

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Upper gastrointestinal (UGI) foreign body (FB) ingestion is the most common indication for therapeutic gastrointestinal endoscopy in children. It most commonly occurs in children aged between 6 months and 3 years.123 Coins are the most common FBs, accounting for up to 69% of FBs ingested by children.12
Of the cases of FB ingestion that come to medical attention, 80% to 90% pass spontaneously, 10% to 20% require endoscopic removal, and < 1% ultimately require a surgical intervention.3 Flexible endoscopy has a success rate of over 95% in the removal of UGI FBs.4 There have been tremendous advances in endoscopic techniques and equipment; thus, it is becoming a common practice for pediatric endoscopists to remove FBs (more easily), rather than waiting for a spontaneous passage.5
The timing and requirements for endoscopic FB removal in children are determined by three key factors: the type of FB ingested, its location, and the patient’s symptoms.3 Large, sharp, or rapidly damaging materials, such as multiple magnets or disc batteries, require rapid removal. However, even when the FBs are not very large, if they stay in one location for a long time, or if a spontaneous passage is not expected, endoscopic removal will be required at an appropriate time. When endoscopic removal of the FB is not possible owing to the type and size of the material, location, or complications, surgical removal should be considered.
In children, when endoscopic removal is possible, there are several factors that have to be taken into consideration before performing the removal. This is because the type of FB ingested, age, weight, and sedation methods are very different in children when compared to adults. The procedure should be performed quickly and safely, and by a skillful pediatric endoscopy professional. Therefore, the choice of appropriate endoscopic ancillary device is very essential for rapid and safe removal of the FB. Some ancillary devices may be used with the permission of the health insurance system.
Previous studies on FBs in the UGI tract in children have focused on the type of FBs, age of the patients who ingested the FBs, and the type of management (surgical versus endoscopic removal).367 Few studies have been conducted on device selection and on the duration of the endoscopic removal procedures.
Therefore, the present study was undertaken to provide a description of the overall experience of endoscopic UGI FB removal in children, in real-world clinical settings, based on the experiences of four university hospitals actively performing gastrointestinal endoscopy in children and adolescents. We analyzed data while focusing on endoscopic techniques, including sedation type, duration of the endoscopic procedure, and the accessory devices used for the endoscopic removal in a conscious situation.
METHODS
We retrospectively analyzed the medical records of pediatric patients aged < 18 years who underwent UGI endoscopic FB removal, between January 2012 and August 2020, at four university hospitals (Chungbuk National University Hospital, CNUH; Gangneung Asan Hospital, GAH; Pusan National University Yangsan Hospital, PNUYH; and Jinju Gyeongsang National University Hospital, GNUH). The procedures were performed by seven pediatric endoscopists. Patients, diagnosed with gastrointestinal FB ingestion, who did not meet the indications for endoscopic removal were excluded from the study. Patients in whom the attempted endoscopic removal failed because of spontaneous passage were also excluded from the study.
Demographic data including age, sex, and body weight (kg) were collected. The patients were categorized into the following age groups: less than 1 year, 1–5 years, 6–10 years, and 11–18 years. Information regarding the types of FBs, the initial locations of the FBs (at the time of diagnosis), and the locations of the FBs at the time of removal, were recoded. We divided into two groups based on the body weight of 14.9 kg because the normal minimum body weight of a 5-year-old boy in Korea is 14.9 kg: less than 14.9 kg and greater than 14.9 kg.
Regarding the endoscopy data, the method of sedation, duration of the endoscopic procedure (minutes), and complications were investigated. As for duration of the endoscopic procedure, the beginning and end times of endoscopy were recorded in electronic medical records, and the time was calculated and recorded. The types of accessory devices used for retrieving the FBs (forceps, retrieval net, snare, or others) were also reviewed.
We conducted additional analyses focusing on the type of device used. We selected cases wherein both forceps and retrieval nets could be used (based on the type and shape of the FB) and analyzed the procedure duration according to the location of the FB and the devices used for the retrieval. In this analysis, FBs located above the esophagus or below the stomach were excluded. Cases wherein a retrieval net was used in the esophagus were excluded. Cases wherein multiple devices were used or multiple FBs were present (in multiple organs) were also excluded from this analysis.
Statistical analyses were conducted using frequency and analysis of variance tests in the Statistical Analysis Software (version 9.4; SAS Institute, Inc., NC, USA). Statistically significant differences were reported when the P values were below 0.05.
Ethics statement
The study protocol was approved by the Institutional Review Boards of GNUH (2020-10-002), CNUH (2022-04-017), GAH (2020-12-011), and PNUYH (05-2020-210). This was a retrospective study of medical records; thus, the requirement of informed consent from individual participants was waived.
RESULTS
Patients’ characteristics
A total of 424 children aged between 6 months and 18 years underwent UGI endoscopic FB removal during our study period (Table 1). There were 265 (62.5%) from PNUYH, 76 (17.9%) from CNUH, 52 (12.3%) from GNUH, and 31 (7.3%) from GAH. They included 277 male (65.3%) and 147 female (34.7%) patients. The mean age of the patients was 4.1 ± 3.7 years, 65 (15.3%) were aged ≤ 1 year and 304 (71.7%) were ≤ 5 years old. The mean body weight was 18.3 ± 11.9 kg (median: 14.9 kg).
Table 1
Demographic data, conscious sedation methods, the type of FBs, and the used endoscopic devices of children who underwent endoscopic FBs removal
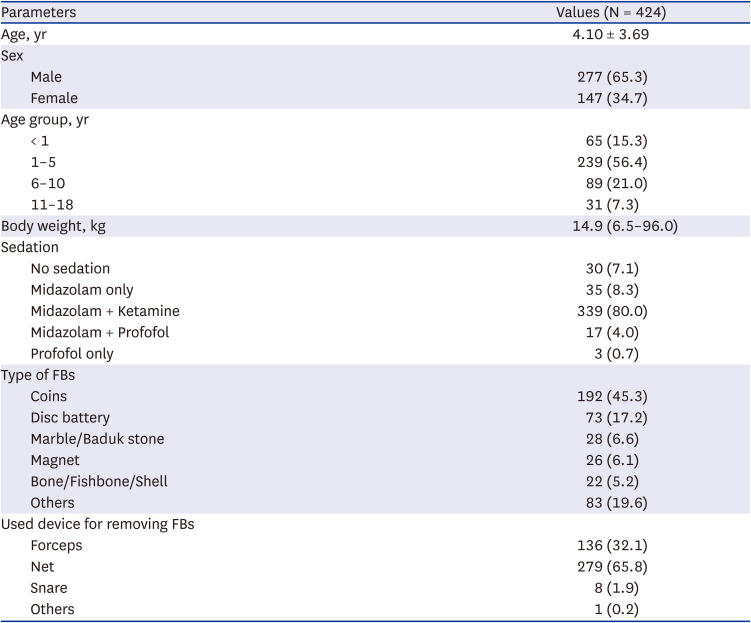
Three hundred ninety-four (92.9%) procedures were performed under sedation (Table 1). Midazolam was used in 391 (92.2%) procedures, and 339 (80.0%) endoscopies were performed under conscious sedation using midazolam and ketamine. Thirty-five patients (8.3%) were sedated with midazolam alone, while 20 procedures were performed using propofol with or without midazolam.
Coins were the most common FBs requiring removal, accounting for 192 cases (45.3%); disc batteries, marble/baduk stone, and magnets followed in 73 (17.2%), 28 (6.6%), and 26 (6.1%) patients, respectively (Table 1). The most common initial locations of the FB were the esophagus (45.8%) and stomach (48.3%), and they corresponded to the most common removal sites (25.5% and 69.5%, respectively) (Table 2). Disc batteries were the most common FB in children aged < 1 year (40.0%), and the second most common in children aged between 1–5 years (17.6%) (Table 3).
Table 2
Location of the foreign body during endoscopy
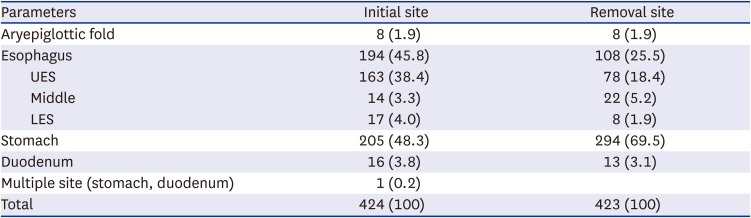
Table 3
Proportion of foreign bodies identified and procedure duration in different age groups

Endoscopic FB removal procedures
The retrieval net (65.8%) was the most commonly used device (for endoscopic FB removal in the children), followed by forceps (32.1%). The retrieval net was the most frequently used device in children aged below 10 years, while forceps (51.6%) were the most frequently used devices in children aged above 10 years (Table 4). There were no significant differences between the different institutions, regarding the device used.
Table 4
Proportion of foreign body retrieval procedures performed using the different devices in different age groups

The average duration of the FB removal procedure was 6.5 ± 7.3 minutes; the average durations in the less than 1 year, 1–5 years, 6–10 years, and 11–18 years groups were 5.2 ± 6.6, 6.3 ± 7.1, 7.0 ± 8.1, and 8.7 ± 8.4 minutes, respectively (the differences were not statistically significant, P = 0.154). Two hundred and seventy-three (64.4%) procedures were conducted within 5 minutes.
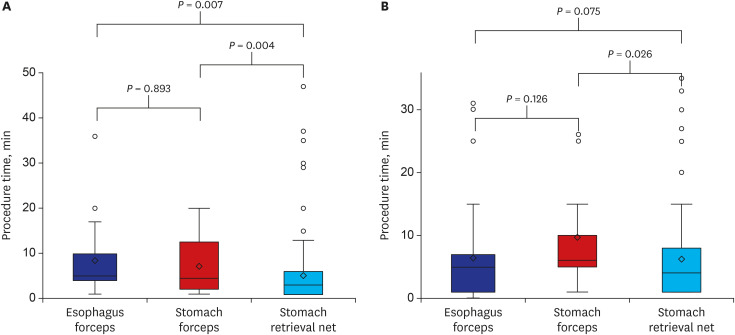
In 371 cases, both forceps and retrieval nets were used. The procedure duration for the endoscopic removal of gastric FBs using the retrieval net was the shortest (5.7 ± 7.3 minutes, P = 0.003) (Table 5). In the post hoc test, the procedure duration was significantly shorter when the net was used for gastric FBs than when forceps were used for esophageal or gastric FBs (P = 0.011 and P = 0.008). This difference was more significant in the group of patients weighing less than 14.9 kg (n = 188, P = 0.007); however, no significant difference was found in the large body weight group (≥ 14.9 kg) (n = 183, P = 0.075) (Fig. 1). In the lower body weight group, the procedure duration for retrieving gastric FBs using nets was significantly shorter than the procedure durations for retrieving gastric and esophageal FBs using forceps (P = 0.004) (Fig. 1). In the larger body weight group, the procedure duration for retrieving gastric FBs using retrieval nets was also shorter than when forceps were used for FBs in the same location (P = 0.026); however, it did not differ from the time taken to retrieve esophageal FBs using forceps (P = 0.075) (Fig. 1). When multivariate analysis was performed on the type of device used and the shape and maximum diameter of the FBs, the procedure duration was significantly shorter when the retrieval net was used in the group weighing less than 14.9 kg (P = 0.047).
Table 5
Endoscopic retrieval procedure duration according to location and device when both tools were clinically available (n = 371)

Fig. 1
Procedure duration for endoscopic FB removal according to the locations of the FB and devices used when both tools were clinically available (n = 371). (A) Lower body weight group (less than 14.9 kg, n = 188) showed significant shorter procedure duration for gastric FBs retrieval using retrieval nets than for gastric and esophageal FBs retrieval using forceps (P = 0.005 and P = 0.008, respectively). (B) Larger body weight group (more than 14.9 kg, n = 183) also showed shorter procedure duration during retrieval using retrieval nets than during retrieval using forceps (P = 0.026).
FB = foreign body.
There were no reported complications related to the FB removal procedures, except for one patient in whom the procedure failed.
DISCUSSION
In the present study, we retrospectively analyzed the duration of the procedures (according to the location of the FBs, type of FBs, and age and body weight of children) when using each of the ancillary devices used in removing FBs in children. The records were taken from four institutions, from January 2012 to August 2020. All the patients underwent the endoscopic FB removal procedure, with or without conscious sedation, but were not under general anesthesia. Previous studies on pediatric FB ingestion have focused on age, location of the FB, presenting symptoms, type and size of FB, and therapeutic modalities of the FB removal (endoscopic and surgical).89 In the present study, we determined which device was more efficient in removing these FBs in children. Our results showed that successful endoscopic removal of the FBs was achieved in 64.4% of patients within 5 minutes (in an average of 6.5 ± 7.3 minutes), and that the retrieval net was the most suitable device for this procedure, especially for gastric FBs. The average time taken to remove the FBs was shorter when using the retrieval net (2.8 minutes) than the time taken when using forceps.
Children’s characteristics such as age and weight vary according to the type and size of the ingested FBs. Additionally, the endoscopic removal of FBs is more difficult in young children than in adults. It is important for both patients and doctors to remove UGI FBs quickly and safely. In a Korean report, most children with FB ingestion were managed under conscious sedation (89.0%), and only 0.9% among them were managed under general anesthesia.10 However, in the present study, 92.9% of cases underwent endoscopic FB removal under conscious sedation, and none was managed under general anesthesia. Pediatric endoscopy for the removal of UGI FB should be performed in an appropriate environment, using ancillary endoscopic equipment for children, and by an experienced pediatric endoscopist.25 In smaller pediatric patients or those with a narrower esophageal lumen, small rubber-tipped or V-shaped forceps, or small alligator forceps, can be passed through the channel of an endoscope with a 2.0-mm channel.3
Young children (aged between 6 months and 3 years) occasionally accidentally ingest common objects found in the home environment, such as coins, disc batteries, and magnets.8911 As in previous studies,23 we found that coins were the most commonly ingested FBs (45.3%), followed by disc batteries, in our general study population. However, disc batteries were the most common (40.0%) FBs in children under 1 year of age.
We analyzed the relationship between the location of the FB and the time of removal. At the time of diagnosis, the FBs were located in the esophagus and stomach in 45.8% and 48.8% of cases, respectively. However, 25.5% and 69.5% of the FBs were removed from the esophagus and stomach, respectively. The difference between the initial location and the removal location resulted from the endoscopists pushing some of the FBs into the stomach, because the narrowness of the esophagus in children hindered the removal of the FBs in these cases. If the FB was initially located in the esophagus and removed from the stomach after pushing it, it was analyzed as an esophagus. To remove FBs in the esophagus, opened forceps should approach the FBs at a 90-degree angle to catch. In children, the angle at which the forceps can catch the FB is not easily controlled because of the narrow esophageal diameter and the mass effect caused by the FBs on the esophagus. Unlike during general anesthesia, patients can respond and move during endoscopy under conscious sedation. Therefore, esophageal FB retrieval cannot be easily performed when a young child moves under conscious sedation. Technically, the push technique is a method of gently pushing foreign objects directly through the endoscopy to the stomach and pulling FB in the stomach. These push techniques are successfully used in many smooth margined foreign substances.12 The time required for the push technique is usually similar to inserting an endoscope from the esophagus to the stomach.12
To retrieve esophageal coins or disc batteries, forceps such as alligator forceps or other forceps with the “rat-tooth configuration” (Raptor forceps; US Endoscopy, Mentor, OH, USA) are recommended, because the “rat tooth” end of the forceps can often successfully grasp the step-off between the two poles of the battery for removal.13 Alternatively, a retrieval net (Roth net; US Endoscopy) may also be effective.13 Roth retrieval nets are useful for the retrieval of round and smooth FBs,13 while polypectomy snares are useful for the removal of long objects that do not slip out of the snare.313 Gastric coins are usually located in the most dependent position of the stomach, which is usually the gastric cardia (when the patients are in the supine position). The retroflexed position of the endoscope may increase the difficulty in retrieving FBs. This is because when the forceps are straightened from the “J” position, dropping of the coin or FB may occur.3 Roth nets are most often successful because there are little chances for the FBs to leak.13 In the present study, for the removal of disc batteries in infants, a retrieval net was the most commonly used device (75.4%). Our results showed that the Roth retrieval net is a suitable device for the retrieval of FB in the stomach, in young and small children (Fig. 2).
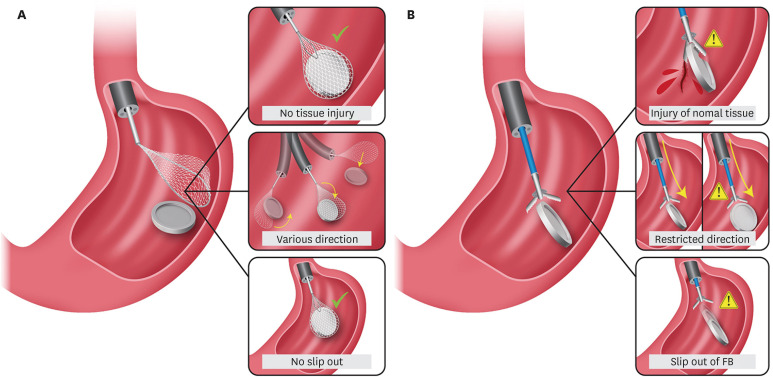
Fig. 2
Summarized illustration for endoscopic foreign body removal with retrieval net (A) versus with forceps (B). Roth net are most often successful because there are little chances for the FBs to slip out.
FB = foreign body.
Endoscopic accessories were chosen based on trials performed on prototypes of the ingested FB and also based on the preference of the endoscopist. Long objects may be securely grasped with a snare or a basket, whereas smaller or round objects may be better captured using a retrieval net.13 Small and flat objects, such as coins, are often securely grasped by forceps with longer jaws or “teeth” at the end (such as alligator, rat-tooth, or shark-tooth forceps).13 Rat-tooth forceps, Roth retrieval net, and polypectomy snares are commonly used forceps.2 Balekuduru et al.2 reported that all coins were removed using Roth nets or forceps, except for 15 cases where the coin passed out spontaneously.
The present study has several limitations. First, device selection might be related to insurance coverage and operator preference; however, these aspects were excluded from the analysis. Second, this study was also limited by the fact that we retrospectively analyzed medical records.
In conclusion, our results showed that successful endoscopic FB removal was achieved within an average of 5 minutes, and the retrieval net was the most suitable device for the removal of gastric FBs in children. Therefore, the retrieval net is a useful endoscopic ancillary device for quick and safe removal of gastric FBs in young children.
 XML Download
XML Download