herpes zoster patients
![]()
VZV-specific IgA and IgG antibodies
The paired sera obtained during the acute and convalescent phase from 44 patients with HZ were examined by ELISA for the presence of VZV IgA and IgG antibodies. The results were compared with those of single serum samples from 44 HCs.
VZV-specific IgA antibody was detected in 9 of 44 (20.5%) patients in acute phase and 8 of 44 (18.2%) patients in convalescent phase. No VZV IgA antibody was detected in the sera of HCs. The median value of IgA against VZV in HCs was 1.35 mIU/mL (IQR, 0.10–4.81 mIU/mL), while the median values in HZ patients during acute and convalescent phases were 5.2 mIU/mL (IQR, 0.79–45.1 mIU/mL) and 15.8 mIU/mL (IQR, 4.42–25.8 mIU/mL), respectively. The median values of VZV IgA depicted on a log scale, during the acute (P < 0.001) and convalescent phases (P < 0.001) were also significantly higher that the median value reported for HCs (Fig. 1A). However, the value of VZV IgA was not different between the sera of acute and convalescent phases among HZ patients.
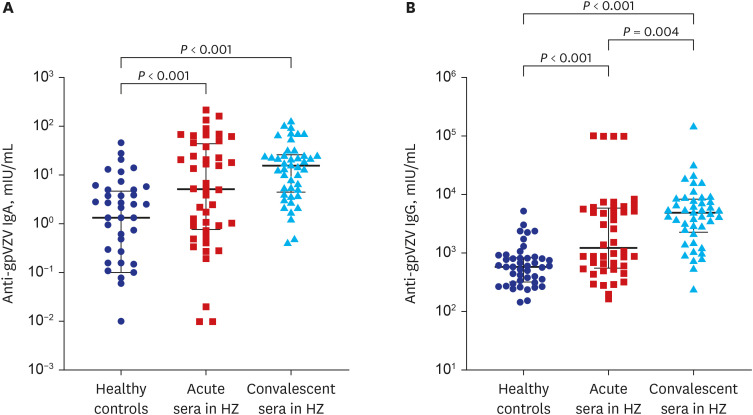
Fig. 1
Level of VZV-specific IgA (A) and IgG antibodies (B) among 44 herpes zoster patients and 44 HC subjects, depicted on a log-scale. Bars show the median and interquartile range.
VZV = varicella zoster virus, IgA = immunoglobulin A, IgG = immunoglobulin G, HC = healthy control, HZ = herpes zoster.
![]()
VZV-specific IgG was detected in both HZ and HC groups. The VZV IgG levels increased in 32 of 44 (72.7%) HZ patients during 4 weeks. A four-fold or higher increase in VZV IgG antibody titer was detected in 16 of 44 (36.4%) paired sera of HZ patients. The median VZV IgG antibody titers of HZ patients during acute (1,471.0 mIU/mL, IQR, 557.4–5,898.9, P < 0.001) and convalescent (4,934.7 mIU/mL, IQR, 2,264.5–8,576.4, P < 0.001) phases were significantly higher than the median titer reported for HC (591.6 mIU/mL, IQR, 322.0–853.0) (Fig. 1B). In HZ patients, VZV IgG levels in convalescent phase sera were significantly higher than those in acute-phase sera (4,934.7 vs. 1,471.0 mIU/mL, P = 0.004).
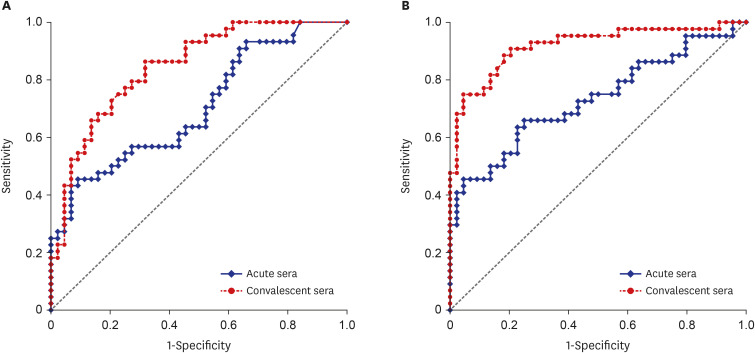
ROC curves were plotted for VZV IgA and IgG level to assess their diagnostic performance for discriminating HZ-positive samples from HZ-negative samples. For VZV IgA, the area under the curve (AUC) was 0.70 (95% confidence interval [CI], 0.60–0.82) in acute-phase sera and 0.85 (95% CI, 0.77–0.93) in convalescent-phase sera (Fig. 2A). For VZV IgG, the AUC was 0.73 (95% CI, 0.63–0.84) and 0.92 (95% CI, 0.86–0.98) for acute- and convalescent-phase sera, respectively (Fig. 2B). On the basis of the ROC curves obtained for VZV IgA levels, we selected the optimal cut-off values of 15.1 mIU/mL (sensitivity 43.2% and specificity 93.2%) and 2.8 mIU/mL (sensitivity 86.4% and specificity 68.1%) for acute- and convalescent-phase sera, respectively. For VZV IgG, we selected an optimal cut-off value of 844.5 mIU/mL (sensitivity 65.9% and specificity 75.0%) for acute-phase sera and 940.8 mIU/mL (sensitivity 83.6%, specificity 79.6%) for convalescent-phase sera to predict HZ. Regarding the use of VZV IgA antibody titer to identify HZ, 80% sensitivity could be achieved at a specificity of 40.9% and 68.2% at baseline and 1 month, respectively. On the other hand, achieving 80% specificity would warrant a sensitivity of 47.7% and 68.2% at baseline and 1 month, respectively. To apply VZV IgG antibody titer for HZ detection, a specificity of 38.6% and 86.4% at baseline and 1 month, respectively, would yield a sensitivity of 80% and a sensitivity of 54.6% and 88.6% at baseline and 1 month, respectively, would yield a specificity of 80%. VZV IgA or IgG titer in convalescent-phase sera was more useful than that in acute-phase sera for HZ diagnosis.
DISCUSSION
We evaluated the diagnostic usefulness of VZV IgA and IgG antibodies to confirm HZ infection. VZV IgA was detected in 9 of 44 (20.5%) acute-phase sera and 8 of 44 (18.2%) convalescent-phase sera of HZ patients. However, a four-fold or higher increase in VZV IgG antibody titer was observed in about one-third of HZ patients. We plotted ROC curves for VZV IgA and IgG antibody and showed that appropriate cut-off values of VZV IgA or IgG antibody particularly in convalescent-phase sera could be used to discriminate HZ patients from HCs.
VZV IgA was detected in the sera of patients with acute varicella and HZ.13 In the present study, the frequency of VZV IgA positivity (20.5%) in the acute-phase sera was lower than that reported in previous studies (80.0–100.0%), probably owing to the differences in the methods used, patient’s clinical status, and time of specimen collection.131415 VZV IgA titers did not increase after HZ, as observed in other reports.15 IgA antibodies in the acute-phase sera are not reliable markers for the diagnosis of HZ, and even in convalescent-phase sera, only 18% of samples showed a positive reaction. Thus, IgA results should be interpreted with caution.
HZ is caused by reactivation of VZV; thus, to make an accurate serological diagnosis, the response of IgG antibody during the acute and convalescent periods is important. Evidences suggest that the endogenous boosting of VZV antibody levels after clinical VZV reactivation and in the absence of HZ are associated with the subclinical VZV reactivation or re-exposure to VZV.616 In general, a four-fold or higher increase in VZV IgG antibody titer is observed in the sera of HZ patients.7 However, it is of limited value for early diagnosis of HZ, as it only provides retrospective serological confirmation of HZ after the analysis of paired serum samples.
To overcome these limitations, we evaluated whether VZV-specific antibody level at a single point can discriminate between HZ-positive and HZ-negative samples using ROC curves. We chose cut-off values of VZV IgA and IgG antibodies to identify patients with HZ in the acute phase and the first month after HZ infection. However, as shown in a previous report,6 we could not obtain an optimal cut-off value with both high sensitivity and specificity. We lost specificity while trying to achieve high sensitivity for VZV IgA, especially with acute-phase sera of HZ patients. Thus, the VZV IgA test with acute-phase sera aims for diagnostic confirmation. For VZV IgG, we chose to set cut-off values to achieve high sensitivity using antibody titer as an initial screening test for recent HZ infection.
HZ patients in the current study were confirmed by salivary VZV DNA positivity. There are many HZ mimicking conditions such as herpes simplex infection and dermatologic diseases. Although VZV PCR in vesicular sample is the gold standard for diagnosis of HZ, those of salivary samples were also comparable according to the previous reports.25 Therefore, our study result might be more reliable than enrolling clinically diagnosed shingles patients. Traditional serological diagnosis of HZ, such as VZV IgA positivity or four-fold or higher increase in VZV IgG antibody titers, were not detected in a satisfactory proportion of confirmed zoster patients. Therefore, it might be useful to consider molecular test such as salivary VZV DNA test in especially atypical HZ.
This study was limited by the fact that the sample size was relatively small and the patient group was heterogeneous; approximately 23% of the study patients were immunocompromised. However, a few reports have shown that VZV-specific humoral immunity is not impaired in immunocompromised patients.1718 In addition, we further compared the IgA and IgG levels for VZV in the acute and convalescent phases by dividing the patients into immunocompetent and immunocompromised groups, and there was no statistically significant difference (Supplementary Table 1). The VZV IgM antibody test is usually used for the diagnosis of acute VZV infection; however, we did not perform VZV IgM antibody test because it is less sensitive and often provides false-positive result, especially when the plasma samples contain rheumatoid factors.719 Thus, we used VZV IgA instead of VZV IgM for the diagnosis of VZV reactivation; however, we could not compare the diagnostic usefulness of VZV IgM and IgA antibodies.
In conclusion, VZV IgA positivity or a four-fold or higher increase in VZV IgG antibody titer was not observed in a satisfactory proportion of patients. This assay may not be helpful for zoster sero-diagnosis. However, the titer of VZV IgA or IgG antibody particularly in convalescent-phase sera may discriminate HZ patients from HCs.
 XML Download
XML Download