

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of dyslipidemia, a pivotal risk factor of atherosclerotic cardiovascular disease, is steadily increasing in East Asia, including Korea.1) Lipid-lowering therapy appropriate to individuals’ risk status is a mainstay of primary and secondary cardiovascular prevention.2) The rate of future cardiovascular events is not high in individuals with low to moderate cardiovascular risk. Absolute risk reduction by lipid-lowering pharmacotherapy is lower and the number needed to treat is higher in these groups than in higher risk groups. Accordingly, as the cost-effectiveness of pharmacotherapy is low, this is not strongly recommended in such individuals, unless they have substantially high low-density lipoprotein-cholesterol (LDL-C) levels.3)4)
Although not routinely recommended, carotid ultrasound can provide information on the presence and characteristics of plaques and grade of stenosis, which can be useful for cardiovascular prevention.5) As it is noninvasive and causes no radiation, carotid ultrasound is commonly used in clinical practice. With advances and frequent utilization of imaging techniques,6) cases exhibiting discrepancies between clinical risk assessment and imaging results can emerge. Furthermore, many physicians may be unfamiliar with concepts of carotid plaques and their burden. Therefore, in the presence of such discrepancies, it may be challenging for clinicians to decide whether to start lipid-lowering pharmacotherapy for cardiovascular prevention.
The risk of major adverse cardiac events has been reported to be incrementally higher according to the burden of carotid plaques,7) In a recent study, the presence of carotid plaques was associated with a 1.66-fold increased risk of coronary artery disease even when the coronary calcium score was 0.8) Based on these studies, the latest European guidelines consider carotid plaques as a risk modifier in low to moderate risk patient groups and classify individuals with carotid plaques into the very-high risk group.4) A few studies have shown statin benefit in patients with carotid artery atherosclerosis or stenosis. Most of the subjects included in these studies were statin-eligible according to current guidelines.9)10) However, there have been no studies evaluating the effect of statins in individuals with low to moderate cardiovascular risk but with carotid plaque. Therefore, it is unclear whether statin therapy provides clinical benefits in them.
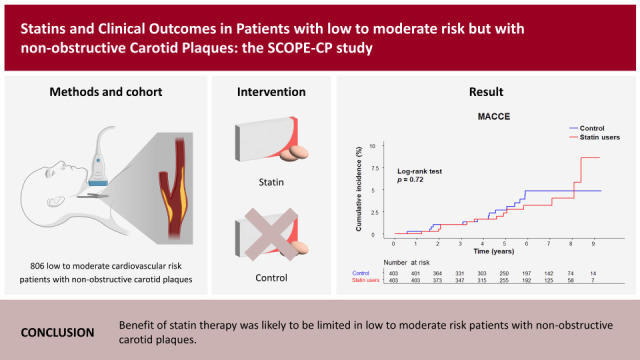
The aim of this study was to evaluate whether statin therapy provides clinical benefit in individuals with low to moderate cardiovascular risk who are not recommended for statins but possess non-obstructive carotid plaques. We classified risk groups based on clinical risk factors. Although this was a retrospective study, we minimized potential bias between the study groups by propensity score matching.
METHODS
The data supporting the findings of this study are available from the corresponding author upon reasonable request. The corresponding author had full access to all data in this study and takes responsibility for data integrity and data analyses.
Ethical statement
This study was approved by the Institutional Review Board of Severance Hospital, Seoul, Korea (4–2021-0304) and was conducted in accordance with the Declaration of Helsinki (2013). The requirement of informed consent was waived because this study was retrospective and the study population was de-identified after cohort creation according to strict confidentiality guidelines.
Study population
This was a retrospective propensity score matching study. We initially screened 12,158 consecutive patients aged ≥18 years who underwent carotid ultrasound between January 2012 and February 2020 at a single university hospital (Figure 1). Carotid ultrasound was performed in patients who visited the outpatient cardiology clinic. Carotid study was performed to check carotid artery for risk evaluation. Inclusion criteria were individuals with low or moderate cardiovascular risk defined by the 2018 guidelines of Korean Society of Lipid and Atherosclerosis3) with the presence of ≥1 non-obstructive carotid plaque on ultrasound. Exclusion criteria were individuals for whom pharmacological lipid-lowering therapy was highly recommended, such as very-high risk group (i.e., atherosclerotic cardiovascular disease), high risk group (i.e., diabetes mellitus, abdominal aortic aneurysm, or carotid artery stenosis), moderate risk group (i.e., ≥2 risk factors) with LDL-C ≥130 mg/dL, or low-risk group (i.e., 0–1 risk factors) with LDL-C ≥160 mg/dL; patients with chronic kidney disease (CKD, estimated glomerular filtration rate [eGFR] <60 mL/min/1.73 m2); and individuals with no laboratory data or previous statin use before carotid ultrasound. We also excluded patients with cross-over during the follow-up period, those with inconsistent statin prescription for <80% of the follow-up period, or follow-up duration <1 year. As in previous studies,11)12) a duration >80% of the follow-up period was regarded as consistent use. A total of 12,159 patients were initially screened and 8,935 had ≥1 carotid plaque and laboratory data. After excluding ineligible individuals, 1,611 (406 new statin users and 1,405 non-users) were enrolled in this study. After 1:1 propensity score matching, 403 new statin users and 403 controls were finally analyzed using clinical follow-up data until May 2021 (Figure 1). All patients received standard medical care at the discretion of the treating physicians and were followed up at outpatient clinics every 3–6 months.
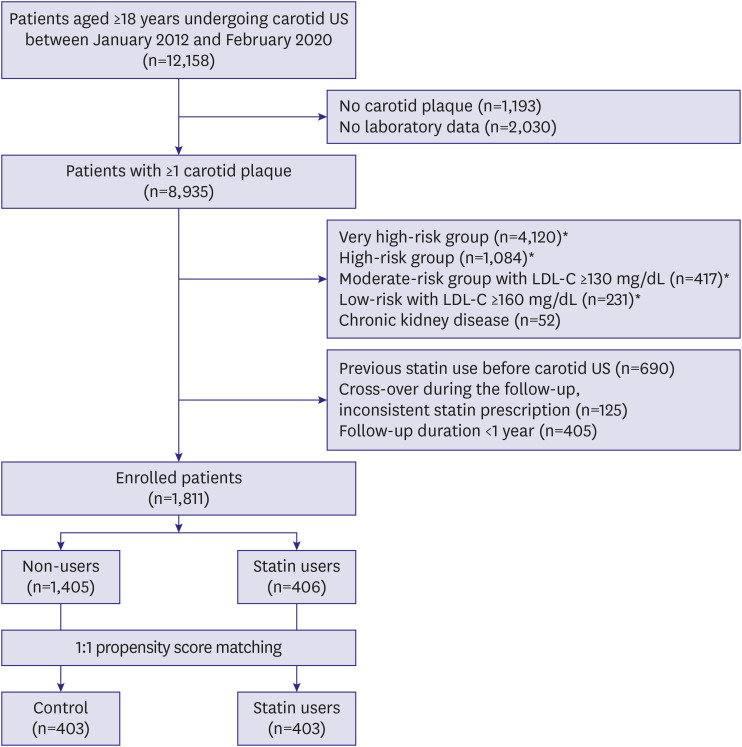
Figure 1
Patient enrollment flow.
LDL-C = low-density lipoprotein-cholesterol; US = ultrasound.
*Risk categories were based on the 2018 Korean Society of Lipid and Atherosclerosis guidelines for the management of dyslipidemia.3)
![]()
Carotid ultrasound
Carotid ultrasound scans were performed by trained sonographers using a specialized vascular ultrasonography device (Acuson X300; Siemens, Munich, Germany) or Acuson Juniper (Siemens). Both right and left carotid arteries were imaged using 2D transducer. Carotid artery plaques were defined as focal structures encroaching into the arterial lumen of ≥0.5 mm or 50% of the surrounding intima-media thickness or cases of diffuse vessel wall atherosclerosis with intima-media thickness >1.5 mm.13) The presence and thickness of carotid plaques were measured in both the right and left common, external, and internal carotid arteries, as well as the bulb area. The maximum carotid plaque thickness (cPTmax) was defined as the greatest thickness of the plaque from either side. Total number of plaques and cPTmax that have been used in recent studies14)15) were used as plaque parameters in the present study. Non-obstructive carotid plaques were defined as carotid plaques causing <50% lumen diameter narrowing.
Study protocol
We retrieved baseline demographic data, medical history, laboratory data, and medications from the medical records. Hypertension was defined as blood pressure ≥140/90 mmHg or use of antihypertensive agents. Blood samples were collected after ≥8 hours fasting. Statin intensity was defined according to the 2018 American College of Cardiology/American Heart Association guidelines.16) Because most patients in our study were prescribed moderate intensity statin, moderate intensity statins were divided into 2 groups: atorvastatin 20 mg or similar statins as high moderate intensity, and atorvastatin 10 mg or similar statins as low moderate intensity.
Primary outcome variables were major adverse cardiovascular and cerebrovascular events (MACCEs) and all-cause mortality. MACCE was defined as the composite of cardiovascular death, nonfatal myocardial infarction (MI), coronary revascularization, and nonfatal stroke or transient ischemic attack (TIA). Secondary outcome variables were individual components of MACCEs. Dates and causes of death were obtained from the Korean Statistical Information Service and Microdata Integrated Service managed by Statistics Korea, a government agency, as previously reported.17)18) MACCE data were collected from electronic hospital record review.
Statistical analysis
Categorical variables are reported as frequencies (percentages). Continuous variables are expressed as mean ± standard deviation or median (interquartile range). The categorical variables were compared using Fisher’s exact test or the Pearson χ2 test, and continuous variables were compared using Student’s t-test.
We performed 1:1 propensity score matching to reduce the effect of selection bias and potential confounders using the nearest neighbor method with a caliper of 0.1. The following variables were used for matching: age, sex, obesity, hypertension, eGFR, LDL-C, number of carotid plaque, cPTmax, number of antihypertensive agents, and use of antiplatelet agents. Standardized mean difference of <10% for the variables indicated appropriate propensity score matching. The rate of adverse outcomes was calculated by dividing the number of events by person-time at risk and presented as the incidence/1,000 person-years. Cumulative incidences of adverse outcomes were depicted using Kaplan-Meier curves and compared across the groups using the log-rank test. Using Cox proportional hazard regression, we analyzed the hazard ratios (HRs) and 95% confidence intervals (CIs) for adverse outcomes. Main regression models were adjusted for clinical variables including age, sex, and smoking. We conducted subgroup analyses for adverse outcomes stratified by age, sex, and other baseline variables. Interaction tests were performed for all subgroups. In sensitivity analysis, first, we conducted analyses for 1,811 patients before propensity score matching. Second, we performed analyses by only excluding patients with very high-risk group and high-risk group. Patients with moderate-risk group, low-risk group, and CKD remained in enrolled process, and propensity score matching was performed.
All tests were 2-tailed, and p values <0.05 were considered statistically significant. Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA) and R programming version 4.0.2 (The R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Baseline characteristics
The baseline characteristics of study population before and after propensity score matching are presented in Table 1. Variables did not differ between the statin and control groups after matching. The mean age was 62.4±11.2 years old, and 48.8% of the participants were male. About half of the study population in each patient group was at moderate risk. The median baseline LDL-C levels were 105 and 102 mg/dL in the control and statin groups, respectively. The median number of plaques was 3 and median cPTmax was 2.1. In the statin group, patients received low moderate intensity-, high moderate intensity-, and low intensity statins, in the order of frequency (Supplementary Figure 1). Atorvastatin, rosuvastatin, and pitavastatin were frequently used.
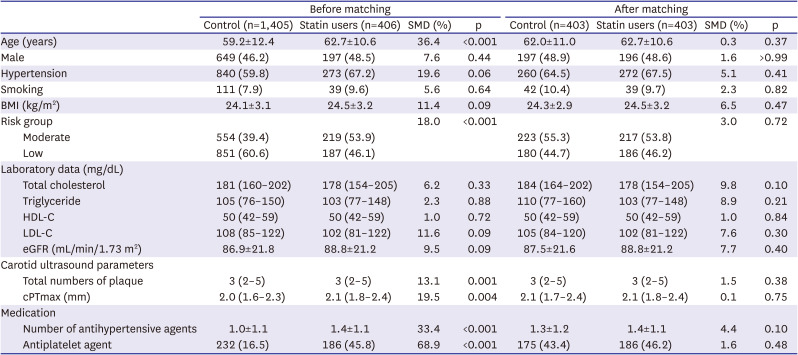
Table 1
Baseline characteristics of study population before and after propensity score matching
Values are expressed as mean ± standard deviation, median (interquartile range), or number (%).
BMI = body mass index; cPTmax = maximum carotid plaque thickness; eGFR = estimated glomerular filtration rate; HDL-C =high-density lipoprotein-cholesterol; LDL-C = low-density lipoprotein-cholesterol; SMD = standardized mean difference.
![]()
Clinical outcomes
During the median follow-up of 6.0 years, 14 (3.5%) and 13 (3.2%) patients experienced MACCEs in the control and statin groups, respectively (Table 2). The incidence of MACCEs did not differ between the groups (6.1 and 5.7/1,000 person-years, respectively; adjusted HR, 0.95; p=0.90). The events occurred in 8 out of 256 (3.1%) patients receiving low moderate intensity statins, and 4 out of 118 (3.9%) patients receiving high moderate intensity statins. The incidences of each component of MACCEs were all similar between the 2 groups. Nine individuals in each group died during the follow-up and the incidence of all-cause mortality did not differ between the groups (3.9 and 3.9/1,000 person-years, respectively, adjusted HR, 1.02; p=0.97). The Kaplan-Meier curves showed similar rates of MACCEs (log-rank p=0.72) and all-cause mortality (log-rank p=0.99) in statin users and controls (Figure 2).


Figure 2
Kaplan–Meier curves of the cumulative incidence of MACCE (A) and all-cause mortality (B) according to statin use.
MACCE = major adverse cardiovascular and cerebrovascular event.
![]()
Table 2
Risk of MACCE and all-cause mortality according to statin use
CI = confidence interval; HR = hazard ratio; MACCE = major adverse cardiovascular and cerebrovascular event; TIA = transient ischemic attack.
*The model was adjusted for age, sex, smoking.
![]()
Follow-up LDL data at 1 year were available for 309 (76.7%) patients in statin group, and 204 (50.6%) patients in control group due to retrospective design. The median follow-up LDL level was 103 (81–124) vs. 85 (69–108) mg/dL in the control and statin groups, showing significant difference (p<0.001).
Predictors of MACCE and subgroup analysis
In univariable analysis, age (HR, 1.06; p=0.007) and smoking (HR, 2.86; p=0.017) were associated with MACCEs (Table 3). Although the total number of plaques showed an HR of 1.10, it was not statistically significant (p=0.11). In multivariable analysis, age (HR, 1.06; p=0.011) and smoking (HR, 3.41; p=0.029) were identified as independent predictors of MACCEs. There was no subgroup in which statin provided differential impact on MACCEs (Supplementary Figure 2). Only individuals with HDL-C ≥50 mg/dL exhibited a tendency of statin benefit compared to the counterpart (p for interaction=0.059).
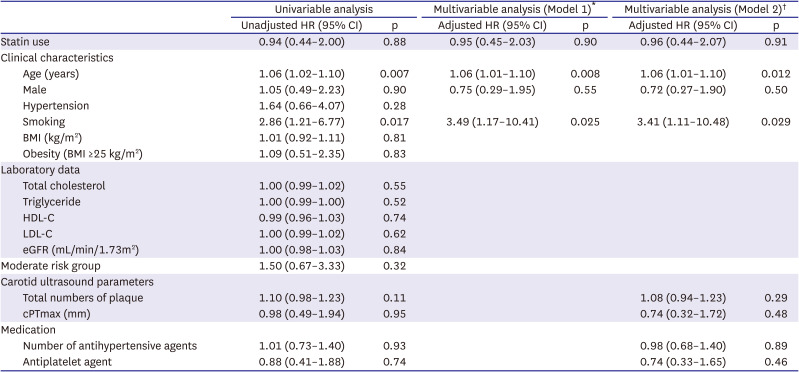
Table 3
Factors predictive of major adverse cardiovascular and cerebrovascular event identified by univariable and multivariable regression analyses
BMI = body mass index; CI = confidence interval; cPTmax = maximum carotid plaque thickness; eGFR = estimated glomerular filtration rate; HDL-C = how-density lipoprotein-cholesterol; HR = hazard ratio; LDL-C = low-density lipoprotein-cholesterol.
*Multivariable regression analysis was performed by using variables: age, sex, smoking, and statin use.
†Multivariable regression analysis was performed by using variables: age, sex, smoking, total number of carotid plaque, cPTmax, number of antihypertensive agents, antiplatelet agent and statin use.
![]()
Sensitivity analyses
The result of sensitivity analysis before propensity score matching (406 statin user, 1,405 controls) were consistent with the main analyses (log-rank p=0.78 for MACCE, 0.70 for all-cause death; Supplementary Figure 3). In addition, the result of sensitivity analysis only excluding patients with very high-risk group and high-risk group showed the similar results. (log-rank p=0.95 for MACCE, 0.92 for all-cause death; Supplementary Figure 4).
DISCUSSION
The main findings of the present study are as follows: cardiovascular outcomes were not different between statin users and controls in the study population with low to moderate cardiovascular risk and non-obstructive carotid plaques. In multivariable analyses, age and smoking were identified as predictors of worse outcomes. There was no subgroup that showed differential statin effects in analyses including carotid plaque indices. The present study provided evidence that benefit of statins is likely to be limited if any even when carotid plaques, a reported risk modifier, are present in low to moderate risk groups. These results may help physicians in clinical decision-making regarding cardiovascular prevention.
The presence and severity of carotid plaques have been reported as markers of future cardiovascular outcomes in several studies.7)8)15)19) However, no studies were conducted to investigate statin benefit in this population and ours is the first to evaluate the effect. The results of our study have several clinical implications. According to our findings, statin therapy may not be needed in low to moderate risk groups even when carotid plaques are present. In other words, it is reasonable to follow current lipid-lowering guidelines for the corresponding risk groups. In addition, the need for carotid ultrasound for guidance regarding pharmacotherapy in these groups is low because statin benefit was limited in the present study. Conversely, as age and smoking were predictive of adverse events, more active management of individuals with these factors is desirable.
The results of our study can be explained as follows: first, additive cardiovascular risk in individuals with carotid plaques may be clinically insignificant. In the present study, the estimated 10 years MACCE (cardiovascular death, nonfatal MI, coronary revascularization, nonfatal stroke or TIA) rate based on event rate (per 1,000 person-years) in our control group was 6.1%. Nevertheless, the estimated 10 years composite event rate used in pooled cohort equation (coronary death, nonfatal MI, or stroke) was only approximately 3.1% in our control group. Individuals with such a risk belong to the low risk group (i.e., 10-year risk <5%) according to the latest American lipid guidelines.16) In the HOPE-3 study that proved statin benefit in individuals with relatively low, “intermediate” risk group, the composite event (cardiovascular death, nonfatal MI, and nonfatal stroke) rate was 4.8% in the control group during a median follow-up of 5.6 years.20) This rate is much higher than that reported in the present study. In this regard, the actual risk of our study population might have been lower than that predicted by Korean guideline based assessment at enrollment. This could be a potential reason for the lack of statin benefit in our study. On the other hand, the lack of statin effect in the present study might have been influenced by the relatively small cohort assessed in of our study. However, masking of statin benefit due to this reason may not be high because the event rate in each group was very similar in our study.
Although the relationship between the presence of carotid plaques and stroke risk has been previously reported,15) it differed from the report of Mehta et al.8) In the present study, unadjusted and adjusted HRs of ischemic stroke or TIA, a component of MACCEs, were 0.58 and 0.49, respectively in the statin group. These rates are the numerically lowest HRs of all MACCE components. However, since the rates are 4 and 2 (1.7 and 0.9/1,000 person-years) in controls and statin users, respectively, they are too small to confirm statin benefit. Further studies are required to clarify potential benefits of statins benefit on stroke risk in this population.
Our study has a few limitations. We used the total number of carotid plaques and cPTmax. However, with further quantified or quality-related plaque indices, such as plaque type, and select test population based on these, we cannot preclude that stain benefit can be shown. Although some studies use magnetic resonance images or 3-dimensional data in patients with carotid plaques, this information was not available for our patients. In addition, we did not have sufficient data regarding follow-up lipid parameters and drug adverse events. Most available follow-up LDL-C data were from the 1-year follow-up time point, and the proportion of missing data was high. Therefore, there was limitation in analyzing the impact of LDL-C reduction on cardiovascular events in the present study. These data might have enabled more detailed evaluation of clinical benefit. Furthermore, we chose 2 study groups by propensity score matching. However, the retrospective nature of our study has the limitation of potential differences in baseline characteristics between the 2 groups. Conversely, estimation of future event risk and power calculation was difficult, as the study population meeting our inclusion criteria might not fit in widely used risk grouping. Therefore, we enrolled study subjects as much as possible for the present study. Furthermore, we considered the duration of statin prescription as the period of drug coverage. However, the compliance of patients was not exactly assessed in our study setting, and there could be a case of inconsistent statin use or stopping statin during follow-up period, which could be potential bias in our study, although we tried to maximally exclude patients who had inconsistent statin use. Routine Carotid study was performed in patients with low to moderate risk. However, the mean age of study population was >60 years and more than half of them were hypertensive. These indicate that individuals with lower risk level in the low risk group such as the young or those without any risk factor were quite rare in our subjects. The study population was withdrawn from individuals who visited a university hospital and this might be one background for their clinical characteristics. Therefore, we cannot fully rule out potential bias caused by this factor of the participating hospital. In the period when our participants underwent carotid ultrasound, physicians might have commonly referred to the guidelines at that time.21) Carotid ultrasound was recommended to intermediate risk group with class IIa. However, there was no mention on the test in low risk population. In this regard, routine carotid study in the low risk group seems to be carried out beyond the guidelines. Finally, as we collected event data from electronic hospital record review, there might be a substantial number of undetected event cases with this retrospective study design.
In conclusion, this study analyzed the statin effects in individuals with low to moderate cardiovascular risk but with carotid plaque, for whom statins were off-label. Statins demonstrated no significant cardiovascular benefit in this population. The current findings provide an evidence that could assist physicians in clinical decision-making regarding lipid-lowering pharmacotherapy in these individuals.
 XML Download
XML Download