

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In patients with ischemic stroke, various neurological deficits could occur resulting in mild to severe symptoms based on the location and size of the occluded blood vessels. Severe neurological deficits can occur in patients with large vessel occlusion, such as internal carotid artery, middle cerebral artery of the anterior circulation, and basilar artery of the posterior circulation. Since brain injury starts immediately following the occlusion of the blood vessel in a patient with ischemic stroke with large vessel occlusion, treatment to recanalize the occluded cerebral artery is necessary as soon as possible. Current medical guidelines recommend intravenous thrombolytic agent administration and intra-arterial thrombectomy as treatments for acute ischemic stroke.1 Intravenous thrombolytic agents were approved in 1995 and can be used within 4.5 hours of symptom onset.2 Intra-arterial thrombectomy, as mechanical thrombectomy (MT) that involves eliminating the thrombus from a large occluded cerebral artery and recanalizing it, was first included in the guidelines in 2015 based on four clinical studies that achieved better outcomes than standard medical treatment.3 Performing the procedure on patients who visited the hospital within 6 hours following the neurological deficit was possible when MT was first recommended as a treatment guideline. Patients who visited the hospital within 6 hours following confirmation of the neurologic deficit were included in the previous study; however, the patients who had passed 6 hours from the last normal time since the exact time point of the neurologic deficit were not known were not eligible for treatment. Moreover, in patients with developed collateral circulation of cerebral blood flow, even after 6 hours or more following cerebral artery occlusion, the ischemic core was not large; thus, thrombectomy was expected to be effective.4 Thereafter, two studies comparing MT with standard medical treatment (SMT) was conducted in patients who had not yet suffered severe ischemic brain injury 6 hours following the onset of symptoms.56 The two studies included a study on thrombectomy in stroke within 6 to 24 hours of onset showing discrepancy between the neurologic deficit and ischemic lesion, and a study on the effect of thrombectomy in stroke within 6 to 16 hours of onset selected through advanced perfusion imaging. In both studies, the rate of good prognosis (modified rankin scale [mRS] ≤ 2) was analyzed in patients with cerebral artery occlusion in the anterior circulation for more than 6 hours following the occurrence of neurologic deficit. The prognosis was favorable in 45–49% and 13–17% in patients undergoing MT and SMT, respectively. Based on these study results, in 2018, the US first published guidelines for MT treatment that expanded the target population of MT treatment to patients within 24 hours of symptom onset.7 In South Korea, the medical guidelines were also revised in 2019; selection of the treatment target population using appropriate multi-modal imaging profiles for patients within 24 hours of symptom onset was recommended.1
Various methods are considered for selecting the treatment target population according to the medical institution. These methods are largely divided into two categories: a clinical-core mismatch between clinical symptoms and the ischemic core, or a perfusion-core mismatch between a penumbral region and the ischemic core. These two methods require identification of the ischemic core that has already suffered irreversible damage. This can be accurately confirmed by diffusion-weighted images in brain magnetic resonance imaging (MRI); however, performing an emergency MRI examination is challenging in many healthcare institutions. Thus, each hospital is known to prepare a protocol based on the hospital settings and conduct an examination for target patient selection.8 While performing brain computed tomography (CT) angiography (brain CTA), which is required to confirm the occlusion of the cerebral artery, cerebral perfusion and ischemic core could be assessed and estimated. However, the exact volume of the ischemic core cannot be confirmed with the existing test method alone, and the patient to be treated was selected based on the judgment of experienced physicians. In clinical studies, the volume of the ischemic core was calculated by automatically analyzing the results of perfusion CT with advanced imaging software to overcome these limitations and accurately select the patients to be treated.56 Since such software can only be used by paying the developer’s license fee on an annual subscription basis, it is currently used in very limited healthcare institutions in South Korea.
This study aimed to use software that automatically processes perfusion CT results for patients with acute ischemic stroke to determine the expansion of the MT target population and analyze the prognosis. It also aimed to compare and analyze the prognosis of patients who received SMT without MT before software introduction and those who received MT after software introduction.
METHODS
Study population
Patients admitted for ischemic stroke at the emergency room (ER) at the Department of Neurology, National Health Insurance Service (NHIS) Ilsan Hospital, were selected as the participants for this study. Our hospital has a protocol for performing brain CTA and perfusion CT to identify patients who are indicated for MT. Until December 2018, the protocol was applied to patients who visited the ER within 12 hours following the onset of neurologic deficit. RAPID (iSchemaView, Menlo Park, CA, USA), a software that automatically analyzes perfusion CT, was first used in May 2018 at our hospital. After the introduction of RAPID software, the time indication was extended to 24 hours from January 2019. The patients were selected for the same period of 2 years before and after the introduction of the software, from 2016 to 2020, except for patients hospitalized in 2018.
First, the patients with acute ischemic stroke, who visited the hospital within the time indicated for reperfusion therapy with the test results for assessment of the occluded cerebral artery were identified. Thus, among the patients who visited the ER and were admitted to the neurology department after being diagnosed with ischemic stroke, those who had brain CTA and perfusion CT were selected. Among these patients, those with occluded cerebral artery associated with neurologic deficit requiring reperfusion therapy were considered.
Thereafter, among the patients between 2016 and 2017, those who did not receive reperfusion therapy for a valid reason were selected as the control (SMT group). For selecting the patients, the time taken from the last normal time (LNT) to visiting the ER was investigated. Among the patients from 2016 to 2017, since CTA and perfusion CT were performed within 12 hours of the neurologic deficit, more than 12 hours passed since the LNT was also included. Those who were not eligible for reperfusion therapy according to the guidelines, among those who visited the hospital within 24 hours of LNT and did not receive reperfusion therapy since the occlusion of the cerebral artery was identified, were excluded from the control as follows9: those with mild neurologic deficit (National Institutes of Health Stroke Scale [NIHSS] ≤ 6), those with rapid neurological improvement following admission or intravenous thrombolytic (tissue plasminogen activator, tPA) administration, Alberta Stroke Program Early CT Score (ASPECTS) < 6, and those with an mRS score > 2 before onset.
Before the introduction of RAPID software in May 2018, the decision of performing MT was at the discretion of the neurologist and interventional radiologist at our hospital based on the neurologic deficit and radiological findings. After the introduction of the software, patients with an ischemic core of less than 70 ml and an ischemic penumbra-to-core ratio of 1.8 or more were subjected to MT as indicated in previous clinical studies.56 In our hospital, with the exception of the change in the time indication for MT, the protocol for treatment in the intensive care unit and stroke unit following MT remained the same during the study period. Among the patients from 2019 to 2020, the patients who received MT after visiting the hospital for more than 6 hours from symptom onset, were selected as the cases (extended MT [EMT] group). In order to identify the change in the ratio of thrombectomy-treated patients to total patients with ischemic stroke before and after the introduction of RAPID, patients who underwent MT during the entire study period were also selected and checked. Among them, patients who visited the hospital within 6 hours and underwent MT according to the existing guidelines over the same period as the EMT group, were classified into the MT within 6 hours (MTW6) group.
From the perfusion CT, the EMT and MTW6 groups were able to obtain the ischemic core and penumbra volumes and the mismatch from the RAPID software. Since these volumes could not be obtained in the SMT group, the authors measured the ASPECTS, which indicates initial ischemic injury, using non-contrast brain CT. The medical records were reviewed for hypertension, diabetes, atrial fibrillation, chronic kidney disease, history of ischemic stroke, cancer, and smoking status for determining the risk factors for ischemic stroke in the patients.
Outcome
The degree of neurologic deficit (NIHSS) at the time of discharge of the patients and mRS after 3 months were evaluated. Based on analyzing the association between quality of life and mRS in previous studies,10 mRS of 3 is known to be closer to 2 than 4, and the prognosis is classified as poor for mRS of 4 or higher. Those with an mRS of 2 or lower and capable of living independently were classified as having a good prognosis. The thrombolysis in cerebral infarction (TICI) grade was checked for patients who underwent MT to determine the success of the treatment. TICI grades 2b and 3 were defined as successful recanalization.
Statistical analysis
When all the study participants were classified into each group, whether the normal distribution was satisfied was assessed since there were fewer than 30 groups. When the normal distribution was not satisfied, the Mann-Whitney test, a non-parametric statistical analysis method, was used. Continuous variables are expressed as mean ± standard deviation if normally distributed or median (interquartile intervals) if not normally distributed. A χ2 test was performed to compare the frequency of comorbidities among the study participants. Multiple logistic regression analysis was performed to confirm prognosis-related factors. We aimed to determine whether the prognosis of the EMT group was better than that of the SMT group. In addition, we analyzed whether the prognosis of the EMT group was different from that of the MTW6 group treated for the same period. A statistical significance of less than 0.05 as a result of a two-tailed test was defined as significant.
RESULTS
From 2016 to 2017, 1,058 patients were hospitalized for ischemic stroke; among them, 458 patients (43.3%) had brain CTA and perfusion CT scans. Among them, 63 patients visited the hospital within 24 hours of LNT; however, they did not undergo MT. Of these, 36 had valid reasons for not receiving MT: 23 patients had an NIHSS score of 6 or lower, 6 patients had an mRS score of 3 or higher before the onset of ischemic stroke, 4 patients had thrombus migration, 2 patients had ASPECTS of 5, and 1 patient had improved neurologic deficit after using tPA. From 2019 to 2020, 1019 patients were hospitalized for ischemic stroke, and among them, 508 patients (49.9%) had brain CTA and perfusion CT scans. Among them, 85 patients (8.3%) received MT (Fig. 1). From 2016 to 2017, among the 63 patients who visited the hospital within 24 hours of the last normal time but did not receive MT, 27 patients met the indications for MT according to the current guidelines; however, they were treated only by SMT (SMT group). From 2016 to 2017, among the patients with ischemic stroke, 60 patients (5.7%) received MT. From 2019 to 2020, among the 85 patients with ischemic stroke who received MT (8.3%), 24 patients visited the hospital between 6 and 24 hours of LNT (EMT group), and 61 patients visited the hospital within 6 hours of LNT meeting the previous guidelines (MTW6 group).
Fig. 1
The process of selecting subjects for the study among all patients with ischemic stroke.
CT = computerized tomography, NIHSS = National Institutes of Health Stroke Scale, Pre-mRS = pre-modified rankin scale, ASPECTS = Alberta Stroke Program Early CT Score, tPA = tissue plasminogen activator.
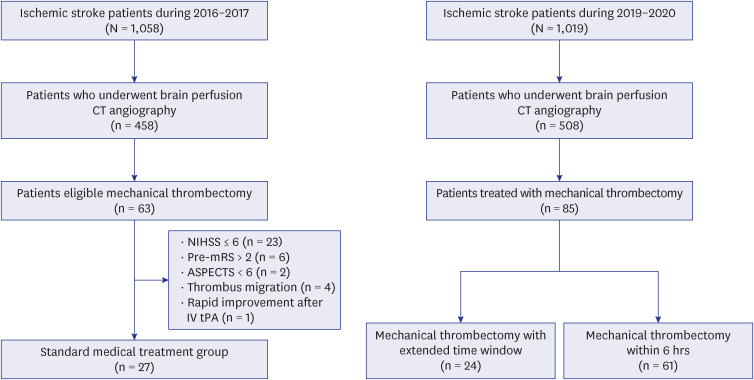
Table 1 shows the clinical characteristics and prognosis of the SMT and EMT groups. There was no statistically significant difference in the age of the two groups. Considering the comorbidities, diabetes and smoking were more common in the group that received MT (EMT group). Among the patients in the SMT group, 18 patients came to the hospital within 6 hours, and 9 of them received intravenous thrombolytics (tPA). However, among them, only 3 patients (11.1%) had a good prognosis at 3 months; 24 patients (88.9%) with a poor prognosis and 9 deaths (33.3%) were reported. On the other hand, in the EMT group, patients who could receive intravenous thrombolytics were not present; however, recanalization of the occluded cerebral artery was successfully performed in 19 patients (79.2%). Among them, 10 patients (41.7%) had a good prognosis at 3 months, with only 9 patients (32.5%) having a poor prognosis and no deaths were reported.
Table 1
Clinical characteristics of SMT and EMT groups
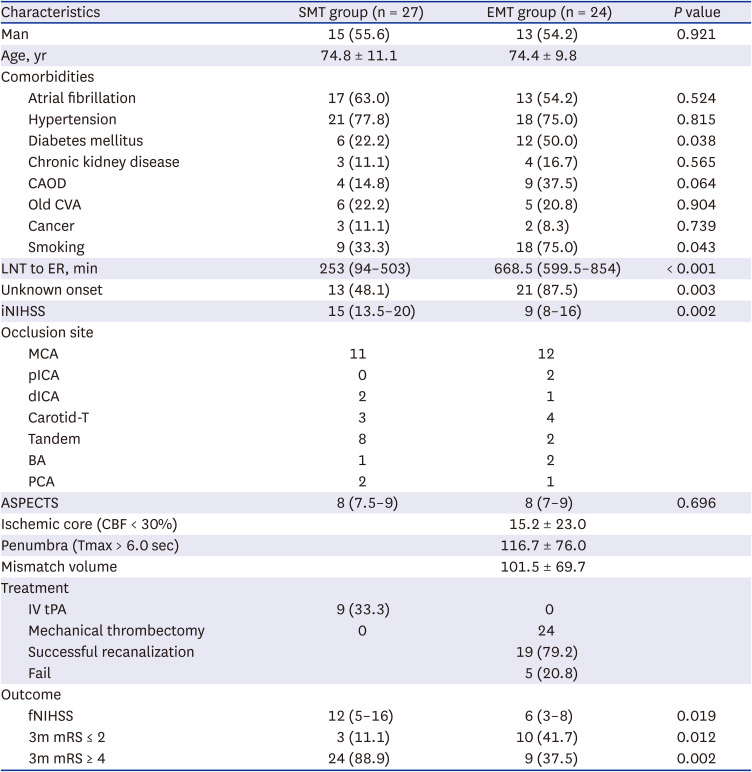
Variables are expressed as mean ± standard deviation, number (%), or median (interquartile intervals).
SMT = standard medical treatment, EMT = extended mechanical thrombectomy, CAOD = coronary artery obstructive disease, CVA = cerebrovascular accident, LNT = last normal time, ER = emergency room, iNIHSS = initial National Institutes of Health Stroke Scale, MCA = middle cerebral artery, pICA = proximal internal carotid artery, dICA = distal internal carotid artery, Tandem = occlusion of proximal internal carotid artery and middle cerebral artery, BA = basilar artery, PCA = posterior cerebral artery, ASPECTS = Alberta Stroke Program Early CT Score, CBF = cerebral blood flow, tPA = tissue plasminogen activator, fNIHSS = final National Institutes of Health Stroke Scale, mRS = modified rankin scale.
Table 2 shows the results based on the comparison of the characteristics and prognosis of the EMT and MTW6 groups. Based on the comparison of the comorbidities and clinical features of patients between EMT and MTW6 groups, a statistical difference was observed only in the presence or absence of smoking. There was no difference in the volume of the ischemic core in the perfusion images; however, the volume of the penumbra was statistically smaller in the EMT group (P = 0.036). There was no difference in the recanalization success rate and good prognosis between the two groups (P = 0.628). In the MTW6 group, most (90.2%) of the occluded cerebral artery were recanalized successfully. At 3 months, 33 patients (54.1%) with a good prognosis, 28 patients (45.9%) with a poor prognosis, and 6 deaths (9.8%) were reported.
Table 2
Clinical characteristics of patients who received MT according to time
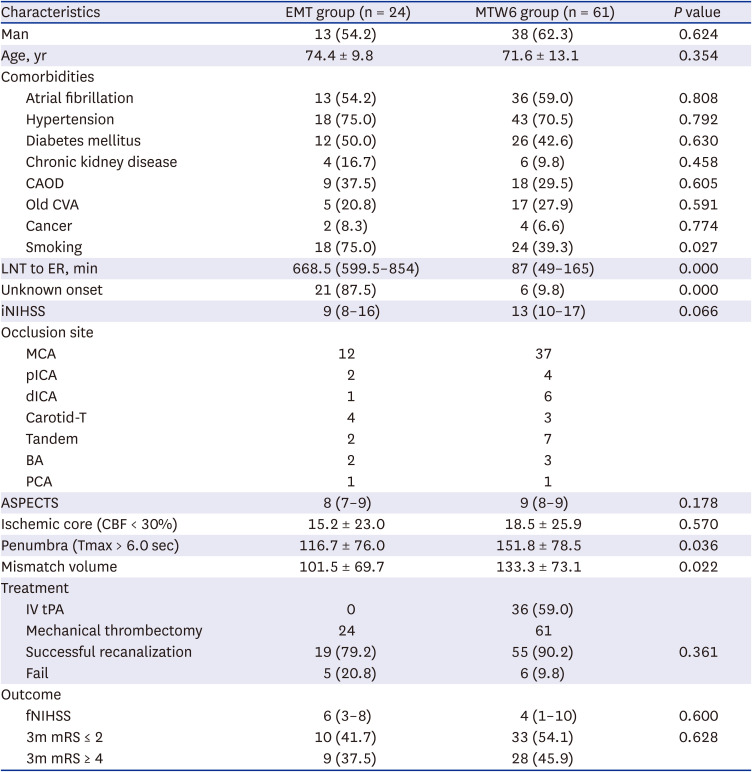
Variables are expressed as mean ± standard deviation, number (%), or median (interquartile intervals).
MT = mechanical thrombectomy, EMT = extended mechanical thrombectomy, MTW6 = mechanical thrombectomy within 6 hours, CAOD = coronary artery obstructive disease, CVA = cerebrovascular accident, LNT = last normal time, ER = emergency room, iNIHSS = initial National Institutes of Health Stroke Scale, MCA = middle cerebral artery, pICA = proximal internal carotid artery, dICA = distal internal carotid artery, Tandem = occlusion of proximal internal carotid artery and middle cerebral artery, BA = basilar artery, PCA = posterior cerebral artery, ASPECTS = Alberta Stroke Program Early CT Score, CBF = cerebral blood flow, tPA = tissue plasminogen activator, fNIHSS = final National Institutes of Health Stroke Scale, mRS = modified rankin scale.
Upon comparing the SMT and EMT group, including the accompanying risk factors, the factor that had the greatest effect on poor prognosis was the MT performance (adjusted odds ratio [OR], 49.104; 95% confidence interval [CI], 2.760–173.549; P = 0.008). Furthermore, the degree of neurologic deficit (iNIHSS) (adjusted OR, 1.412; 95% CI, 1.008–1.832; P = 0.009) at the ER visit was a predictor of poor prognosis, and the comorbidities were not related to the prognosis (Table 3).

DISCUSSION
In line with previous reports, this study confirmed that the patients who received MT treatment by applying the extended time indication had a better prognosis than those who received only SMT. The EMT group in this study showed a similar prognosis to the MTW6 group. In this study, among patients who received SMT prior to the introduction of the software, those with an mRS ≤ 2 accounted for 11.1%, which was slightly lower than the previous study result of 13%.6 The rate of mRS ≤ 2 with a good prognosis among the EMT group was 41.7%, slightly lower than that of existing clinical studies,6 which was presumably attributed to a difference between the actual clinical data and the study results obtained from selected patients. The rates of good prognosis were reportedly 34% and 53.7% in other studies analyzing the patients treated by applying the extended time indication in the actual clinical settings and in our study, respectively.1112 While the rate of successful recanalization (79.2%) was slightly lower in the EMT group meeting the extended time indication than in the MTW6 group, it was still similar to the previously reported recanalization success rate of MT (76%).13
At our hospital, the total number of hospitalized patients with ischemic stroke decreased by 3.7% following the introduction of advanced imaging software: however, the rate of screening for patients eligible for MT increased by 6.6%. The number of cases undergoing MT increased by 41.7% following the introduction of the software, which was higher than the rate reported in other similar studies.14 Among patients with ischemic stroke, the proportion of patients receiving MT increased by 2.6%. If all of the patients in the SMT group had received MT, the proportion of MT before the introduction of the software would have been 8.2%, nearly the same as the proportion following the introduction. The proportion of patients receiving MT among all the patients with ischemic stroke following the introduction of the software was much higher than the proportion known from the South Korean ischemic stroke database in 2014 (3.6%).15 In the United States, 3.1% of patients with ischemic stroke received MT from 2015 to 2016.16 From 2016 to 2018, the proportion of patients receiving MT among more than 200,000 patients treated at 173 hospitals increased to 8.4%, which was consistent with the findings of our study.17 A German registry study also found that the proportion of patients with ischemic stroke who underwent MT increased from 4.3% in 2016 to 7.2% in 2019.18 A study estimated the proportion of patients eligible for MT in a time window of less than 6 hours in patients with ischemic stroke as 9%.19 However, the ratio reportedly could be up to 12.2% when the time window extended to 24 hours.20 Therefore, fewer patients are more likely to be treated with MT than those who are actually eligible to receive MT.
Approximately 100,000 patients are known to suffer from strokes annually in South Korea, and nearly 80% of them include patients with ischemic stroke. Approximately 80,000 patients are estimated to suffer from ischemic stroke annually.15 Upon checking the number of cases undergoing MT based on the claim code, MT has been performed over 5,000 times each year since 2019,21 for nearly 6.3% of all patients with ischemic stroke. Therefore, a significant number of patients with ischemic stroke who are eligible for MT are presumably not receiving effective treatment. Several obstacles, such as MT, exist that prevent patients with ischemic stroke from receiving effective treatment.22 One of them is the detection of a large vessel occlusion to be smaller; thus, the use of vascular imaging in all patients with suspected ischemic stroke could be a potential solution. However, the use of advanced brain imaging software, such as RAPID used in this study, incurs a fee by healthcare institutions, and currently, these costs cannot be billed to the patients, hindering its use at healthcare institutions. In the United States, a new technology add-on payment system for such software has created a new billing code to reduce the cost burden.23 Solving the cost problem of advanced imaging software would allow more healthcare institutions to utilize the software, thereby increasing the number of patients who can receive MT.
This study has several limitations. First, the results are based on the data of patients collected retrospectively from a single healthcare institution. Since advanced brain imaging software was recently introduced in South Korea, combining and analyzing the data from multiple healthcare institutions are considered challenging. Second, the number of patients who have undergone MT is small. Since the healthcare institution that collected the information of the study participants did not refer patients from other hospitals, the total number of patients with ischemic stroke was not large, which resulted in a small sample size, making the use of various statistical analysis methods impossible. Lastly, since the time criteria for the imaging protocol in the two periods were different, some patients who presented symptom onset within 24 hours but failed to undergo perfusion CT were not included in the study population during 2016–2017.
Based on the results of this study, it was confirmed that the treatment results of patients who underwent MT were favorable by applying the extended indication following the introduction of the advanced brain imaging software. Owing to the increase in the aging population, the number of patients with ischemic stroke will continue to increase in the future, with more patients eligible for MT. There are still ten organizations in South Korea that are able to use advanced imaging software since 2021.24 The introduction of such software in more institutions could result in a greater number of MT eligible ischemic stroke patients, which could lead to a better prognosis following treatment.
 XML Download
XML Download