

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In Korea, approximately 260,000 adult men involuntarily enlist in the military every year under the mandatory military service system.1 In a recent survey, 1 in 5 Korean soldiers complained of maladjustment to military life.2 The strict top-down command system of the military organization, poor service environment, and job inappropriateness make it difficult for soldiers to adapt to their units,3 and it is highly likely that they will experience negative events in various stressful situations. Negative life events can lead to various psychological responses, such as depression, anxiety, anger, and embitterment in individuals.4 When soldiers perceive an event that they experience in the military to be unfair or unjust, and feel a high level of embitterment related to such event for a long period of time, they may have posttraumatic embitterment disorder (PTED).5
PTED is triggered by negative events experienced in daily life, such as conflict at work, unemployment, divorce, or severe illness. Embitterment, the main emotional symptom of PTED, involves mixed feelings of disappointment, humiliation, defeat, vengefulness and helplessness. PTED patients complain of anger, anxiety, and irritability in addition to long-term embitterment. In addition, as PTED is often accompanied by symptoms such as demotivation, withdrawal from social relationships, intrusive ruminations about relevant events, avoidance of people or places involved, and suicidal ideation, along with other mental disorders such as depression, anxiety, and adjustment disorder, the patients may suffer from persistent mental health problems.5
According to a study by You and Ju6 that investigated social anger in Korea, soldiers were one of the groups that most often complained of anger, along with the families of victims of accidents and workers. The biggest causes of anger in soldiers included defamation, vilification, and false accusations. In addition, 19.8% of the surveyed soldiers reported that they had been treated unfairly while serving in the military, and the types of unfair treatment included a lack of guaranteed rest (28.5%), private commands (19.8%), and verbal abuse (16.4%).2
Mental health is one of the most important factors for stable adjustment to the military and successful performance of duties.7 Soldiers with mental illness or personality issues are more likely to experience maladjustment to their units,2 feel dissatisfied with military life overall, and have difficulty in performing assigned duties with willingness.3 Mental health problems in soldiers often lead to various incidents/accidents such as assault, desertion, or casualties such as suicide and homicide, and the non-combat losses, decreased sense of unity, and demoralization caused by these incidents/accidents may escalate to a crisis for the entire military organization.3
Stress has been reported as a main threat to the mental health of soldiers.8 Soldiers are put under stress due to poor service environment, job inappropriateness, revulsion with the military service, and interpersonal problems in and out of the military,3 and high levels of stress can lead to mental health problems such as depression and suicidal ideation.9
Depression and suicidal ideation have been reported as major mental health problems among Korean soldiers. According to the 2012 Military Depression Prevalence Survey published by the Ministry of National Defense, the prevalence of major depressive disorder among 1,310 soldiers amounted to 4.6%. In a study that used a self-reporting scale to evaluate the level of depression, 20–30% of the soldiers had experienced mild or severe depression.10
Depression in soldiers is closely related to suicidal ideation,11 and according to a study that examined the prevalence of suicide-related behaviors among 463 ordinary soldiers, the prevalence of suicidal ideation in the last 6 months was found to be 5.0%, and in the past 1 year was 6.4%.12 Considering that the one-year prevalence of suicidal ideation among general adult males aged between 18 and 29 years, who are in the same age group as ordinary servicemen, is 2.6%,13 the prevalence of suicidal ideation is quite high in the military group.
Self-esteem and impulsiveness were also found to be related to soldiers’ mental health and maladjustment to the military.14 Soldiers with low self-esteem may face difficulties with military life as they lack coping skills, are prone to emotional outbursts, and are more likely to act in hostile and aggressive ways in response to negative reactions from others.15 Since impulsiveness in soldiers is a factor related to disciplinary issues, violent behavior, vulnerability to stress, depression, and suicide in the military,16 those with a high level of impulsiveness are more inclined to exhibit behavior problems.
To this day, research on embitterment or PTED in Koreans has been mainly conducted on mentally or physically ill patients,17 survivors of the Sewol Ferry Disaster,18 and the general population.6 Despite the fact that soldiers are in an environment where they can easily feel a sense of embitterment due to negative life events such as unfair treatment, no study has addressed this sort of emotion in soldiers.
The purpose of this study was to identify the prevalence of PTED among soldiers, and the relationship between PTED, stress, depression, self-esteem, impulsiveness, and suicidal ideation in soldiers, considering that PTED is associated with other mental health problems at high rates. In addition, this study also aimed to determine the characteristics of PTED in soldiers by examining differences between soldiers and the general control group in the above-listed variables and the effects of each variable on PTED.
Go to : 
METHODS
Participants
This study adopted the deliberate sampling method and was conducted on soldiers currently serving in an Army division located in Gangwon-do (Province). The data collection period for this study was from July to December 2019. Before conducting the survey, the purpose of this study was explained to the soldiers, and only those who voluntarily agreed to participate in the study were surveyed. Questionnaires were distributed to a total of 212 soldiers who were asked to take the survey on the spot, and the questionnaires were retrieved upon completion. Of the collected questionnaires, those with missing or invalid responses were excluded from the analysis, and as a result, 200 questionnaires were used as final analysis data. For the control group, men in their early 20s who had never enlisted in the military were selected as subjects, and were recruited from among college students in the two regions. Questionnaire distribution and collection were conducted in the same manner as for the experimental group. A total of 210 students completed the survey, and questionnaires with missing or invalid responses were excluded from the analysis. As a result, 197 questionnaires were used as final analysis data.
Assessment
PTED Self-Rating Scale (hereinafter the “PTED Scale”)
Developed by Linden et al.19 as a self-reported scale to evaluate the severity of the symptom of embitterment, it consists of 19 items to assess the subject’s psychological state and social functioning, emotional response to events, and thoughts about revenge. Each item is rated on a 5-point (0–4) Likert scale, and according to Linden, an average score of 1.6 points or higher for all items on this scale suggests that the subject has been suffering from long-term embitterment, while an average score of 2.5 points or higher implies that the person has a severe mental disorder- that is, PTED (Table 1). In the Korean version of the PTED scale standardized by Shin et al.,20 the internal consistency (Cronbach’s α) was found to be 0.96, and in this study it was also 0.96.
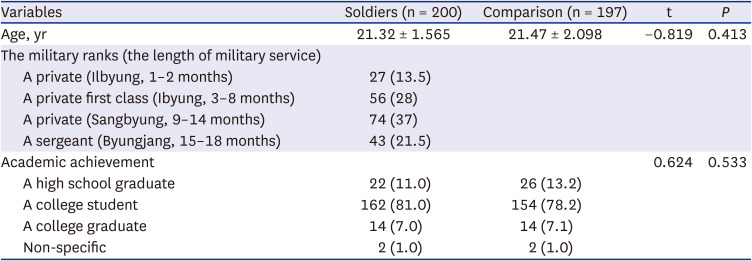
Table 1
Epidemiological characteristics of study subjects
![]()
Stress Response Inventory
The Stress Response Inventory developed by Ko et al.21 was used to measure stress responses, which include emotional, somatic, cognitive, and behavioral responses. This scale consists of a total of 39 items that represent the following 7 sub-domains of stress responses: tension (6 items), aggression (4 items), somatization (3 items), anger (6 items), depression (8 items), fatigue (5 items), and frustration (7 items). Each item is rated on a 5-point (0–4) Likert scale, with a higher score indicating a higher responsiveness to stress. The internal consistency (Cronbach’s α) in the original scale was .97, whereas in this study it was .98.
Beck Depression Inventory (BDI)
BDI devised by Beck and colleagues to evaluate the symptom of depression, it consists of 21 items that represent the domains of cognitive, emotional, motivational, and somatic symptoms. Each item is rated on a 4-point (0–3) Likert scale, with higher scores indicating higher levels of depression. The Korean version of this scale standardized by Lee and Song22 proposes 16 points as a cut-off value. The internal consistency (Cronbach’s α) of the scale was 0.78 in the study of Lee and Song22 and 0.89 in this study.
Rosenberg Self-Esteem Inventory (RSI)
This is a scale developed by Rosenberg to measure an individual’s self-acceptance pattern and overall self-esteem, and was adapted by Lee23 in Korea. It consists of a total of 10 items, including 5 items of positive self-esteem and 5 items of negative self-esteem. It is rated on a 4-point (0–3) Likert scale, with a higher score indicating higher self-esteem. In this study, the internal agreement (Cronbach’s α) was 0.64.
Barratt Impulsiveness Scale II (BIS)
This scale was designed by Barratt to assess impulsiveness, and this study used a Korean version standardized by Lee.24 It contains 23 items in total, including 6 items for attentional impulsiveness, 8 items for motor impulsiveness, and 9 items for non-planning impulsiveness. Each item is rated on a 4-point (0–3) Likert scale, with a higher score meaning higher impulsiveness. The internal consistency (Cronbach’s α) in this study was found to be 0.80.
Beck Scale of Suicide Ideation (BSI)
This is a scale developed by Beck and colleagues to evaluate suicidal ideation, and in this study, a Korean version standardized by Lee and Kwon25 was used for measurement. A total of 19 items cover the dimensions of the intensity, duration, and specificity of suicidal ideation and plans. Each item is rated on a 3-point (0–2) Likert scale, with a higher score suggesting a higher level of suicidal ideation. In the study of Lee and Kwon,25 the internal consistency (Cronbach’s α) of the scale was 0.74, while in this study it was 0.87.
Statistical analysis
The collected data were analyzed using SPSS version 21 (IBM Corp., Armonk, NY, USA), a statistical software package. Frequency analysis and descriptive statistical analysis were used to evaluate the demographic characteristics and embitterment levels of the soldiers and the control group. To identify the mean and standard deviation (SD) of major variables, descriptive statistical analysis was carried out, and the relationship between the major variables was examined with Pearson’s correlation analysis.
In addition, t-test was performed to examine the differences in stress, depression, self-esteem, impulsiveness, suicidal ideation, and PTED between the soldiers and the control group.
Finally, a hierarchical multiple regression analysis was conducted to determine the effects of independent variables on PTED in the soldiers. A hierarchical multiple regression analysis was performed with up to two models by adding variables. In Model 1, demographic variables (age and educational background) were input into the model, and in Model 2, stress, depression, self-esteem, impulsiveness, and suicidal ideation were additionally input to measure the effects on PTED.
Ethics statement
The Institutional Review Board of Dankook University permitted this study (DKU 2020-09-026). Written informed consents were provided by all participants before participation.
Go to :
RESULTS
This study surveyed a total of 397 subjects among whom 200 were soldiers aged 21.32 years on average (SD, 1.565). By military rank, the soldiers surveyed can be divided into 27 privates (13.5%), 56 privates first class (28%), 74 corporals (37%), and 43 sergeants (21.5%). By educational background, 22 of them (11.0%) were high school graduates, 162 (81.0%) were currently in college, 14 (7.0%) were college graduates, and 2 (1.0%) had another level of education. The control group consisted of a total of 197 males with an average age of 21.47 years (SD, 2.098). Classified by educational background, 26 of them (13.2%) were high school graduates, 154 (78.2%) were currently in college, 14 (7.0%) were college graduates, and 2 (1.0%) had nonspecific. No significant difference in age or educational background was found between the soldiers and the control group (Table 1).
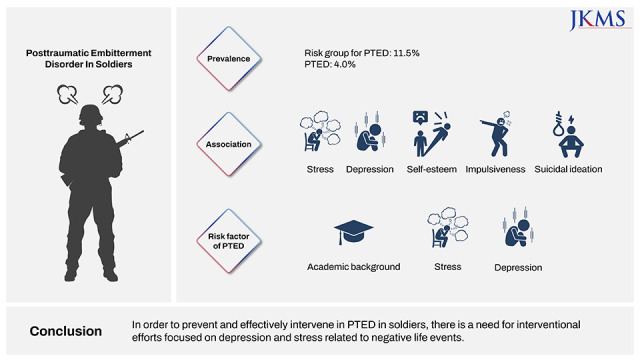
On the PTED self-reporting scale, if the average score for all 19 items is 1.6 points or higher, it suggests that the subject suffers from long-term embitterment, while if the average score is 2.5 points or higher, it can be considered that the person has PTED.5 The average score of the items among the soldiers was 0.8968 ± 0.74350, which indicates that 11.5% of them were suffering from long-term embitterment (an average score of 1.6 points or higher), and 4% were deemed to have PTED (an average score of 2.5 points or higher). The average score in the control group was 0.6359 ± 0.64588, and 12.7% of them were experiencing long-term embitterment (Table 2).

A t-test was performed to examine the differences in stress, depression, self-esteem, impulsiveness, suicidal ideation, and PTED between the soldiers and the control group. The t-test found significant differences between the two groups in all variables except for suicidal ideation. Compared with the control group, the soldier group showed statistically significant differences in stress (t = 3.296, P < 0.01), depression (t = 2.914, P < 0.01), self-esteem (t = −3.393, P < 0.01), impulsiveness (t = 2.938, P < 0.01) and PTED (t = 3.732, P < 0.001). In other words, compared with the control group the soldiers had higher stress, depression, impulsiveness, and PTED scores, and also had lower self-esteem (Table 3).
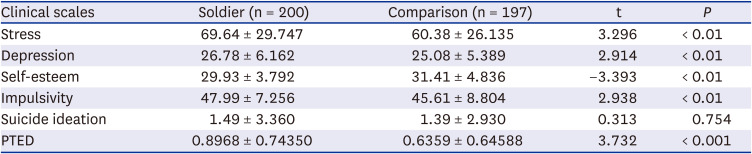
Table 3
Stress, depression, self-esteem, impulsivity, suicide ideation, and posttraumatic embitterment disorder score of the soldier and the comparison group
![]()
This study surveyed a total of 397 subjects among whom 200 were soldiers aged 21.32 years on average (SD, 1.565). By military rank, the soldiers surveyed can be divided into 27 privates (13.5%), 56 privates first class (28%), 74 corporals (37%), and 43 sergeants (21.5%). By educational background, 22 of them (11.0%) were high school graduates, 162 (81.0%) were currently in college, 14 (7.0%) were college graduates, and 2 (1.0%) had another level of education. The control group consisted of a total of 197 males with an average age of 21.47 years (SD, 2.098). Classified by educational background, 26 of them (13.2%) were high school graduates, 154 (78.2%) were currently in college, 14 (7.0%) were college graduates, and 2 (1.0%) had nonspecific. No significant difference in age or educational background was found between the soldiers and the control group (Table 1).
On the PTED self-reporting scale, if the average score for all 19 items is 1.6 points or higher, it suggests that the subject suffers from long-term embitterment, while if the average score is 2.5 points or higher, it can be considered that the person has PTED.5 The average score of the items among the soldiers was 0.8968 ± 0.74350, which indicates that 11.5% of them were suffering from long-term embitterment (an average score of 1.6 points or higher), and 4% were deemed to have PTED (an average score of 2.5 points or higher). The average score in the control group was 0.6359 ± 0.64588, and 12.7% of them were experiencing long-term embitterment (Table 2).
The t-test of both groups found significant differences between the two groups in all variables except for suicidal ideation. Compared with the control group, the soldier group showed statistically significant differences in stress (t = 3.296, P < 0.01), depression (t = 2.914, P < 0.01), self-esteem (t = −3.393, P < 0.01), impulsiveness (t = 2.938, P < 0.01) and PTED (t = 3.732, P < 0.001). In other words, compared with the control group the soldiers had higher stress, depression, impulsiveness, and PTED scores, and also had lower self-esteem (Table 3).
As seen in Table 4, The result of a hierarchical multiple regression analysis was as follows. First, in Model 1, where the demographic variables were input, educational background (β = 0.163, P < 0.05) was found to have a statistically significant positive effect on PTED (F = 0.73611, P < 0.05). In Model 2, with the additionally input variables (stress, depression, self-esteem, impulsiveness, and suicidal ideation), academic background (β = 0.114, P < 0.05), stress (β = 0.215, P < 0.01), and depression (β = 0.432, P < 0.001) had a statistically significant positive effect on embitterment (F = 26.900, P < 0.001). The explanatory power of the two models was 3.0% and 49.5%, respectively, increasing in Model 2 by 46.5% compared to Model 1.
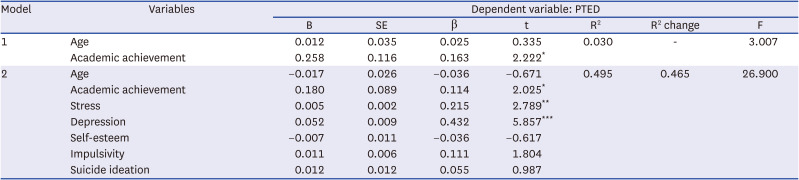
Table 4
Multiple regression analysis among variables influencing PTED
![]()
Go to :
DISCUSSION
This study intended to identify the prevalence of PTED among Korean soldiers and the relationship between PTED and stress, depression, self-esteem, impulsiveness, and suicidal ideation in soldiers. The study also sought to determine the characteristics of PTED in soldiers by examining the differences between a soldier group and a general control group in these variables and their effects on PTED.
To assess the prevalence of PTED in the soldier group and the control group, a survey with a PTED self-reporting scale was performed. The results showed that 11.5% of the soldiers were suffering from long-term embitterment (an average score of 1.6 points or higher for the items on the PTED scale), and 4% of them were found to have PTED (an average score of 2.5 points or higher). In the control group, 12.7% suffered from long-term embitterment, but none were classified as PTED patients. The two groups reported long-term embitterment at similar rates, but PTED was only reported in the soldier group. As soldiers are required to observe strict discipline and assimilate into their unit, they are more likely to face negative events such as unfair treatment compared to the control group, which causes them to experience a higher level of embitterment.
In a study that investigated the prevalence of PTED in the general Korean population,26 it was found that about 20–40% of the study subjects were suffering from long-term embitterment. The prevalence of PTED in the soldier group and the control group surveyed in this study, ranging from 11% to 13%, was lower than that in the general population. It is considered that the gender and age of the study subjects affected the result. While the subjects of the aforementioned study were men and women aged between 20 and 60 years or over, the subjects of this study, which was conducted on ordinary soldiers, were men in their early 20s. In a study by Lee et al.,27 subjects in their 30s reported a higher level of embitterment compared with other age groups, and in a study conducted on 1,000 adults aged between 18 and 35,25 women had significantly higher scores on the PTED scale than men. In particular, there is a possibility that the soldiers surveyed might have underreported the level of embitterment they were experiencing because of their desire to appear socially desirable.
This study analyzed the correlations between PTED in soldiers and other variables, and the results are as follows. Embitterment had a greater positive correlation with depression (r = 0.658, P < 0.01), stress (r = 0.592, P < 0.01), impulsiveness (r = 0.346, P < 0.01), suicidal ideation (r = .296, P < 0.01), and educational background (r = 0.170, P < 0.05), in descending order, and had a negative correlation with self-esteem (r = −0.339, P < 0.01). A higher level of education was found to be related to PTED, and this result is consistent with the finding of a previous study28 that PTED is often accompanied by a high level of depression. This result also reaffirms the assumption made by Lee et al.26 that PTED is a type of trauma- and stress-related disorder in which stressful life events act as a direct cause given a significantly positive correlation between stress and PTED. In this study, impulsiveness was also found to have a positive correlation with PTED. While no domestic or foreign preceding study has reported the relationship between PTED and impulsiveness, there is a research result showing that PTED and adjustment disorder with a high level of comorbidity are related to impulsiveness. According to a study by Yoo and Lim,29 soldiers hospitalized for adjustment disorder showed a significantly higher level of impulsiveness than ordinary soldiers. It can be therefore presumed that the level of impulsiveness will be high in PTED patients as well. The results of this study are also consistent with the finding of previous studies26 that a high level of suicidal ideation is associated with a high level of PTED. Linden5 reported that PTED patients tended to blame themselves for not being able to prevent or cope with negative events. It is thought that this tendency could explain the relationship between a low level of self-esteem and a high level of PTED.
A t-test on the soldier group and the control group in this study found that the stress, depression, impulsiveness, and PTED scores were significantly higher in the soldier group, while the self-esteem score was lower. On the other hand, there was no significant difference in suicidal ideation between the two groups. Recently, the Ministry of National Defense of Korea is promoting what it calls a “gatekeeper” system to prevent suicide attempts among soldiers of all ranks. It is also making active efforts to prevent suicide in the military by training instructors exclusively responsible for suicide prevention in battalion-level units, providing all soldiers with suicide prevention education at least once every half–year, and operating a three-stage suicide prevention system.1
It is difficult to compare the results of this study that involved soldiers and ordinary males as the experimental and control groups with the findings of preceding studies that mainly compared the characteristics of the non-adaptive and adaptive soldiers.6 It is not clear whether the specific environment of the military had an effect on the mental health of the soldiers, but the results of this study suggest that soldiers may be in a psychologically more vulnerable state compared to the general population. While research on stress, depression, and suicidal ideation in soldiers has been actively carried out, self-esteem, impulsiveness, and embitterment in this specific group have been given relatively less attention. As these variables may also affect soldiers’ adjustment to their units, duty performance, and behavior problems,14 there is a need for more attention and intervention regarding these factors.
By examining the effects of age, educational background, stress, depression, self-esteem, impulsiveness, and suicidal ideation on PTED in the surveyed soldiers, only educational background (β = 0.114, P < 0.05), stress (β = 0.215, P < 0.01), and depression (β = 0.432, P < 0.001) were found to have a significant effect on embitterment. In a previous study,26 the number of negative life events experienced by the study subjects and their perceived stress levels were identified as predictors of PTED. The stress responses measured in this study were also found to be a significant predictor for PTED. It is suggested that follow-up studies make efforts to prevent and manage PTED in soldiers by developing a validated scale to evaluate the negative life events that soldiers may experience inside and outside the military, and by specifically exploring the types of events that may cause PTED.
Depression has been reported to be closely related to PTED. In a study by Linden et al.15 that assessed the comorbidities and symptoms of 48 inpatients who were likely to be diagnosed with PTED, 52% of the study subjects complained of major depression. Lee et al.,26 who examined the relationship between embitterment and depression in the general Korean population, revealed that the severity of depression is an important predictor of PTED. They also suggested the possibility that PTED and depression, as comorbidities that frequently coexist with one another, share similar psychopathophysiological mechanisms. The results of this study also show that depression is a significant predictor of PTED in soldiers.
PTED differs from depressive disorder in that the patient’s ability to regulate emotions is not impaired and they exhibit normal emotions when they are absorbed in other activities, and in that negative events are directly related to the onset of the symptoms.15 However, as PTED and depression are often accompanied by one another and have similar symptoms, it may be difficult to differentiate and diagnose them. There may be a need for different therapeutic approaches for each of the respective cases where a soldier is diagnosed with depressive disorder, PTED, or both disorders. It is therefore suggested that follow-up studies focus on detailed symptoms that distinguish between these cases, or effective intervention methods for each case.
The limitations of this study and suggestions for follow-up research are as follows. First, it would be hasty to generalize and apply the findings of this study to the whole military population. As this study was conducted only on the soldiers serving in an army division located in two regions, sampling of more soldiers from all over the country should be carried out in follow-up studies.
Second, as this study used a self-reporting scale as a measurement instrument, there is a limit to the reliability of the collected data. In particular, it is possible that the study subjects chose socially desirable responses, lied, or responded in a careless manner.
Third, since this study was conducted as a cross-sectional study, it has limitations when it comes to clearly determining the onset times of each variables and the causal relationships between them. It is therefore considered that if a follow-up study can verify the causal relationships between these variables through longitudinal monitoring over the entire service term from enlistment to discharge, it will be able to provide a deeper understanding of embitterment in soldiers.
Despite these limitations, this study has significance as the nation’s first study to provide basic data on PTED in soldiers. While preceding studies have focused on depression in soldiers, there are symptoms that cannot be addressed only as depression. The results of this study suggest the need to deepen the understanding of PTED in soldiers, and to consider the presence of PTED when performing psychological interventions on soldiers. Follow-up studies are required to further improve the understanding of PTED in soldiers and examine different treatment techniques. In addition, in order to prevent and effectively intervene in PTED in soldiers, it is considered that interventional efforts should be made with a focus on depression and stress in soldiers related to negative life events experienced both inside and outside the military.
Go to :
 XML Download
XML Download