

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Obstructive lung disease (OLD) is a chronic respiratory condition characterized by airflow limitation. Airflow limitation is commonly defined as a reduced ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC). Most airflow limitations are caused by chronic obstructive pulmonary disease (COPD) or asthma, although a broad spectrum of other chronic airway diseases also contribute to airflow limitation.1 The prevalence of airflow limitation has increased globally,2 influenced by cigarette smoke and air pollution.34 Airflow limitation is related to increased mortality in not only chronic airway disease such as COPD5 and asthma,6 but in lung cancer,7 chronic infectious disease,8 chronic non-specific lung disease,9 and heart failure,10 and even in general population.6
Screening for airflow limitation by spirometric examination has been tried for early detection of OLD.11 Among the spirometric tests, peak expiratory flow (PEF) and FEV1/FVC have been evaluated as an index for screening of COPD.12 The AU-ROC of pre-bronchodilator PEF to detect COPD in general population was 0.66 (low-risk subgroup) and 0.76 (high-risk subgroup), which are considered suboptimal for clinical applications.13 Pre-bronchodilator FEV1/FVC showed a good performance with AU-ROC of 0.84–0.85 for COPD screening only in ever-smokers.1415 Most studies for COPD screening cross-sectionally evaluated the accuracy of pre-bronchodilator spirometric indexes, but did not predict the long-term future occurrence of COPD in general population. In addition, there has been a lack of evidence on whether screening for OLD with pre-bronchodilator spirometry affects health-related quality of life or mortality.
In the general population, FEV1/FVC is not a fixed value; it decreases with age.16 Different decline rates of FEV1/FVC have been reported according to different clinical characteristics. Current or former smokers show a faster FEV1/FVC decline rate than those who have never smoked.17 An excessive decline in FEV1/FVC has been reportedly related to biologic changes such as airway smooth muscle contraction, hypersecretion, and destruction or remodeling of small airways.18 Therefore, even if the current state of lung function lies within the normal range, OLD can develop in people with an accelerated decline rate of FEV1/FVC during their lifetime. In addition, a reduced FEV1/FVC was related to a higher risk of all-cause mortality in a multivariable analysis.19 However, the association between the FEV1/FVC decline rate and all-cause mortality or respiratory mortality has not been sufficiently studied in general population.
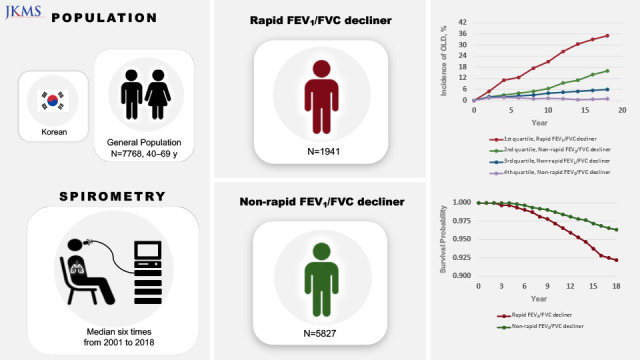
In this context, we aimed to evaluate the FEV1/FVC decline rate in the Korean general population and compare the incidence rate of OLD and the risk of all-cause and respiratory mortality between participants with rapid and non-rapid FEV1/FVC decline.
METHODS
Our study has been structured according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.20
Study design and eligibility criteria
We conducted an observational longitudinal study to evaluate the general population between 40 and 69 years of age with biannual follow-up from 2001 to 2018. We analyzed epidemiologic data and lung function information of two prospective population-based studies (the rural Ansung and urban Ansan cohorts) as sub-cohorts of the Korean Genome Epidemiology Study (KoGES). Detailed information on the study design for the two cohorts has been described in a previous cohort profile report.21 The eligibility criteria for this study were as follows: 1) presence of spirometric information at baseline examination, and 2) subsequent follow-up with spirometric evaluation. We excluded the subjects with existing airflow limitation (FEV1/FVC < 0.7) at baseline examination.
Variables and outcomes
For baseline sociodemographic and anthropometric information, we evaluated age, sex, body mass index (BMI), waist circumference, history of cigarette smoking, cigarette pack-years, history of physical exercise, school year, and income. For baseline medical information, underlying comorbid disease and medication history were acquired through protocolized and systematic questionnaires. For baseline lung function information, we evaluated pre-bronchodilator FEV1, FVC, FEV1/FVC (%), and forced expiratory flow between 25% and 75% of vital capacity (FEF25-75). A proportion of preserved ratio impaired spirometry (PRISM) was checked. For baseline general medical conditions, we evaluated the results of a complete blood count test and blood laboratory test. The development of OLD was defined using the spirometric criterion for airflow limitation of pre-bronchodilator FEV1/FVC < 0.7. We obtained information on all-cause mortality and specific causes of death from Statistics Korea.
Spirometric data
We calculated the annual FEV1/FVC decline percentage point (%p) for each participant using the Spirometry Longitudinal Data Analysis (SPIROLA) Software (Centers for Disease Control and Prevention, MorganTown, WV, USA).22 A linear regression slope, which is the beta-coefficient, for each individual was estimated using all available spirometric information from baseline examination to the last follow-up. Follow-up was terminated by death or censoring. We estimated missing FEV1/FVC values by linear interpolation or extrapolation to figure out the year in which FEV1/FVC was expected to decrease to below 0.7.
Definition of rapid decline
As an appropriate definition for rapid FEV1/FVC decline was not found through systematic review, we made an operational definition for rapid FEV1/FVC decline based on the quartiles of the annual FEV1/FVC decline rate. This approach was also used to define rapid FEV1 decline in previous studies.232425 The most negative change in FEV1/FVC (1st quartile) was defined as rapid FEV1/FVC decline. The other quartiles (2nd, 3rd, and 4th quartiles) were defined as non-rapid FEV1/FVC decline. The participant with rapid FEV1/FVC decline was referred to as a rapid FEV1/FVC decliner, while the participant with non-rapid FEV1/FVC decline was referred to as a non-rapid FEV1/FVC decliner.
Statistical analysis
We used Student’s t-test or the Wilcoxon rank-sum test to analyze continuous variables and the chi-square test or Fisher’s exact test to analyze categorical variables. A multivariable linear mixed effect model was used to evaluate the clinical factors related to annual FEV1/FVC change. Repeatedly measured lung function was considered as a random effect variable and other variables as fixed effect variables in our linear mixed effect model. We performed a multivariate Poisson regression analysis to compare the incidence rate ratio (IRR) of OLD between the rapid and non-rapid FEV1/FVC decliners. The Cochran−Armitage test for trend was conducted to evaluate the incidence of all-cause mortality across deciles. Kaplan−Meier survival analysis with log-rank test was conducted for all-cause mortality and respiratory mortality. Univariate and multivariate Cox proportional regression analyses were performed to determine whether rapid FEV1/FVC decline is an independent risk factor for all-cause mortality and respiratory mortality. The stepwise variable selection method was applied for the multivariable Poisson regression model or Cox proportional regression model using the R package 'My.stepwise'. The stepwise variable selection method initially selected variables with P < 0.05 in univariable analyses and excluded variables with P ≥ 0.05 by performing multivariable analysis whenever variables were added one by one. For multivariable Cox regression analyses, adjustment variables including age, sex, BMI, waist circumference, smoking history, income, congestive heart failure, and platelet were used to evaluate all-cause mortality and those including age, sex, smoking history, income, congestive heart failure, total cholesterol were used to evaluate respiratory mortality. P < 0.05 was considered statistically significant. The variance inflation factor for significant multicollinearity was > 4.0. R statistical software, version 4.1.0 (R Core Team [2020], Vienna, Austria), was used for all statistical analyses.
Ethics statement
The Institutional Review Board (IRB) Committee of Seoul National University-Seoul Metropolitan Government (SNU-SMG) Boramae Medical Center approved the study protocol (IRB No. 07-2022-10). Our study followed the ethical guidelines of the Declaration of Helsinki in 1975. The Korean Centers for Disease Control and Prevention obtained written informed consent from all patients included in the study.
RESULTS
Among the 10,030 participants, baseline FEV1/FVC was measured in 9,791 and follow-up FEV1/FVC was measured in 8,554. Among the eligible 8,554 participants, we excluded 786 with FEV1/FVC < 0.7 at baseline. Eventually, we included 7,768 participants in this study (Supplementary Fig. 1). During the study period, the median number of times that FEV1/FVC was measured was 6 (interquartile range = 3–7) for each patient, and the median annual FEV1/FVC decline rate was 0.32 (interquartile range [IQR] = 0.14–0.54) %p/year (Supplementary Fig. 2). Among the eligible 7,768 patients, 1,941 (25.0%) were described as rapid FEV1/FVC decliners, and the remaining 5,827 (75.0%) were described as non-rapid FEV1/FVC decliners.
Demographic and clinical features
Rapid FEV1/FVC decliners were predominantly male, older, and had a lower BMI, a smaller waist circumference, and more cigarette smoking exposure (Table 1). Rapid FEV1/FVC decliners also exercised lesser, had a shorter school year, and had less income. We found no significant difference in underlying comorbidities and medication history between the non-rapid and rapid FEV1/FVC decliners. In the baseline spirometric assessment, rapid FEV1/FVC decliners showed a lower FEV1 (%) or FVC (%) but a higher FEV1/FVC than the non-rapid FEV1/FVC decliners (Table 2). In the laboratory findings, inflammatory markers such as white blood cell (WBC) count and high-sensitivity C-reactive protein (hs-CRP) levels were higher in the rapid FEV1/FVC decliners.
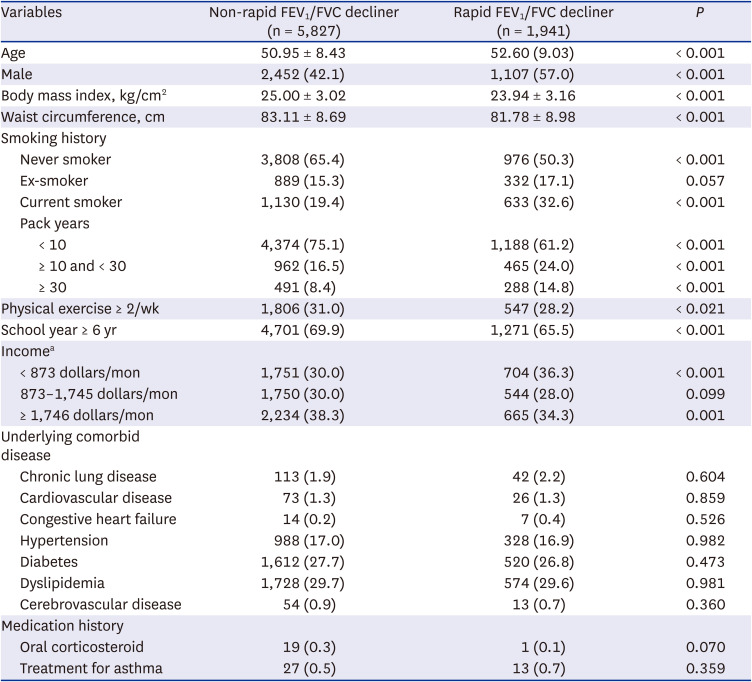
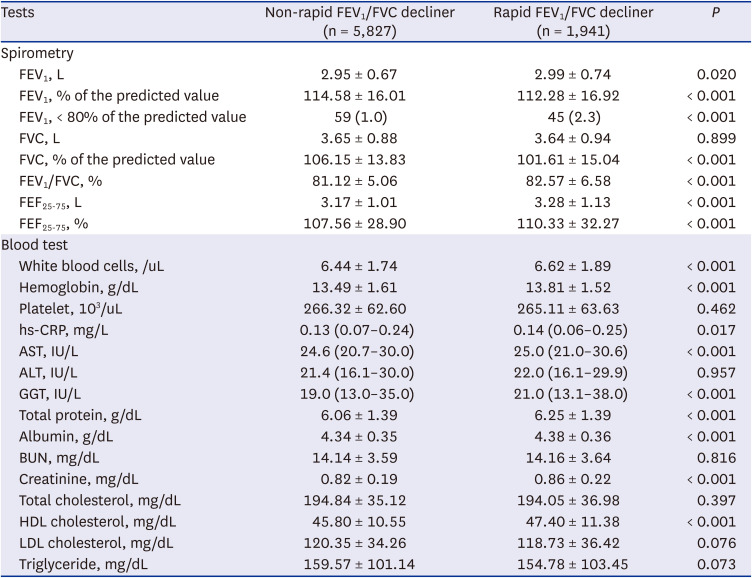
Table 1
Baseline characteristics of non-rapid and rapid FEV1/FVC decliner
Data are expressed as mean ± standard deviation or number (percentage).
FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity.
a1,000 won is converted into 0.873 dollar.
![]()
Table 2
Spirometric and laboratory findings at initial assessment
Data are expressed as mean ± standard deviation, median (interquartile range), or number (percentage).
AST = aspartate aminotransferase, ALT = alanine aminotransferase, BUN = blood urea nitrogen, CRP = C-reactive protein, FEF25-75 = forced expiratory flow between 25-75% of vital capacity, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, GGT = Gamma glutamyl transpeptidase, HDL = high-density lipoprotein, IU = international unit, LDL = low-density lipoprotein.
![]()
FEV1/FVC decline and OLD
FEV1/FVC was reduced annually by 0.76 (IQR = 0.63–1.05) %p in rapid FEV1/FVC decliners and 0.24 (IQR = 0.06–0.37) %p in non-rapid FEV1/FVC decliners (Supplementary Fig. 3). We found that FEV1 (%) decline rate was faster in rapid FEV1/FVC decliners, while FVC (%) decline rate was similar between rapid and non-rapid FEV1/FVC decliners. Clinical factors related to the annual decline rate of FEV1/FVC are described in Supplementary Table 1. Annual FEV1/FVC decline rate was faster with variables including older age, female sex, lower BMI, ex- or current smoker, previous history of chronic lung disease, history of treatment for asthma, higher FEV1 (L), higher FVC (L), lower FEV1/FVC (%), lower FEF25-75 (L), higher WBC, higher hs-CRP, higher total protein, and lower albumin. Risk factors related to rapid FEV1/FVC decliner were summarized in Supplementary Tables 2 and 3. In addition to the effect of cigarette smoking, other risk factors related to rapid FEV1/FVC decliner were older age, male sex, lower BMI, higher baseline FEV1/FVC, higher total protein, and higher HDL cholesterol in the total and never-smoker patients. During the follow-up period, the cumulative incidence of OLD was significantly higher in rapid FEV1/FVC decliners than in non-rapid FEV1/FVC decliners (35.0% vs. 8.5%, P < 0.001, Fig. 1). Incidence of OLD increased with worsening annual FEV1/FVC decline (Cochran−Armitage test for trend, P < 0.001). Adjusted IRR for OLD was significantly increased in rapid FEV1/FVC decliners compared to non-rapid FEV1/FVC decliners (adjusted IRR, 2.118; 95% CI, 1.932–2.324; Supplementary Table 4).
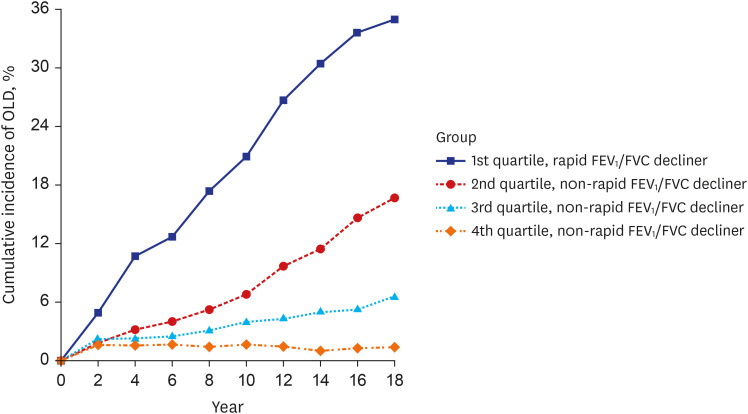
Fig. 1
Cumulative incidence of OLD according to quartiles of FEV1/FVC decline rate measured at two-year intervals. Cumulative incidence of OLD for 18 years was 35.03% in 1st quartile group, 16.67% in 2nd quartile group, 6.59% in 3rd quartile group, and 1.39% in 4th quartile group. There was a linear trend of cumulative incidence of OLD according to quartiles of FEV1/FVC decline rate (P = 0.034).
FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, OLD = obstructive lung disease.
![]()
All-cause mortality
Rapid FEV1/FVC decliners showed higher all-cause mortality than non-rapid FEV1/FVC decliners (8.0% vs. 3.9%, P < 0.001). All-cause mortality increased with worsening annual FEV1/FVC decline (Cochran−Armitage test for trend, P < 0.001, Supplementary Fig. 4). In the Kaplan−Meier curve, the probability of all-cause mortality was significantly higher in rapid FEV1/FVC decliners (log-rank test P < 0.001, Fig. 2A). We summarized the unadjusted hazard ratios (HRs) for all-cause mortality according to various clinical variables (Supplementary Tables 5 and 6). In the multivariable Cox-regression model using the clinical variables with statistical significance, we found that rapid FEV1/FVC decline was independently related to all-cause mortality (adjusted HR, 1.374; 95% confidence interval [CI], 1.105–1.709; P = 0.004; Table 3).
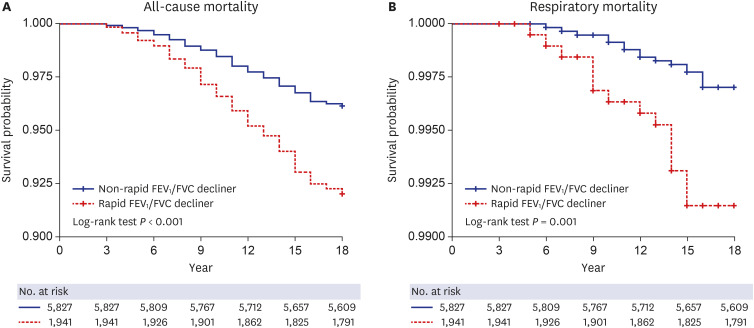
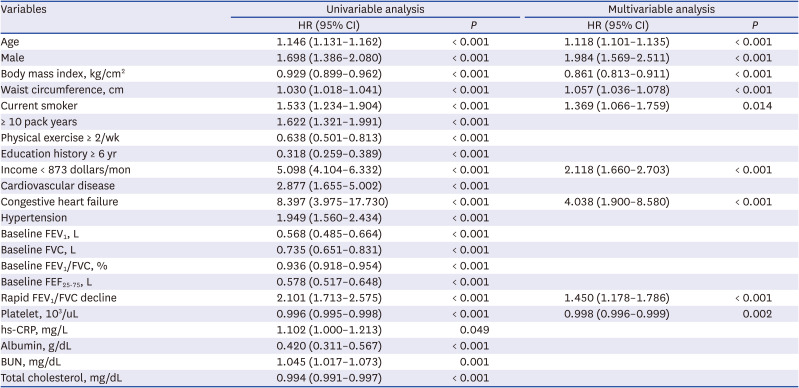
Fig. 2
Kaplan−Meier survival curve for all-cause and respiratory mortality. Survival probability was compared between non-rapid FEV1/FVC decliner and rapid FEV1/FVC decliner in terms of (A) all-cause mortality and (B) respiratory mortality.
FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity.
![]()
Table 3
Independent risk factors for all-cause mortality
FEF25-75, % was not included in this multivariable analysis due to multicollinearity with FEV1/FVC, %.
HR = hazard ratio, CI = confidence interval, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, FEF25-75 = forced expiratory flow between 25–75% of vital capacity, hs-CRP high-sensitivity c-reactive protein, BUN = blood urea nitrogen.
![]()
Respiratory mortality
We found that rapid FEV1/FVC decliners showed higher mortality due to respiratory disease than non-rapid FEV1/FVC decliners (0.8% vs. 0.3%, P = 0.003, Supplementary Table 7). In the Kaplan−Meier curve, the probability of respiratory mortality was significantly higher in the rapid FEV1/FVC decliners (log-rank test P = 0.001, Fig. 2B). We summarized the unadjusted HRs for respiratory mortality according to various clinical variables (Supplementary Tables 8 and 9). In the multivariable Cox-regression model using the clinical variables with statistical significance, we found that rapid FEV1/FVC decline was independently related to respiratory mortality (adjusted HR, 2.151; 95% CI, 1.069–4.328; P = 0.032; Table 4).

Table 4
Independent risk factors for respiratory mortality
FEF25-75, % was not included in this multivariable analysis due to multicollinearity with FEV1/FVC, %.
HR = hazard ratio, CI = confidence interval, FEF25-75= forced expiratory flow between 25–75% of vital capacity, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity.
![]()
DISCUSSION
In our longitudinal study, the subjects without airflow limitation at baseline examinations were classified into rapid and non-rapid FEV1/FVC decliners and observed for up to 18 years. The annual FEV1/FVC decline rate was 0.32%p in the general population, similar to the results of a previous systematic review that reported 0.29%p of FEV1/FVC per year.16 Compared with non-rapid FEV1/FVC decliners, rapid FEV1/FVC decliners showed two times higher covariate-adjusted incidence rate of OLD; rapid FEV1/FVC decliners had an increased risk of all-cause and respiratory mortality in the multivariable analyses. Annual FEV1/FVC decline rate may be an independent clinical factor related to the incidence of OLD and the risk of mortality in the general population.
Our study suggests that rapid FEV1/FVC decline may be a useful marker for detecting individuals with pre-COPD or those at high risk of developing COPD. Pre-COPD is a recently proposed concept for individuals who are currently without airflow limitation but have the potential to develop airflow limitation in their lifetime.26 Rapid lung function decline leading to COPD is considered an important feature of pre-COPD.2728 Many studies have analyzed annual FEV1 decline to evaluate the progression of airflow limitation; however, it has been limited to identifying when COPD develops or when treatment needs to be considered.23 In addition, FEV1 decline can worsen without progression of airway disease by factors such as low BMI that affects FVC.2930 Therefore, it is speculated that a comprehensive understanding of both FEV1 decline and FEV1/FVC decline would be helpful to find individuals with pre-COPD or make an early diagnosis of COPD.
Distinctive spirometric profiles were found in rapid FEV1/FVC decliners. At baseline, a higher proportion of PRISM was found in rapid FEV1/FVC decliners. This finding is consistent with a previous report that an accelerated FEV1 decline rate was related with PRISM.31 Considering a lower FVC % and FEV1%, a relatively smaller lung volume was suspected in rapid FEV1/FVC decliners. Although annual FEV1/FVC decline rate was attenuated by a higher baseline FEV1/FVC or FEF25-75%, a higher FEV1/FVC or FEF25-75 was a risk factor for rapid FEV1/FVC decliners. Similarly, a higher baseline FEV1 function was reportedly related with an accelerated FEV1 decline rate.3233 This finding suggests that other clinical factors in participants with a higher baseline FEV1/FVC or FEF25-75 would aggravate the FEV1/FVC decline rate.
The relationship between airflow limitation and mortality has been widely investigated.6 The severity of airflow limitation was positively correlated with all-cause mortality.34 Even after adjusting physical function and inflammatory and cardiac markers, FEV1/FVC was independently associated with mortality.35 In particular, decreased FEV1 or worsened airflow limitation was associated with increased cardiovascular mortality.36 Among the several clinical variables that have been considered to mediate the relationship between airflow limitation and mortality, chronic systemic inflammation might be the most important explanatory factor.37 Our study is the first to elucidate that although there was no current airflow limitation, the individuals with rapid FEV1/FVC decline had higher risks of all-cause and respiratory mortality. However, only a small proportion of all-cause mortality cases were accounted for by respiratory causes. This finding suggests that the chronic systemic inflammation in rapid FEV1/FVC decliners may significantly affect mortality by causes other than respiratory disease.38 Recent studies have shown that the susceptibility to airflow limitation by inhaled toxicants varies depending on genetic factors.3940 Further research on the genetic variants related to lung function decline rate may provide more plausible information on the biological mechanism between the progression of airflow limitation and mortality.
We found that old age, low BMI, current cigarette smoking, and low platelet count were the independent variables related to an increased risk of mortality and accelerated FEV1/FVC decline. Despite statistical significance, the absolute differences in age, BMI, and platelet count between rapid and non-rapid FEV1/FVC decliners were considered too small to imply clinical importance. A more impressive difference between the two groups was smoking status. Cigarette smoking increased COPD and mortality,4142 while smoking cessation improved accelerated lung function decline and reduced mortality.43 It is commonly suggested that cigarette smoking worsens the FEV1 decline rate through exacerbated airway inflammation, and the FVC decline rate through destruction of lung parenchyma.4445 The FEV1 decline seems more dominant than the FVC decline in smokers, considering that FEV1/FVC decline rate was accelerated in smokers with ≥ 10 pack-years.44 However, our study showed that half of the rapid FEV1/FVC declines were never smokers. Rapid FEV1/FVC decline was still associated with the development of OLD and mortality even after adjusting for smoking status. Therefore, irrespective of smoking status, the FEV1/FVC decline rate would be a biomarker for the development of airflow limitation and mortality.
Several limitations were found in this study. First, we used a fixed ratio of pre-bronchodilator FEV1/FVC as a spirometric criterion for diagnosing OLD. Therefore, it was difficult to distinguish between COPD and asthma, and the incidence of OLD may be overestimated, particularly in young adults.4647 Second, a false normal FEV1/FVC decline rate can be observed in certain clinical conditions that mainly worsen FVC, even though there is a definite progression of airflow limitation. In patients with combined pulmonary fibrosis and emphysema, FEV1 decline was more accelerated, but FEV1/FVC decline was more attenuated than in COPD patients.48 Therefore, it is necessary to check comorbidities that can continuously worsen FVC, such as interstitial lung disease, when interpreting the FEV1/FVC decline rate. Third, environmental and occupational exposures are important factors that affect FEV1/FVC, but it was not possible to analyze them in our study because relevant data were lacking. In individuals with lower income or educational status, a higher harmful occupational exposure is expected.49 Considering that socioeconomic status was lower in rapid FEV1/FVC decliners in our study, this group may be more exposed to toxic inhalants.
In conclusion, the annual FEV1/FVC decline rate was 0.32%p in the general population in Korea. The incidence rate of OLD and the hazards of all-cause and respiratory mortality were increased in rapid FEV1/FVC decliners. Further study is necessary to verify the benefit of periodic screening for rapid FEV1/FVC decliners, such as early detection of OLD or prevention of mortality.
 XML Download
XML Download