

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The current pandemic of coronavirus disease 2019 (COVID-19) has set up new challenges in the management of persons with chronic diseases such as rheumatological disorders.12 Various registries and surveys have helped provide real-world data on patients with rheumatic diseases. Analysis of data from electronic record databases and other registries has shown that COVID-19 outcomes are usually poorer in patients with rheumatic diseases.34567 However, the bulk of this data is limited to patients having common rheumatic diseases like rheumatoid arthritis, spondyloarthritis (SpA), systemic lupus erythematosus, or psoriatic arthritis. There is some evidence that patients with SpA may have better outcomes with COVID-19.8 However, limited information is available about reactive arthritis (ReA) during the pandemic.
The classical definition of ReA encompasses arthritis that occurs around 2–4 weeks after a genitourinary or enteric infection and with no direct infection in the primary joint structures.91011 It is a sub-type of SpA. Arthritis occurs as a result of immune-mediated changes rather than the direct invasion of the joints by any pathogen.12 Several pathognomonic features are sacroiliitis, uveitis, dactylitis or enthesitis. The presence of the HLA-B27 gene or a family history of SpA, psoriasis, or uveitis helps to categorize a patient as having ReA.13 In countries where ReA is not commonly diagnosed, it may be misclassified as peripheral oligoarthritis or even psoriatic arthritis.14
ReA is prevalent in lower-income countries. In contrast, it is not so much known in Eastern Europe and Central Asia. Worldwide it is thought that the incidence of ReA is declining. However, it is still encountered in developing countries where infections are common. Several questions remain unanswered about the patterns of ReA worldwide, in the background of wider antibiotic use and immunosuppressants. HIV-related infections are on the rise globally and these also seem to play a role in the pathogenesis of ReA as a direct arthritogenic agent or causing immune dysfunction and deregulation in the production of cytokines predisposing to infection by other arthritogenic pathogens.1516
Generally, COVID-19 presents with mild to modest musculoskeletal symptoms such as arthralgia and myalgia. It does not typically cause clinical arthritis. The pattern of profound inflammation and generation of pro-inflammatory cytokines is similar between COVID-19 and ReA.17 The introduction of the term “post-COVID ReA” has led to many new questions.10 Also, ReA after COVID-19 vaccination has been reported.18 After the COVID-19 pandemic, the emergence of this “post-COVID-19 ReA” has raised an important question of whether we must persist with the traditional definitions of ReA or update it to include more diverse entities. There is a burning need to allow or disallow arthritides occurring after emerging infections to be called ReA. The controversies brought forth in ReA by the pandemic are best summarized elsewhere.19
The focus is particularly on therapeutic cytokine inhibition to counteract the pathological hyper-inflammatory disease state. However, none of the rheumatology societies or such international organizations has advised on the management of ReA during the current pandemic. Therefore, this survey was conducted to look at the patterns of ReA encountered by rheumatology practitioners and understand their choices, especially in the context of the COVID-19 pandemic.
Go to : 
METHODS
This survey was devised to cover the current knowledge and perceptions of healthcare workers (HCWs) regarding ReA diagnosis and management amidst the COVID-19 pandemic. An online platform (SurveyMonkey.com) was used to carry out the survey.
Survey design
The survey was designed to obtain information about the understanding of pathogenesis and specific features of ReA (arthritis, dactylitis, enthesitis, conjunctivitis, uveitis, oral and/or genital ulcers, sacroiliitis), clinical presentation, common test practices used for diagnosis, presence of preceding infection (urogenital, gastrointestinal and respiratory), the time interval between triggering infection and onset of arthritis and commonly used management strategies in ReA patients. The survey also obtained information regarding arthralgia and/or arthritis cases post COVID-19 infection and changes in ReA incidence over time as experienced by HCWs in their practice.
Three experts reviewed the questions over three rounds of discussion to finalize the wording and ensure content validity. The third round included dummy fill-ups of the online form to have a real feel. After finalization, the survey included 20 questions, of which 18 were multiple choice questions with a single answer to be chosen for 13 and multiple answers allowed for five questions. The two remaining questions needed numerical value entry only.
The respondents could change the answers before submission but not after it. All questions were made mandatory, such that partial responses were automatically discarded by the SurveyMonkey platform.
Sampling strategy
We employed a convenient sampling strategy. The questionnaire was circulated on social media platforms like Twitter and Facebook between 6th October 2021 and 23rd January 2022. The survey began with an informed consent document with all information pertaining to the survey mentioned therewith.
The survey link was open from the time the survey link was circulated on social media. The cover letter included details on the background and purpose of the study. Informed consent was taken at the beginning of the survey and no incentives were offered for survey completion.
Statistical analysis
The normality of data was checked by the Shapiro-Wilk test. Mostly descriptive statistics are presented. For graphical representations, Microsoft Excel (Microsoft, Redmond, WA, USA) was used to build figures. Chi-square tests were used to compare responses between groups. Results were considered to be significant at a P value of < 0.05. Statistical analysis was performed also using Microsoft Excel.
Confidentiality
The survey was partly anonymised with Internet Protocol (IP) addresses and emails of respondents being the only linked identifiers. These identifiers were used to ensure unique entries from each individual. Data handling was completely anonymous, with the IP addresses and email lists remaining with the first and corresponding author. Other authors had access to the synthesized data in tables without linked identifiers.
Ethics statement
Full ethics review was exempted by the Institutional Ethics Committee of Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow (protocol number 2021-299-IMP-EXP-44). We adhered to our recommendations on online surveys during the COVID-19 pandemic20 and the Checklist for Reporting Results of Internet E-surveys to report the data.21
Go to :
RESULTS
Out of a total of 193 respondents, nearly half (88, 45.6%) were adult rheumatologists followed by general practitioners (24, 12.4%). Nearly one-third lived in Kazakhstan (59, 30.6%) followed by Turkey (41, 21.2%). There were responses from 22 other countries also. A detailed description of the demographics of the respondents is presented in Table 1.
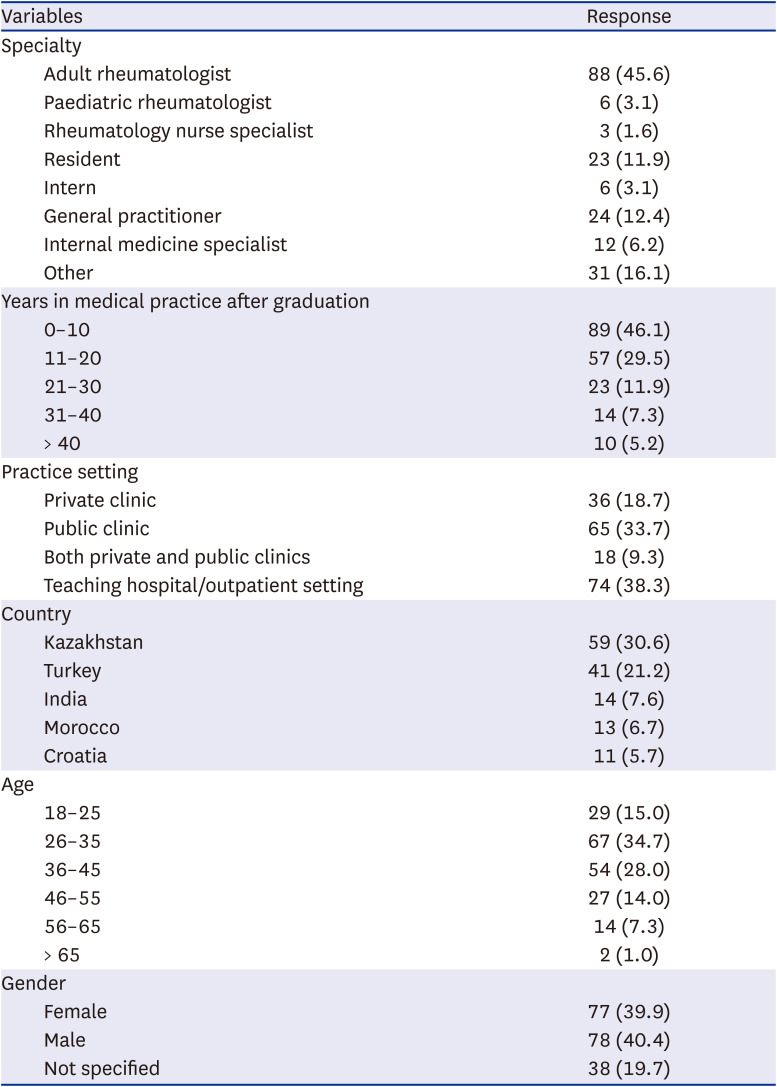
Table 1
Baseline demographics
![]()
Presenting features of ReA
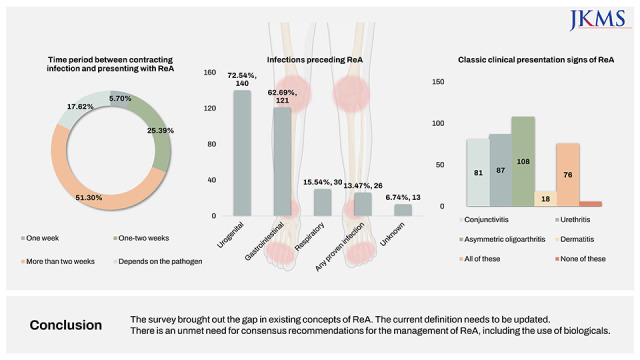
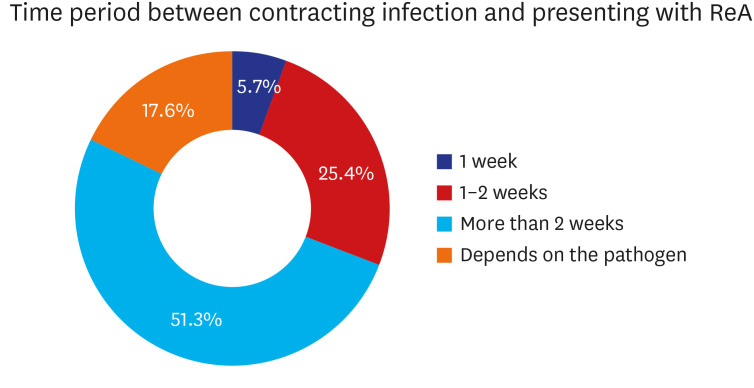
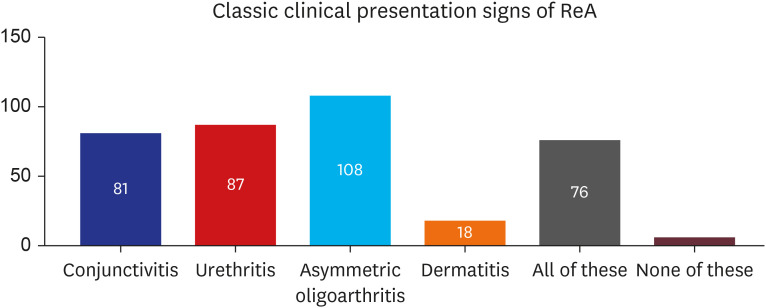
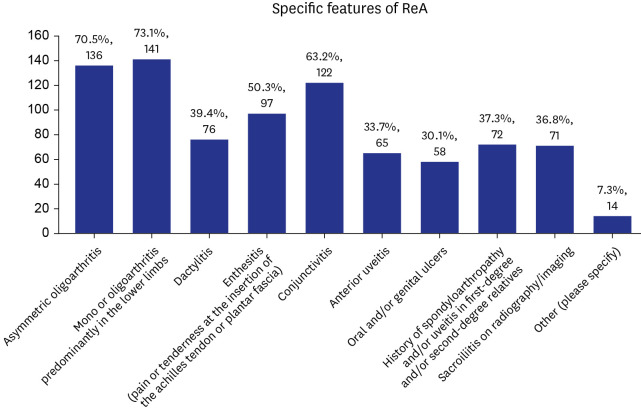
More than half (123, 63.7%) of the respondents were aware of the definition of ReA along with its origin, with nearly one-third (42, 21.8%) knowing the definition. Based on observations in clinical practice, the period between contracting the infection and presenting with ReA was reported to be more than two weeks in nearly half the cases (99, 51.3%) (Fig. 1). Urogenital (140, 72.5%) and gastrointestinal (121, 62.7%) system infections were among the majority to precede ReA (Fig. 2). Nearly half of the respondents reported that the triad of conjunctivitis (81, 42.0%), urethritis (87, 45.1%), and asymmetric oligoarthritis (108, 56.0%) were the classic clinical presentation signs of ReA. More than one-third (76, 39.4%) reported dermatitis in addition to the classical triad (Fig. 3). Among the specific features of ReA, nearly three-fourths (141, 73.1%) reported mono or oligoarthritis predominantly in the lower limbs, followed by asymmetric oligoarthritis (136, 70.5%), conjunctivitis (122, 63.2%) and enthesitis (pain or tenderness at the insertion of the Achilles tendon or plantar fascia) (97, 50.3%) (Fig. 4).
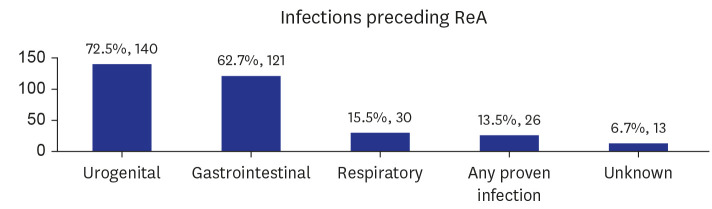 | Fig. 2Infections preceding ReA. Y axis depicts the number of respondents.ReA = reactive arthritis.
|
Diagnosis of ReA
Among the tests employed to examine ReA patients in order to reach a diagnosis, C-reactive protein (132, 68.4%) was the most commonly used modality followed by a test for Chlamydia trachomatis (120, 62.2%), Joints imaging/ultrasonography (affected joints and sacroiliac joints) (118, 61.1%), HLA-B27 (116, 60.1%) and others. However, nearly three-fourths (138, 71.5%) reported that there are no specific tests for the diagnosis of ReA.
Treatment of ReA
Non-steroidal anti-inflammatory drugs were the most commonly (162, 83.9%) used drug for the management of ReA in practice settings, followed by Intraarticular corticosteroid injections (79, 40.9%), Methotrexate and other disease-modifying antirheumatic drugs (78, 40.4%) and others.
Table 2 gives a detailed description of the Knowledge and perceptions of ReA diagnosis and management amidst the COVID-19 pandemic. Table 3 gives a detailed description of the Knowledge and perceptions of ReA diagnosis and management in Kazakhstan and Turkey.
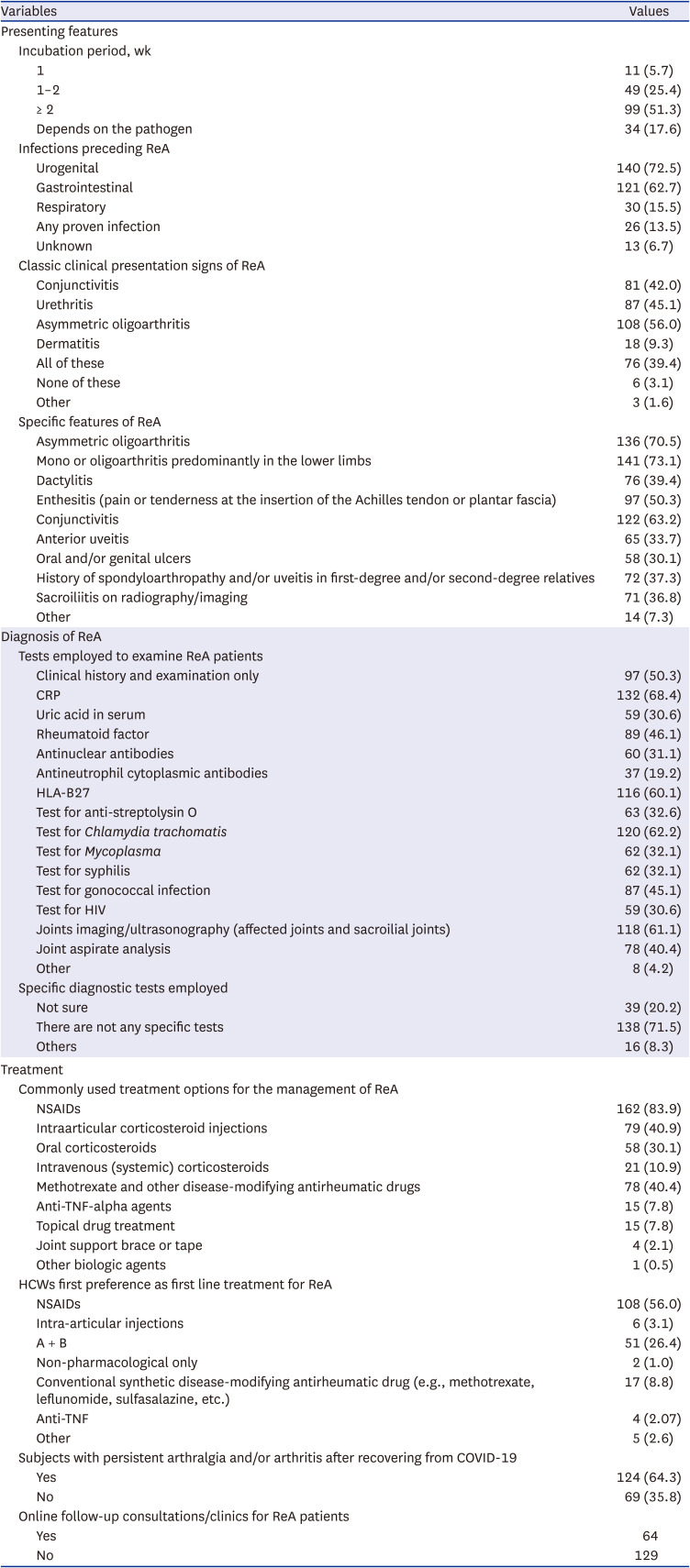
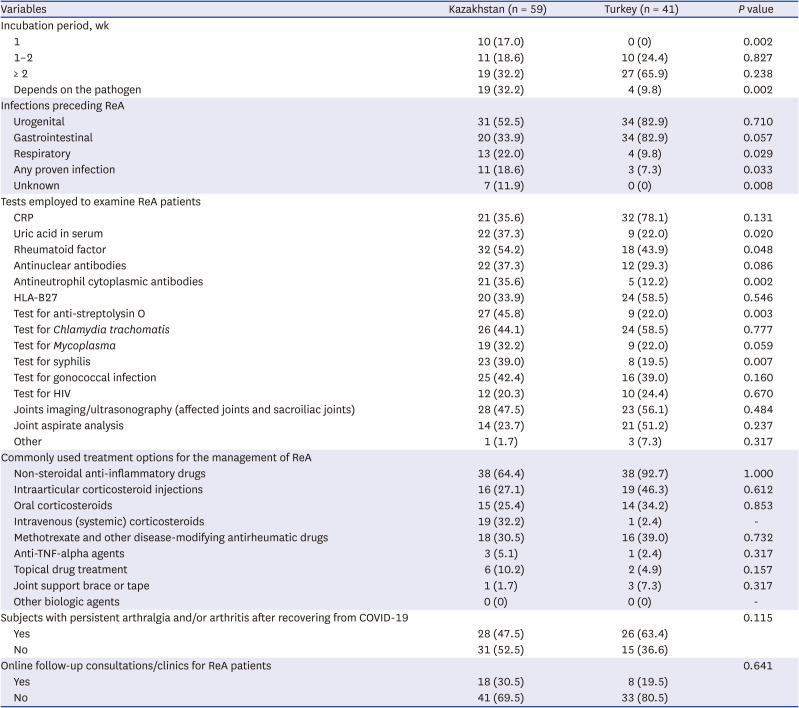
Table 2
Knowledge and perceptions of ReA diagnosis and management amidst the COVID-19 pandemic
Values are presented as number (%).
ReA = reactive arthritis, COVID-19 = coronavirus disease 2019, HIV = human immunodeficiency virus, CRP = C-reactive protein, NSAID = non-steroidal anti-inflammatory drug, TNF = tumor necrosis factor, HCW = healthcare worker.
![]()
Table 3
Knowledge and perceptions of ReA diagnosis and management in Kazakhstan and Turkey
Values are presented as number (%).
ReA = reactive arthritis, COVID-19 = coronavirus disease 2019, HIV = human immunodeficiency virus, CRP = C-reactive protein, TNF = tumor necrosis factor.
![]()
Go to :
DISCUSSION
This study aimed to identify the current knowledge and perceptions of HCWs regarding ReA diagnosis and management amidst the COVID-19 pandemic. The epidemiology of ReA has been evolving15and the COVID-19 pandemic has made it evolve further.
Nearly half of the survey respondents (88, 45.6%) were adult rheumatologists with up to 10 years of experience in medical practice after graduation (89, 46.1%). Nearly one-third of the respondents practised at a public clinic (65, 33.7%) and a teaching hospital/ outpatient setting respectively (74, 38.3%). The majority of the responses were from Kazakhstan (59, 30.6%) and Turkey (41, 21.2%).
ReA is inflammatory arthritis which manifests after several days to weeks after a genitourinary or gastrointestinal infection.22 When the findings from Kazakhstan and Turkey are compared, we note that there is a significant difference in the percentage of respiratory infections preceding ReA, with the number of cases encountered being higher in Kazakhstan. It may point to the changing pattern in pathogens preceding ReA which could be a consequence of COVID-19 infection and its effects on individuals. Respondents from different parts of the world may be using different concepts or definitions of ReA.23
This perception of ReA occurring after respiratory infections is possibly the effect of the COVID-19 pandemic. ReA is often an orphan disease that may be neglected by physicians. However, the COVID-19 pandemic has brought it to the forefront.24 Before this interest is lost, it is imperative to update the definitions of ReA so that physicians worldwide recognise this entity in the same conceptual framework. Several newer pathogens beyond severe acute respiratory syndrome coronavirus 2 are being implicated in the pathogenesis of ReA.25 Nevertheless, there is no consensus on how to include newer pathogens in the definition of ReA.13
Among the tests employed to examine ReA patients, there was a significant difference between Kazakhstan and Turkey when it came to the following tests: serum urate levels, rheumatoid factor, anti-neutrophil cytoplasmic antibodies, test for anti-streptolysin O and test for syphilis, all of which is used in higher numbers in Kazakhstan. This may suggest the change in aetiology and origin of ReA over the years. However, regardless of the infectious agent and diagnostic modality, there has been no difference observed in the treatment of ReA.26 The management goals of ReA in terms of providing symptomatic relief and preventing chronic complications are still prevalent.
This study also highlights the lack of clarity and consensus regarding the diagnosis and care of ReA. This is not new and has been acknowledged even whenever attempts have been made to structure working definitions.1927 Expanding the definition of ReA requires input from all parts of the world and this survey contains perspectives from central Asia that are often missing in the literature.28 Since it is a relatively uncommon disease, it requires well-defined hypotheses and planning to establish clinically relevant case definitions.29
The limitations of the study include the snapshot picture of the data captured during the pandemic period. The pattern and chronicity may change in the future. It is also limited by the fact that the relationship between COVID-19 and ReA was not studied in great detail.
This survey highlights the varied interpretations of ReA by different respondents and the lack of consensus in management, especially during the COVID-19 pandemic. This calls for a united international effort for experts in the field to get together and formulate and update current definitions of ReA.
Go to :
 XML Download
XML Download