

 PDF
PDF Citation
Citation Print
Print



FIRST CORONAVIRUS DISEASE 2019 (COVID-19) OUTBREAK IN DAEGU CITY, KOREA, AND THEIR INITIAL RESPONSE
The first case of COVID-19, which is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), in Korea was reported on January 20, 2020. The first epidemic occurred in Daegu city (a city in South Korea located in the southeastern Korean Peninsula, with about 2,400,000 population),1234 which stemmed from a massive outbreak in the religious group Shincheonji.1345 In addition, several confirmed cases were reported in medical institutions and religious facilities.12
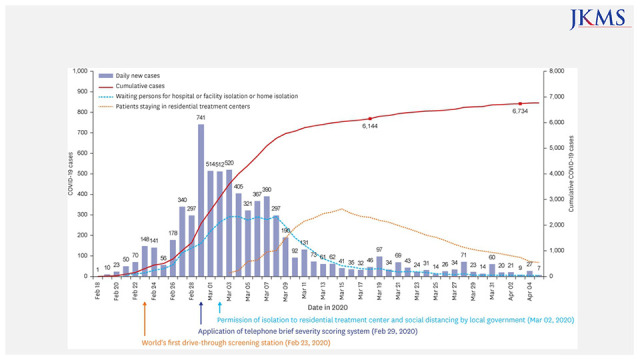
Fig. 1 shows the explosive diagnosis of initial patients and the responses of Daegu city and national government.1236
Fig. 1
The first reported case of COVID-19 in Daegu (the first epidemic in Korea).
COVID-19 = coronavirus disease 2019.
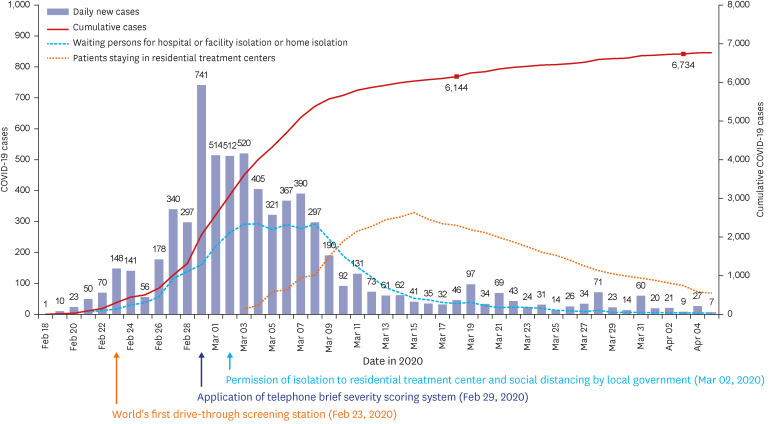
Table 1 summarizes the responses in Daegu city during the early epidemic period. The responses included prompt isolation and quarantine action by local government with cooperative help from expert groups and the central government and rapid expansion of negative-pressure beds in the hospitals. Citizens refrained from leaving home, and high-intensity social distancing was implemented by local government (Fig. 1).78 Along with the rapid increase in the number of patients, there was a shortage of negative pressure rooms; hence, ‘residential treatment centers’, at the time not permitted under the law, were opened. This initiative was approved by the Korea Disease Control and Prevention Agency (KDCA) upon the request of Daegu city during the early period of the COVID-19 outbreak. The isolation of COVID-19 patients in residential treatment centers was performed for the first time in Korean history, which helped resolve the shortage of hospital beds in the area (Fig. 1).910 In cases where face-to-face care was difficult to perform, a telephone scoring system for predicting the disease severity was effectively used to allocate COVID-19 patients to negative pressure intensive care unit (ICU), negative pressure general ward or residential treatment center.10
Table 1
Strategies for the responses during the initial COVID-19 outbreak in Daegu
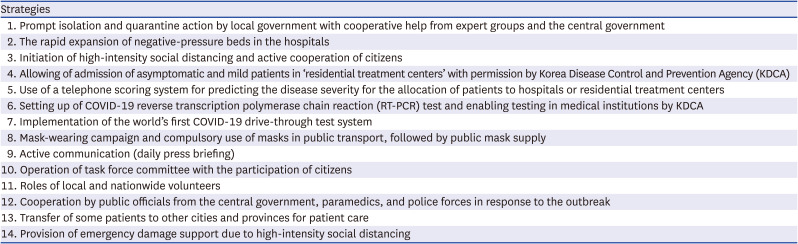
Several medical personnel and volunteers, paramedics, and the police force helped the response.11 Due to the lack of negative pressure rooms, some patients received medical care in beds in other cities outside Daegu city. The KDCA played a major role in Korea’s early response to COVID-19 by setting up of COVID-19 reverse transcription polymerase chain reaction (RT-PCR) test and enabling testing in medical institutions.1213 The drive-through COVID-19 testing was initially developed in Daegu city and was eventually implemented worldwide, and many other regions and foreign countries followed this testing system.1415 Since then, various local governments have also implemented walk-through COVID-19 test systems.1516
The “test, trace, and treatment (3 Ts)” strategy was the initial response of national government to the COVID-19 outbreak.61213 Epidemiological investigations were performed to track the spread of infection, and rapid-response teams were operated by the local and central governments.6 To date, the crisis has been overcome without a nationwide lockdown.
My colleague and I reported that loss of smell and taste, not well known until then, were the symptoms of COVID-19 and were recognized as the typical symptom of COVID-19.17
The mortality rate in Daegu city had reached 2.5% in the early period of 2020, due to the relatively high virulence of ancestral SARS-CoV-2 and the absence of knowledge of effective treatment.3 The government reported a mortality rate of approximately 2.1% during the first epidemic period.2 Hydroxychloroquine was primarily used as treatment based on the reports of a few studies regarding its effects in vitro.181920 However, no clinical efficacy was reported in several follow-up studies, leading to its exclusion from the preferred drug therapy.2122 Lopinavir/ritonavir was also used during mass outbreaks in Daegu city, but its use was decreased as no clinical effectiveness was observed in several studies.222324
The fight against COVID-19 required intense physical and mental labor and caused burnout among the responders.252627 Nonetheless, they remained steadfast and coped effectively with the challenges brought about by the COVID-19 pandemic; in response to this, the government and the society launched a movement called the “Thank You Challenge”. The COVID-19 epidemic curve was successfully flattened through social distancing due to the efforts of all citizens, the local and central governments, experts, paramedics, and other groups.812
EPIDEMIC SPREAD AND RESPONSE IN KOREA
The Korean government divided the epidemic into five periods.2 The first period covers from January 20 to August 11 (205 days), 2020, which involved the initial outbreak of COVID-19 in Daegu city, Gyeongbuk, and the metropolitan area (Figs. 1 and 2).12 The second period involved the spread of infection in the metropolitan area; the third period nationwide spread; the fourth period spread of the delta variant; and the fifth period spread of the omicron variant from January 30, 2022 to the present (Fig. 2).2
Fig. 2
Changes in cases and SARS-CoV-2 variants in Korea and changes in response policies.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, COVID-19 = coronavirus disease 2019.
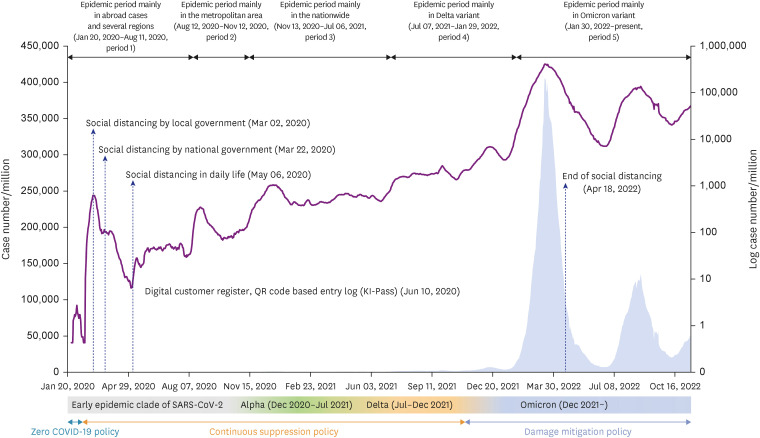
In the second and third periods, local mass outbreaks (those in hospitals and nursing homes) and community infections were common, with case fatality rates of 1.66% and 1.16%, respectively.12 The fourth period mainly involved community infections; from July 7, 2021 to January 19, 2022, the fatality rate was 0.78%.12 The number of confirmed cases increased in the fourth period due to the decrease of the effectiveness of COVID-19 vaccination, the dominance of the delta variant, and the emergence of the omicron variant.12 The mortality rate during the fifth period (January 30, 2022–April 24, 2022) was extremely low (0.1%).2 From the first to the fifth period, local mass outbreaks (those in hospitals and nursing homes) gradually decreased, while community infections increased.2 Hospitals and nursing facilities accounted for a high proportion of cases during the first period, religious facilities in the second period, workplaces in the third period, and educational facilities in the fourth period.12 During the fifth period, a large-scale epidemic occurred throughout the community.2
Although not used during the first period in Daegu city, remdesivir (Gilead Sciences, Foster City, CA, USA), approved for emergency use by the Ministry of Food and Drug Safety in July 2020, was gradually used as the primary treatment drug.1922282930 Later, remdesivir plus steroid (e.g., dexamethasone) was administered to patients with COVID-19 receiving oxygen therapy.2231 Since September 2020, regdanvimab (Celltrion, Seoul, Korea) has been used in high-risk patients who do not require supplemental oxygen therapy to prevent aggravating their condition.323334 Although it was effective against the ancestral virus strains, its effectiveness against the delta variant gradually decreased,35 while it remained ineffective against the omicron variant; hence, this drug was not used since the outbreak of the omicron variant.36 Nirmatrelvir/ritonavir (Pfizer, New York, NY, USA) and molnupiravir (Merck, Kansas City, MO, USA) became available after the end of 2021 and after March 2022, respectively, as antiviral drugs and were recommended to reduce the risk of developing severe COVID-19 among patients with mild to moderate illness.
During the epidemic, those vulnerable to COVID-19, such as pregnant women, dialysis patients, and children, required special medical care.3738394041 The lack of appropriate medical services for these patient groups remained a challenge for bed-assigning teams; hence, efforts are being made to ensure that these patients receive the necessary medical services.
After the first epidemic period in Daegu city, other epidemics have occurred throughout the country; the outbreak of the omicron variant that occurred at the end of 2021 has forced the implementation of at-home care in the spring of 2022.242 Since the omicron outbreak until the present, at-home care is primarily implemented, with the seriously ill patients being treated in the hospitals.
So far, the response policy has been carried out in three stages (zero COVID-19, continuous containment, and damage mitigation policy). “Social distancing” was implemented and emphasized for zero COVID-19 policy and continuous containment policy to contain the epidemic, and the processes in implementing this policy were revised twice until it became a damage mitigation policy.7 The central and local governments have launched disaster relief funds (Emergency Coronavirus Relief Funds) and compensation for small businesses for the damage caused by social distancing. Figure 2 presents the government’s strategy in response to the epidemic caused by the ancestral virus strain and the delta and omicron variants. The omicron variant had a higher potential for airborne transmission among the different variants.4344 However, the severity and fatality rates decreased; thus, the strategy was changed to damage mitigation policy,45 with a focus on protecting the vulnerable groups. After the emergence of the omicron variant, the quarantine measures were eased (removal of social distancing), such as switching from the 3 Ts strategy to the intensive care of high-risk and vulnerable groups and to a general healthcare system (Fig. 2).2
With increased knowledge of the effectiveness of drugs, vaccines, and COVID-19 epidemics, evidence-based decisions were implemented for policy making for fighting COVID-19 from expert advisory groups of central government response teams (such as the Central Disaster and Safety Countermeasures Headquarters, the Central Disaster Management Headquarters, and the Central Disease Control Headquarters).46
The vaccines were introduced late in Korea compared with that in other countries.47 However, potential COVID-19 therapeutic drugs have been quickly introduced. Although the vital role of national health insurance is not generally recognized, it covers the health care expenditures for COVID-related tests and treatments of outpatients and inpatients. It will continue to provide these services in the future. Without Korea’s national health insurance system, it would have been difficult to overcome the crisis.
The elderly patients were most vulnerable to the severe form of COVID-19; hence, protecting and caring for the vulnerable groups were the top priority of the healthcare team. Moreover, participation in vaccination programs and individual quarantine efforts of the family members of the vulnerable groups were required to protect them.4849
With the outbreak of COVID-19, the incidence of mental health problems, including depression, has increased among various populations.2750 From the first COVID-19 outbreak, psychiatric counseling and support have been provided in Korea through a continuous multidisciplinary approach and connection to medical care, if necessary.27
During the omicron outbreak, the risk of death was relatively high in the older population and terminally ill patients. Protecting vulnerable groups (dialysis patients, pregnant women, children, among others) during national epidemic was also important, and an active response was required and performed for COVID-19 patients with severe preexisting medical conditions.49515253 Difficulties arose in assigning beds for SARS-CoV-2 positive patients who needed hospital admission for other problems (e.g., trauma); hence, the collaboration between local governments and medical institutions in charge was of great importance for this patient group.
The government strongly recommended vaccination owing to its proven effectiveness in preventing infection and reducing disease severity; however, the number of side effects (pericarditis, myocarditis, thrombosis, prolonged discomfort, among others) was higher than expected.305455 In addition, its infection prevention effect lasted only 4–6 months.47 For these reasons, the first and second vaccination rates were high, but the third and fourth vaccination rates were relatively low. Nevertheless, vaccination plays a vital role in reducing the incidence and severity of COVID-19 and is the most cost-effective method for reducing the COVID-19 sequelae (long COVID).54 To reduce the infection rate and disease severity in immunocompromised patients for whom vaccination is not effective, antibody therapeutics such as tixagevimab/cilgavimab (Evusheld; AstraZeneca, Cambridge, England) were introduced in July 2022.30
Although the number of COVID-19-related deaths had decreased, the ‘excess deaths’ (the difference between the observed numbers of deaths in specific time periods and expected numbers of deaths) associated with COVID-19 remained high.56 Although not included in the statistics as death due to COVID-19, a high excess mortality rate is related to the fact that COVID-19 will likely worsen the condition of people with comorbidities and elderly patients or cause the failure of appropriate treatments for other diseases.495157
WHAT ARE THE LESSONS?
The infectious disease crisis is not only a medical-related problem but also affects society, economy, education, and culture. Currently, knowledge about SARS-CoV-2 and COVID-19 has improved, and fears related to COVID-19 have gradually subsided owing to the improvement in patient care and the development of effective vaccines. Currently, a negative-pressure bed does not seem absolutely needed to treat patients. However, the generation of infectious aerosols in hospitals by risky procedures (e.g., tracheal suction, high flow oxygen supply, among others) can elevate the chance of nosocomial COVID-19 infections.6 We learned that wearing a mask is the most important method for preventing COVID-19 during a pandemic.5859
During the outbreak in Daegu city, measures such as securing an isolation ward that can treat seriously ill patients, securing dedicated nursing staff to care for ICU patients, improving communication between the central and frontline field, provision of personal protective equipment and infection control materials, and establishment of appropriate risk allowance have been suggested to ensure a continuous response to a resilient pandemic.6061
Within two years after the outbreak, we have learned that COVID-19 cannot be completely controlled,62 and that it is necessary to protect the high-risk group and minimize the damage while maintaining one’s daily life and normalizing the treatment of non-COVID-19 patients.
Table 2 summarizes the future preparations based on the lessons learned during the pandemic.2750636465666768697071
Table 2
Preparation for future COVID-19 outbreaks and new infectious disease crises
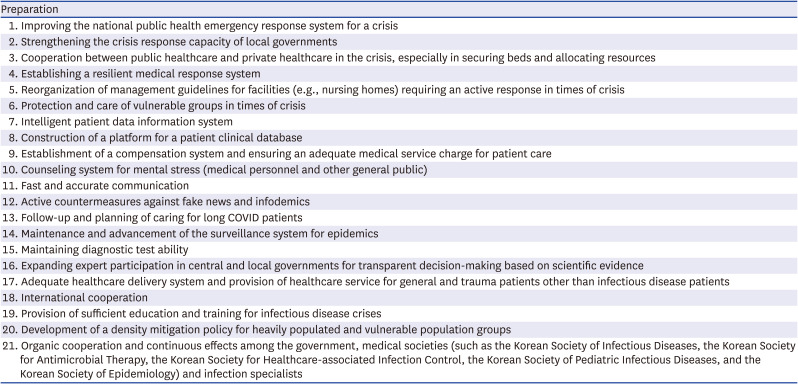
The preparation includes improving the national public health emergency response system for a crisis, strengthening the crisis response capacity of local governments, cooperation between public healthcare and private healthcare in the crisis, especially in securing beds and allocating resources, and establishing a resilient medical response system.6372 Resilience is essential, where strength is provided to respond again by flexibly adjusting the degree of response after facing and overcoming a crisis.6465 Medical institutions need to reestablish patient caring protocols, including patient flow, transport routes, performing confirmational COVID-19 tests, and bed allocation.
The establishment of management guidelines for facilities (nursing hospitals/nursing homes, mental hospitals/mental health facilities, facilities for the disabled, among others) that offer protection, care, and an active response for vulnerable patients (elderly patients, patients with underlying medical conditions, dialysis patients, pregnant women, children, people admitted in psychiatric wards due to mental and psychological disorders, among others) is required.495051525366
To effectively respond to infectious disease crises, an intelligent patient data information system and the construction of a platform for the patient clinical database are necessary to generate scientific evidence and generate databases.67 Medical institutions also need to reestablish policies that include appropriate compensation for all medical personnel and prevent burnout among the medical staff.67 The establishment of a counseling system for mental stress, depression, and lethargy must also be continued,2750 and fast and accurate communication and control of fake news must be implemented continuously.61
Many people develop long COVID after the disease, which causes serious medical and social problems compared with COVID-19.3054687374 Hence, monitoring and follow-up of these patients are needed, and other appropriate medical responses should be given, and additional research is required.69
With the current outbreak of the omicron variant, the number of seriously ill patients has significantly decreased, thus slightly reducing the need for personal protective equipment and infection control materials.677071
Finally, long-term policies are required to reduce the density of the heavily populated facilities for elderly patients, which can lead to minimizing the risk of infectious diseases outbreak.7071
Infectious diseases caused by ribonucleic acid (RNA) viruses are highly lethal, and experts are currently focused on investigating respiratory diseases that can spread through aerosol transmission.7576 COVID-19 is presently the most typical example, with the expected emergence of new variants. At present, the human-infectious form of avian influenza and coronaviruses are the most dangerous type.71 Predicting future trends may be particularly difficult. However, ensuring emergency preparedness in the future is of utmost importance. Preparation by organic cooperation and continuous effects among the government, medical societies (such as the Korean Society of Infectious Diseases, the Korean Society for Antimicrobial Therapy, the Korean Society for Healthcare-associated Infection Control, the Korean Society of Pediatric Infectious Diseases, and the Korean Society of Epidemiology), and infection specialists, are greatly in need.
 XML Download
XML Download