

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Dementia remains one of the biggest public health diseases in the aging society. In Korea, the population with dementia is expected to cross 3 million in 2050.1 In 2016, the dementia prevalence ratio was 2.02 times higher than that in 2008, based on hospital utilization data.2 The cost of dementia management worldwide was expected to reach about $1 trillion in 2018 and is estimated to reach $2 trillion by 2030, with cost estimates in Korea showing a similar growth trend.3
Given the lack of effective treatments for dementia, identifying modifiable risk factors is crucial. It is also necessary to prevent increasing medical costs and reduce family and social burdens by managing modifiable factors, not genetic factors such as apolipoprotein E. The Lancet Committee reported 12 modifiable risk factors for dementia in 2020, including cardiovascular-related factors such as hypertension, diabetes, obesity and smoking.4
Traditional cardiovascular risk factors such as hypertension, diabetes, dyslipidemia, obesity, and smoking have been associated with rapid cognitive decline respectively.56 However, cardiovascular risk factors are interrelated,78 and it is difficult to isolate their individual effects on cognitive decline. A composite score is required to evaluate the cardiovascular risk comprehensively. The Framingham score is commonly used to evaluate cardiovascular risk burden and risk of developing cardiovascular diseases because it also integrates demographic and cardiovascular risk factors.9
Framingham scores and cognitive functioning are related.101112131415161718 Two studies that enrolled individuals with Alzheimer’s dementia and mild cognitive impairment showed that the Framingham score was positively correlated with the rate of cognitive decline.1617 A study conducted in Korea showed that Framingham scores and cognitive decline were positively correlated among elderly women.18
However, the Framingham scores consistently overestimate cardiovascular risk, especially among Asian populations.19
–
21 The Korean coronary heart disease risk score (KRS) was developed to measure cardiovascular risk among Korean populations more accurately.21 In this study, we examined the association between cardiovascular risk, as measured using KRS and global cognitive function in dementia-free Korean older adults.
METHODS
Study sample
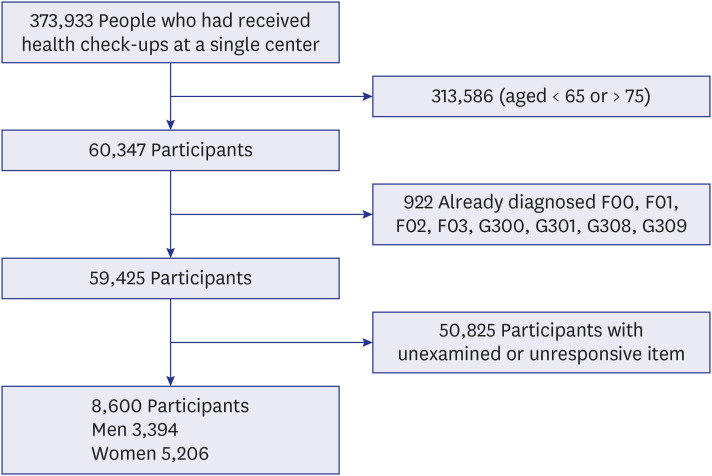
This cross-sectional study was conducted using data of 373,933 Koreans aged 30–95 years old who underwent at least one biennial National Health Insurance Service (NHIS) medical evaluation between 2015 and 2020 at a single hospital. Data were extracted of individuals aged between 65–75 years (n = 60,347). From this sample, data of those with dementia, defined as having International Classification of Diseases 10th Revision diagnostic codes of F00, F01, F02, F03, G309, G300, G301, or G308 (n = 922); for whom data about cognitive function was missing (n = 45,880); and whose KRS data were missing (n = 4,945) were excluded. Finally, data from 8,600 individuals were included in the final analysis (Fig. 1).
Data collection
The biennial NHIS medical evaluation consisted of a self-reporting questionnaire, physical assessment, and laboratory tests. Each individual was instructed to rest for five minutes, and their blood pressure was measured in the sitting position with automatic blood pressure monitoring equipment. They rested again for five minutes, and their blood pressure was measured again. Their height and weight were measured using an automatic scale while wearing a light gown after fasting starting from midnight. Smoking habits were categorized as never smoked, former smoker, or currently smoking. Alcohol consumption was calculated in grams of alcohol consumed per day.22 Total weekly metabolic equivalents (MET) were calculated based on the number of days in which the person engaged in moderate- or high-intensity exercise and the durations for such activities.23 Hypertension was defined as a systolic blood pressure (SBP) of 140 mmHg or higher, a diastolic blood pressure (DBP) of 90 mmHg or higher, or if the person consumed antihypertensive medication. Diabetes was defined as a fasting blood sugar of 126 mg/dL or higher or if the person used diabetes medication. Dyslipidemia was classified as a total cholesterol level of 240 mg/dL or higher or if the person used dyslipidemia medication. Stroke, coronary heart disease, hypertension, diabetes, dyslipidemia, past tuberculosis and medication histories were assessed using questionnaires. Blood samples were taken, including lipid profiles. Cognitive function was ascertained using the Korean Dementia Screening Questionnaire-Cognition (KDSQ-C). Missing total cholesterol and high-density lipoprotein (HDL) cholesterol data were imputated using data within the preceding 5 years.
KRS
The KRS was developed based on the data of 268,315 individuals who were examined in the multicenter health check-up. The KRS is based on sex, age, SBP, DBP, total cholesterol, HDL cholesterol, smoking status, and diabetes history.21 The areas under the receiver operating characteristic (ROC) curve were 0.764 for men and 0.812 for women.21
When calculating KRS, blood pressure was classified according to the 7th Guidelines of the Joint National Committee on Hypertension.24 Total cholesterol was categorized as less than 160, 160–199, 200–239, 240–279, and more than 280 mg/dL. HDL cholesterol was categorized as less than 35, 35–44, 45–49, 50–59, and more than 60 mg/dL.21 KRS was categorized as 0–2%, 2–4%, or more than 4% likelihood of a coronary heart disease event occurring in the next 10 years, corresponding to lowest, middle, and highest, respectively.25 A higher KRS indicates a higher current cardiovascular burden and greater risk of a coronary disease event occurring within the next 10 years.
The KDSQ-C
The KDSQ-C is a standard tool for the early diagnosis of dementia. It is a structured questionnaire that includes 15 questions assessing memory impairment, other cognitive impairments, and instrumental activities of daily living. Each question can be responded to with either “No”, “Sometimes (a little bit) yes”, and “often (a lot) yes”, which receive 0, 1, and 2 points, respectively, for a possible total score of 30 points.
The KDSQ-C is administered as part of biennial NHIS medical examinations starting at the age of 66.26 It is not affected by patient or caregiver age, sex, or educational background. None of the items are related to the ability to read or write, making it effective for screening for dementia among those with low education levels.26 Higher scores reflect poorer cognitive function. Patients with scores ≥ 6 undergo additional tests for dementia diagnosis.27 With respect to dementia diagnosis, the KDSQ-C’s threshold of 6 points has a sensitivity of 79% and a specificity of 80%.27
Statistical analysis
The study sample’s baseline characteristics, identified using KRS, were compared using a Fisher’s exact test, a χ2 test for categorical variables, and a one-way analysis of variance (ANOVA) for continuous variables. Logistic regression analysis was used to estimate the odds ratio (OR) and 95% confidence intervals (CIs) for the associations between cardiovascular risk and cognitive function. Considering the repeated measurement of the same subject, the generalized estimation equation method was used.
Weight, height, stroke history, coronary heart disease history, alcohol consumption, and physical activity engagement were adjusted. The statistical analyses were conducted using SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA). P values of less than 0.05 were considered statistically significant.
Ethics statement
The study was approved by the Institutional Review Board of the National Health Insurance Medical Center (IRB No. 2021-05-004). The requirement for obtaining informed consent was waived because of the retrospective study. This study was conducted in accordance with the ethical principles of the declaration of Helsinki.
RESULTS
Epidemiological data are shown in Table 1. Of the 8,600 individuals included in the final analysis, 5,206 were men, and 3,374 were women. Their average age was 69.74 ± 3.1 years. There were 5,923 (68.9%) individuals in the lowest KRS group, 2,343 (27.2%) in the middle group, and 334 (3.9%) in the highest group. The average KDSQ-C score was 2.96 ± 3.10 points. There were 1,425 (16.6%) individuals with a KDSQ-C score of 6 or higher, while 7,175 (83.4%) others had scores below this level. Smoking status, stroke history, and coronary heart disease history were significantly correlated with KRS in all participants.
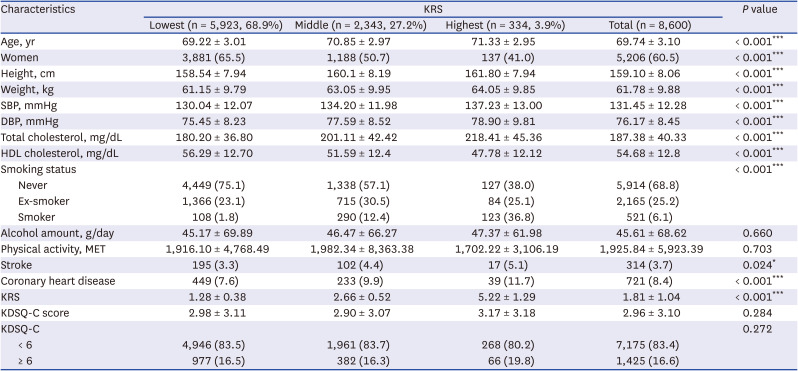
Table 1
Demographic characteristics of the subject by KRS group (n = 8,600)
P values are from χ2 test, Fisher’s exact test or one-way ANOVA; categorical variable: number (percentage), continuous variable: mean ± standard deviation.
KRS = Korean coronary heart disease risk score, SBP = systolic blood pressure, DBP = diastolic blood pressure, HDL = high-density lipoprotein, MET = metabolic equivalents, KDSQ-C = Korean Dementia Screening Questionnaire-Cognition, ANOVA = analysis of variance.
Statistically significant P values were marked with asterisks *P < 0.05 **P < 0.01, ***P < 0.001.
![]()
Tables 2 and 3 display the demographic characteristics of men and women, respectively, by KRS group. More women (74.6%) were in the lowest KRS group than men (60.2%). Conversely, more men were in the highest KRS group (5.8%) than women (2.6%). There were fewer men (13.7%) with a KDSQ-C of 6 or higher than women (18.4%).
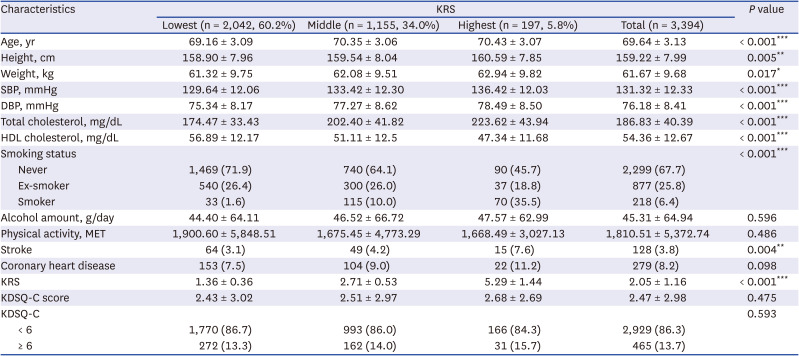
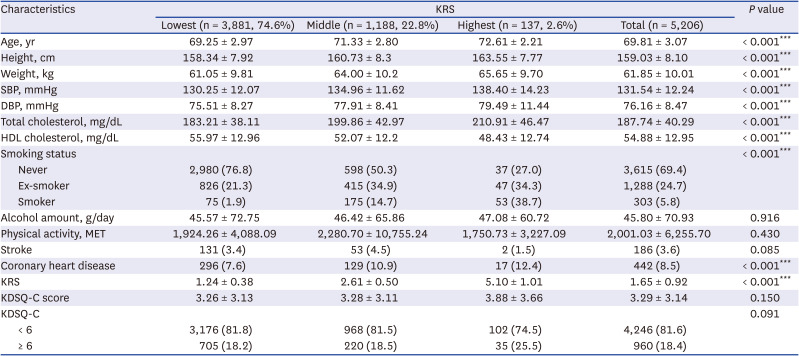
Table 2
Characteristics of men with cardiovascular risk (n = 3,394)
P values are from χ2 test, Fisher’s exact test or one-way ANOVA; categorical variable: number(percentage), continuous variable: mean ± standard deviation.
KRS = Korean coronary heart disease risk score, SBP = systolic blood pressure, DBP = diastolic blood pressure, HDL = high-density lipoprotein, MET = metabolic equivalents, KDSQ-C = Korean Dementia Screening Questionnaire-Cognition, ANOVA = analysis of variance.
Statistically significant P values were marked with asterisks (*P < 0.05 **P < 0.01, ***P < 0.001).
![]()
Table 3
Characteristics of women with cardiovascular risk (n = 5,206)
P values are from χ2 test, Fisher's exact test or one-way ANOVA; categorical variable: number(percentage), continuous variable: mean ± standard deviation.
KRS = Korean coronary heart disease risk score, SBP = systolic blood pressure, DBP = diastolic blood pressure, HDL = high-density lipoprotein, MET = metabolic equivalents, KDSQ-C = Korean Dementia Screening Questionnaire-Cognition, ANOVA = analysis of variance.
Statistically significant P values were marked with asterisks (*P < 0.05 **P < 0.01, ***P < 0.001).
![]()
Smoking status was significantly associated with KRS in both men and women. Stroke history in men and coronary heart disease history in women were significantly associated with KRS. In age subgroup analysis for men, significant differences were observed in SBP, DBP, total cholesterol, HDL cholesterol, and smoking status. No significant difference was observed in alcohol consumption, physical activity, or coronary heart disease history (Supplementary Tables 1 and 2). The female age subgroup analysis also showed differences similar to the men’s subgroup study (Supplementary Tables 3 and 4).
Relationship between KRS and cognitive function
The odds ratios of cognitive function according to KRS group are shown in Table 4. The lowest KRS group was used as the reference. Compared with the lowest group of KRS in all subjects, the highest KRS group in all participants was associated with cognitive decline, as shown in Table 4 (OR, 1.339; 95% CI, 1.034–1.734; P = 0.005). Among women, the highest KRS group was 1.629 times more likely to experience cognitive decline than the lowest risk group (OR, 1.629; 95% CI, 1.144–2.319; P = 0.004).
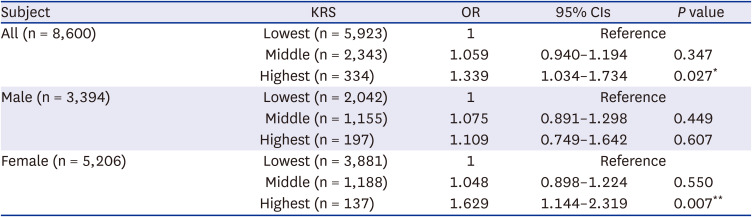
Table 4
OR and 95% CIs for cognitive function by KRS group
Adjusted for height, weight, alcohol amount, physical activity, sex (only in all subjects), stroke, coronary heart disease.
OR = odds ratio, CI = confidence interval, KRS = Korean coronary heart disease risk score.
Statistically significant P values were marked with asterisks (*P < 0.05 **P < 0.01, ***P < 0.001).
![]()
Tables 5 and 6 summarize the correlations between the KRS group and KDSQ-C scores by age subgroup. There were no statistically significant correlations between the KRS group and cognitive function among 65–70-year-olds. Among 71–75-year-olds, women in the highest KRS group were 1.595 times more likely to be experiencing cognitive decline than the lowest KRS group (OR, 1.595; 95% CI, 1.045–2.434; P = 0.031). These results indicate that reducing cardiovascular disease risk among the older adults, especially older women, is important for healthy brain aging.
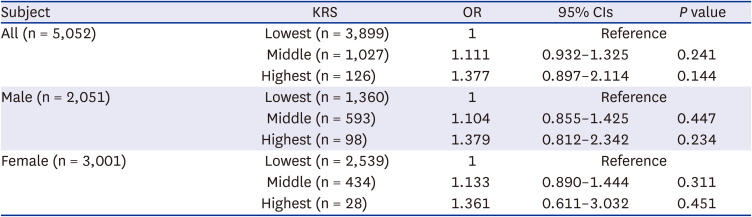
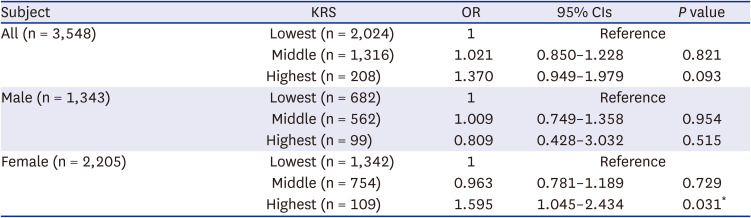
Table 5
OR and 95% CIs for cognitive function by KRS group among 65–70-year-olds
Adjusted for height, weight, alcohol amount, physical activity, sex (only in all subjects), stroke, coronary heart disease.
OR = odds ratio, CI = confidence interval, KRS = Korean coronary heart disease risk score.
Statistically significant P values were marked with asterisks (*P < 0.05 **P < 0.01, ***P < 0.001).
![]()
Table 6
ORs and 95% CIs for cognitive function by KRS group among 71–75-year-olds
Adjusted for height, weight, alcohol amount, physical activity, sex (only in all subjects), stroke, coronary heart disease.
OR = odds ratio, CI = confidence interval, KRS = Korean coronary heart disease risk score.
Statistically significant P values were marked with asterisks (*P < 0.05 **P < 0.01, ***P < 0.001).
![]()
DISCUSSION
This study examined the relationship between cardiovascular risk and cognitive function among non-demented Korean older adults between the ages of 65 and 75. Our study revealed that as cardiovascular risk increased, the odds ratio increased across all participants; however, this relationship was strong among older women.
In previous studies, cardiovascular risk as assessed by Framingham score was positively correlated with cognitive decline.1011121314151617 One study showed that individuals with high Framingham scores rapidly progressed from mild cognitive impairment to dementia.16 Also, a higher vascular risk factor index was related to cognitive decline.28
One study found that the Framingham score was positively correlated with the speed of the decline in global cognition, episodic memory, working memory, and perceptual speed.10 In Korea, individuals with metabolic syndromes, namely abdominal obesity, hypertriglyceridemia, low HDL cholesterol, hypertension, and diabetes, have been found to have lower cognitive function scores compared to others.2930 This study was conducted on individuals who had undergone NHIS medical examinations. The study used a cardiovascular risk assessment model tailored for Koreans.
There are several neuroimaging studies explaining cerebrovascular changes in case of high cardiovascular risk.103132 Changes in the hippocampus, gray matter, and cerebral white matter of dementia-free older adults with high cardiovascular risks have been observed in brain magnetic resonance imaging scans. Reduced hippocampus and gray matter volume indicate the presence of Alzheimer’s dementia, which is associated with neurodegeneration. White matter hyperintensity refers to microvascular lesions in the cerebral white matter. Cardiovascular risk has been found to be positively correlated with neuronal degeneration and vascular changes.10
One study reported that the Framingham score was positively correlated with the β-amyloid burden of Pittsburgh compound Positron emission tomography. High cardiovascular risk and high β-amyloid burden cause synergistic effects and lead to decreased cognitive function scores.31 A study involving older adults with normal cognitive function showed that β–amyloid accumulation was negatively correlated with cerebrovascular responses.32
Some pathophysiological pathways may explain the correlations observed in this study. Cardiovascular risk factors can lead to systemic subclinical atherosclerosis or arteriosclerosis, affecting the heart, brain, and peripheral blood vessels by inducing inflammation and oxidative stress. These effects can cause silent cerebral hypoperfusion, hypoxia, and inflammatory injury, which can ultimately cause cognitive decline.33
The influence of cardiovascular risk factors on cognitive decline differs by sex. The correlation between the Framingham scores and cognitive function, defined in terms of global cognition, verbal fluency, and long-term recall, was stronger in women than in men.34 Analyzing the interaction between sex and KRS revealed that an interaction existed because the ORs are high in females (based on the lowest male, ORs of 2.206 [95% CI, 1.467–3.317] of the female highest group). While interpreting the results of this study, it is necessary to consider the sex-specific differences. Previous studies reported that depression and hearing loss were significantly associated with cognitive impairment among both sexes.3536 Having a limitation in performing the instrumental activities of daily living was significant associated with cognitive decline only among Korean older women. In contrast, a limitation in performing activities of daily living was significantly related to cognitive decline among men.35 In order to prevent cognitive decline, it is necessary to manage depression more thoroughly along with the control of cardiovascular risk factors in Korean elderly. The use of hearing aids is recommended to control hearing loss and prevent cognitive decline simultaneously.36
The difference in the correlation between KRS and cognitive function by sex may be related to vascular physiology. Coronary microvascular and endothelial dysfunction is more common among women than among men because of its smaller arterial size and more vascular remodeling in women. The same mechanism can cause more microvascular damage in women’s brains, resulting in quiet cerebral infarction and hypoperfusion.3437 In cohort study conducted in China, older subjects had more association between high cardiovascular risk and worse calculation ability.37
The prevalence and cost of dementia management have increased significantly over the years. Modifiable factors for dementia prevention have received special attention because of the lack of effective treatments for dementia. The findings of this study suggest that optimal blood pressure and lipid levels, no smoking, and controlling diabetes may help promote healthy brain aging among dementia-free older adults, especially among older women.
One of this study’s strengths was that cardiovascular risk factors were reflected in the integrated KRS. It is important to understand individuals’ cardiovascular risk from the perspective of precision medicine. This study had three key limitations. The first was that it only used data from a single health center. Patients were classified as normal if diagnosed with dementia at another hospital and only examined at the health check-up. The second limitation was that education has also been reported to affect dementia status; however, due to the characteristics of the NHIS medical examination, education data were unavailable and were not included in this analysis. The third limitation was that this study was cross-sectional; subsequent cohort studies should examine the relationship between cardiovascular risk and cognitive decline. Furthermore, the neurocognitive effect of statins remains controversial, and we need to confirm it through follow-up studies.38
In conclusion, our study found that individuals with high cardiovascular risk had poorer cognitive function than those with low risk, especially older women. We recommend carefully managing cardiovascular risk factors to promote healthy mental aging in dementia-free elderly individuals.
 XML Download
XML Download