

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Early-onset dementia (EOD) is generally defined as dementia that occurs before 65 years of age as per several previous works of literature.12 As EOD develops at a relatively young age, economic and social activities are more restricted in EOD-affected individuals than in those with senile dementia, and inevitably burdens their families.3 In several previous studies, the prevalence of EOD is reportedly 7–45% among all dementia patients, and the most common type is known as Alzheimer’s disease.45 Recently, as the importance of early screening for dementia has been emphasized, the interest in EOD has also been increasing.6 Thus, it is emerging as an essential topic in healthcare policy.
EOD is considered a relatively heterogeneous disease entity compared to late-onset dementia (LOD) and, of course, has higher mortality than the general population.7 Moreover, EOD is usually more severe and presents with extensive pathologic changes such as greater brain parenchymal atrophy and white matter abnormalities.89 Therefore, EOD progresses relatively quickly, and the mortality risk is higher than that associated with LOD. Despite onset at an earlier age, the average survival time of EOD is less than ten years, similar to that of LOD.10
Socio-environmental determinants have been analyzed in several survival studies as modifiable factors that may be covered to some extent via efforts in healthcare policymaking.1112 The same is valid for dementia survival studies; Korhonen et al.13 reported that low household income was a strong predictor of dementia mortality in a population study based on Finnish data. A prospective cohort study conducted in the Netherlands also associated low household income with higher mortality risks in both male and female patients with dementia.14 Meanwhile, Chen et al.15 demonstrated a greater mortality risk in patients with dementia living in rural areas in a Chinese cohort study. However, these previous studies have primarily focused on typical, senile dementia. Thomas et al.16 conducted EOD-specific mortality studies with social determinants. They conducted a study in Scotland from 1974 to 1988 in patients with Alzheimer’s disease and vascular dementia whose disease onset had occurred before the age of 65 years. Their results revealed that socioeconomic deprivation and urban/rural scores were not significantly associated with survival in patients with EOD. However, recent EOD-related survival studies focusing on socio-environmental factors have been lacking until now.
As shown above, most dementia survival studies have concentrated on typical, senile dementia.4 Furthermore, EOD not only remains poorly understood. but is also insufficiently considered when distributing services and treatment resources related to dementia in terms of healthcare policies. However, patients with EOD must be treated as urgently due to a more aggressive course and relatively large deprivation of social functioning. Through a healthcare management system that not only detects EOD patients early, but also provides appropriate interventions, it is possible to slow the disease progression and maintain each patient’s ability of daily life.17
In this study, we assessed patients with EOD using the National Health Insurance Service (NHIS) database of Korea. We subsequently investigated the effect of socio-environmental factors on the long-term survival of patients with EOD. In particular, we focused on the effect of the imbalance of these factors by identifying the impact of lower household income and rural area residence on the long-term survival of patients with EOD.
METHODS
Study design and participants
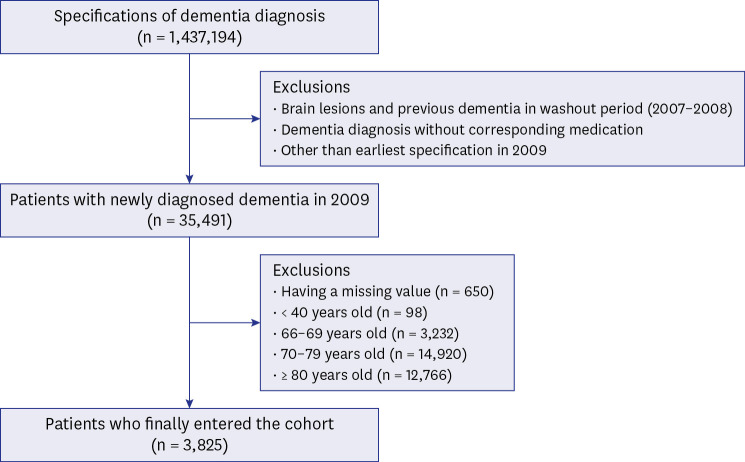
This retrospective, longitudinal cohort study used the Korean NHIS dataset (research management number: NHIS-2020-1-160). Cohort entry was made between January and December, 2009, and the observation period was set until December 31, 2018 (Fig. 1). Our cohort comprised patients aged 40 to 65 years with all types of dementia newly diagnosed in 2009; we defined these patients as EOD cases. The initial sample consisted of 1,437,194 specifications of dementia diagnosis, and we finally included 3,825 patients with EOD. Additionally, we excluded cases with previous brain lesion such as cerebrovascular accidents and traumatic brain injury, those not prescribed medication related to dementia, and having a missing value. The index medication list is presented in Supplementary Table 1. A flowchart of the patient inclusion process is shown in Fig. 2.

Variables and outcome definitions
Our variables of interest were socioeconomic status (SES) and location of residence. SES was defined according to the national health insurance premium (NHIP) levels, charged according to household income. Consequently, all participants were classified into five groups–medical-aid and four quartile groups–according to the NHIP levels (Supplementary Table 2). Based on administrative districts, residential areas were classified into capital, metropolitan, city, and county levels.
Dementia subtypes were defined as Alzheimer’s disease (F00 and G30), vascular dementia (F01), and other types (F02, G3100, and G3182) according to the International Classification of Diseases, 10th Revision (ICD-10) code. Patient comorbidities were identified as the presence of hypertension, diabetes, dyslipidemia, ischemic heart disease, atrial fibrillation/flutter, and chronic kidney disease. We identified the presence or absence of disease codes claimed to the Health Insurance Review and Assessment service for defining the comorbidities. ICD-10 codes for each comorbidity are presented in Supplementary Table 3. We set all-cause death within the observation period as the primary outcome of this study and also identified time to death.
Statistical analysis
All variables were categorized and expressed in terms of frequency (proportion). Subsequently, we performed a χ2 test for comparative analyses between groups. Kaplan-Meier curves and log-rank tests were performed to determine the cumulative survival rate. Cox regression analyses were performed for identifying independent risk factors related to long-term mortality. We used joint tests to determine the interaction between NHIP levels and residential areas. Then, to exclude the interactions, we further established nested and stratified Cox-proportional hazards models. For handling missing data, complete case analysis was performed. Statistical significance was defined as P < 0.05. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Ethics statement
This study was reviewed and approved by the Institutional Review Board of the National Health Insurance Service Ilsan Hospital (NHIS 2022-03-012). Due to the retrospective nature of the study design, informed consent was waived for this study. This study was also performed in compliance with the Declaration of Helsinki. The Korean NHIS database is not publicly available due to privacy and ethical restrictions. The dataset used in this study can only be accessed by authorized researchers through its internal-networking system.
RESULTS
Baseline characteristics
Table 1 summarizes the basic characteristics of patients according to NHIP levels. The proportion of older adults was higher in the higher NHIP groups, whereas the medical-aid group had a relatively younger age distribution (P < 0.001). In the lower NHIP level group, the male to female ratio tended to be high (P < 0.001). There was a difference in the residential area according to income level. In the medical-aid group, the proportion of residents living in the county region was the highest. Contrastingly, in the fourth NHIP quartile group, the percentage of patients living in the capital region was the highest (P < 0.001). There were significant differences between groups in the distribution of dyslipidemia (P < 0.001) among comorbidities. The distribution of dementia subtypes and other comorbidities did not significantly differ between groups.
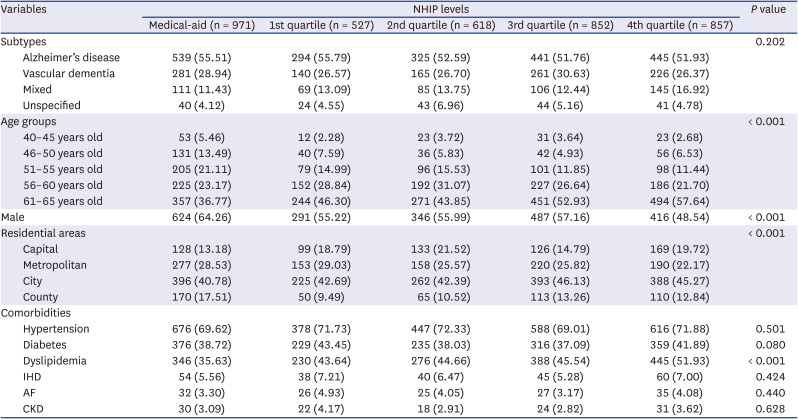
Table 1
Baseline characteristics of patients according to the NHIP level groups
Values are presented as number (%).
NHIP = national health insurance premium, IHD = ischemic heart disease, AF = atrial flutter/fibrillation, CKD = chronic kidney disease.
![]()
When comparing the patients between residential area groups, there was a significant difference in the distribution of NHIP levels (P < 0.001) with the frequency of the fourth quartile NHIP level being the highest in capital residents. Conversely, the proportion of the medical-aid group was highest in county residents. Dyslipidemia prevalence was highest in the capital and lowest in metropolitan areas (P = 0.003). There were no significant differences between groups regarding dementia subtypes, age and gender distributions, and other comorbidities (Supplementary Table 4).
Survival analysis and Cox-proportional hazards models
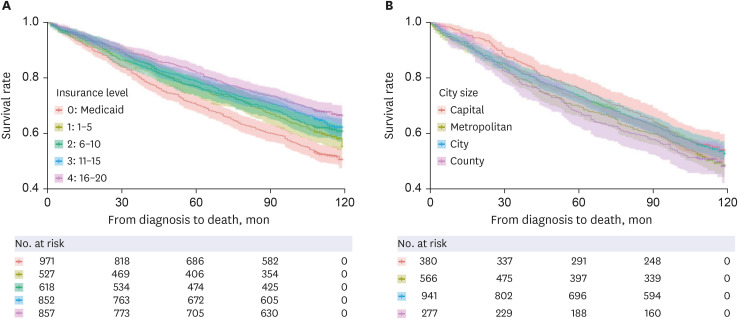
Cumulative survival analyses revealed a significant difference in survival rates according to income quintile and residential area in patients with EOD (P < 0.001 and P = 0.035, respectively) (Fig. 3). The average survival period of the fourth NHIP level group was 96.31 ± 1.20 months, whereas that of the medical-aid group was 85.53 ± 1.30 months. Patients living in the capital had a mean survival of 95.73 ± 1.34 months, whereas those living in the county had 89.66 ± 1.75 months.
We established Cox-proportional hazards models with 3,535 subjects after removing 290 observations due to missing data; then, we found 1,413 events (death). The model revealed that the medical-aid group (adjusted hazard ratio [aHR], 1.67; 95% confidence interval [CI], 1.43–1.94; P < 0.001), first NHIP level group (aHR, 1.26; 95% CI, 1.05–1.50; P = 0.012), and second NHIP level group (aHR, 1.26; 95% CI, 1.06–1.50; P = 0.008) were significantly associated with a higher long-term mortality risk. By residential area, the capital area was associated with a significantly lower long-term mortality risk than was the county region (aHR, 0.82; 95% CI, 0.68–0.99; P = 0.041). Moreover, patients in the older age group and with diabetes, ischemic heart disease, and chronic kidney disease exhibited a significantly higher long-term mortality risk. Conversely, dyslipidemia was associated with significantly lower mortality risk (Table 2).
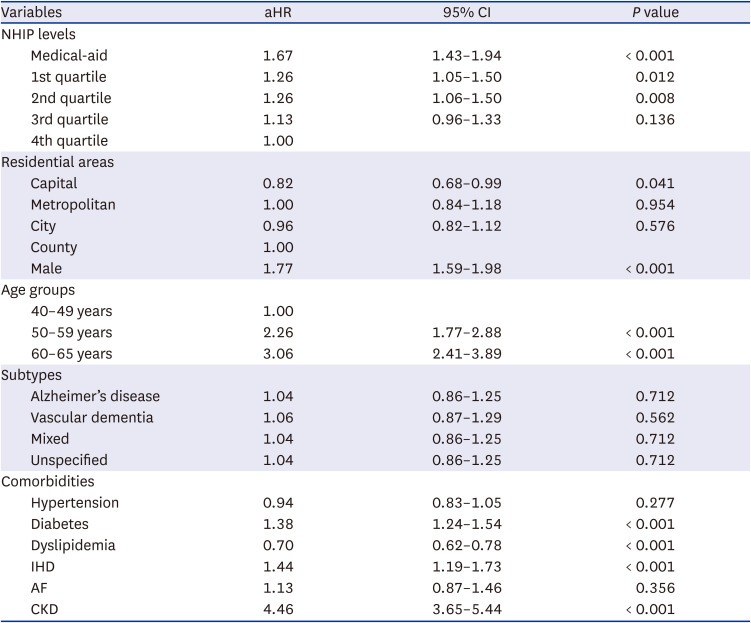
Table 2
The entire Cox-proportional hazards model
aHR = adjusted hazard ratio, CI = confidence interval, NHIP = national health insurance premium, IHD = ischemic heart disease, AF = atrial flutter/fibrillation, CKD = chronic kidney disease.
![]()
We confirmed interactions between the NHIP levels and residential areas (P = 0.026). To confirm each primary variable’s independent effect on long-term survival, we further established nested Cox-proportional hazards models. In the nested model excluding residence area from the variables, the medical-aid group along with the first and second NHIP level groups was associated with a significantly higher long-term mortality. In the nested model excluding NHIP levels as variables, the group of patients living in the capital were also associated with a significantly lower long-term mortality risk than those of their counterparts in the county region (Table 3). Stratified Cox regression analyses revealed that capital residents showed a significantly reduced risk of long-term mortality of EOD (aHR, 0.39; 95% CI, 0.24–0.63; P < 0.001) in the second NHIP level group. However, in the other NHIP groups, there was no significant difference in the risk of chronic mortality according to the residential areas (Table 4).
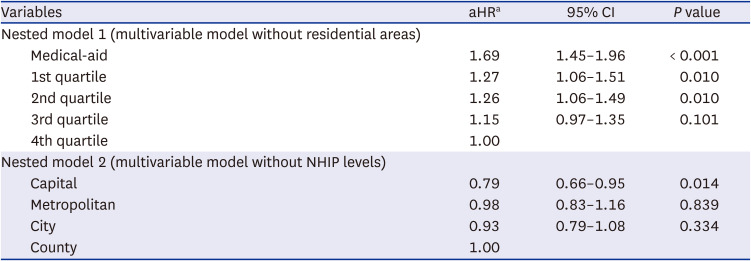
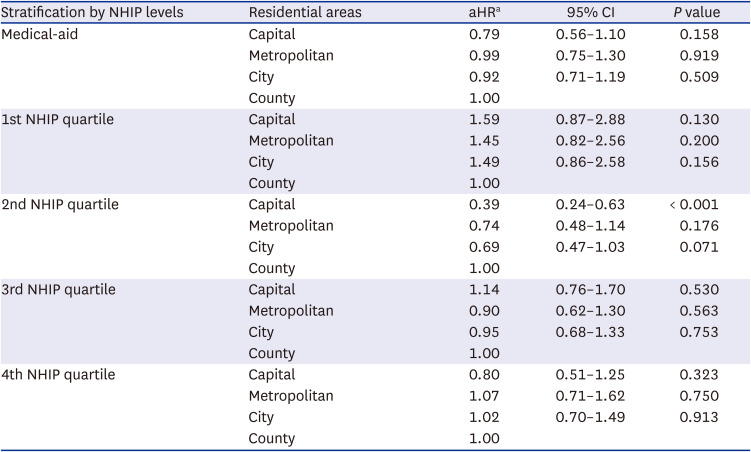
Table 3
Nested Cox-proportional-hazards models according to each variable of interest
aHR = adjusted hazard ratio, CI = confidence interval, NHIP = national health insurance premium.
aAdjusted for age, gender, dementia subtypes, and comorbidities.
![]()
Table 4
Stratified Cox-proportional hazards models
NHIP = national health insurance premium, aHR = adjusted hazard ratio, CI = confidence interval.
aAdjusted for age, gender, dementia subtypes, and comorbidities.
![]()
DISCUSSION
This study establishes lower household income and rural residence as independent risk factors for increasing long-term mortality risk in patients with EOD in Korea. The nested models to exclude the interaction effect between the NHIP levels and residential areas also revealed the same results. Further, in the stratified models by NHIP levels, we confirmed that the residential areas significantly affect the long-term mortality of patients with EOD only in the second NHIP quartile group. Our study is significant because it investigated the effects of socio-environmental factors on long-term survival by focusing on the EOD patient group. As the first survival study of EOD using Korea’s NHIS database, another strength of this study is that it was possible to objectively obtain information on patients' SES levels and residential areas.
It should be noted that our definition of patients with EOD was somewhat different from those used in previous studies because information on symptom onset was unavailable due to the nature of the NHIS database. Since we enrolled patients diagnosed with dementia at the age of 40–65 years, they would have an earlier onset time than the EOD patient group generally defined in other studies. According to van Vliet et al.,18 it took approximately 4.4 years from symptom onset to diagnosis in patients with EOD; therefore, when interpreting our results, this time difference should be considered. Moreover, we inferred that the proportion of patients with a different phenotype from that of senile dementia would be higher than that observed in other studies due to the earlier onset.1920 Finally, symptom onset has a subjective aspect, but the timing of diagnostic confirmation from a physician is objective information. Therefore, we also demonstrate that the patient composition of our study adequately reflects the characteristics of EOD.
We can suggest that the primary reason for the lower long-term mortality risk in higher income and urban resident groups is the difference in medical access and healthcare availability. These influenced the difference in the period from symptom onset to that of diagnosis in individual patients; the higher the income accompanied by urban residence, the shorter the period between disease onset and diagnosis. Conversely, in the case of patients with low-income levels and rural area residence, the time from symptom onset to diagnosis might have been relatively long; therefore, we can infer that it might have been associated with a high long-term mortality risk due to the more prolonged prevalence of the disease. These differences in medical access are also indirectly identified via the rates of non-critical comorbidities such as hypertension, diabetes, and dyslipidemia.2122 In our results, the rates of these chronic diseases tended to be lower in the low-income group and rural residents. However, the high prevalence of these chronic conditions in the high-income and urban residence groups may, paradoxically, be associated with higher medical availability for these diseases.23
Meanwhile, most of the population in Korea lives in or around the city area with a high population density, and the country has relatively convenient and sufficient transportation facilities.24 We suggest this as one of reasons why the risk of chronic phase mortality of patients with EOD according to the residential area was relatively less significant compared to household income level. Meanwhile, in explaining the differences in outcomes of EOD by residential areas, the authors suggest that differences in the healthcare-seeking behavior of members according to regional differences as well as healthcare resource availability could affect the results of this study. When patients entered the cohort, the proportion of those in their 60s was the highest in the county; this difference in age composition might have led to a difference in healthcare-seeking behavior. In addition, we inferred that the differences in the patient’s invisible educational level depending on the residential area, which was not presented in this study, might have caused the difference in healthcare-seeking behavior.
Similarly, differences in income levels can also have a significant impact on the healthcare-seeking behavior.25 Though Korea provides universal health coverage under the NIHS system, some examination and treatment items are still not covered by the NHIS. Therefore, it was highly likely that patients with low-income levels did not properly receive examinations or treatments that NHIS did not cover in a timely manner. In addition, indirect costs such as transportation fees required to move to urban areas are inevitably felt as a significant burden to low-income people living in rural areas.26 Consequently, we could confirm through the results of this study that, in general, the risk of chronic mortality in patients with EOD was more affected by the household income level under the Korean NHIS system.
Another noteworthy point from our results was that the age at diagnosis with dementia tended to be lower in the medical-aid group. The fact that although the medical-aid group had a relatively younger age distribution, they had a high long-term mortality risk suggested that a low-income level was a strong predictor for long-term mortality risk in patients with EOD. From another perspective, the proportion of patients with atypical pathology distinct from senile dementia in the medical-aid group was high. Therefore, it can be interpreted that their disease course was relatively fatal.727
In South Korea, national-level efforts are ongoing to resolve such SES and regional disparities in patients with dementia. Since 2017, the national responsibility system for dementia has been introduced,28 and 256 Local Dementia Centers are in operation as of 2019.29 Local Dementia Centers are based in public health centers in each region and aim to provide screening and diagnostic tests for early diagnosis of dementia at low prices. This enables the improvement in the quality of managing patients with dementia and the minimization of the difference in access to medical institutions due to regional and income disparities. Future studies on the effectiveness of these policy-based efforts in patients with EOD are needed.
Meanwhile, studies have assessed the survival determinants targeting patients with EOD. A five-year longitudinal study conducted by Ueki et al.30 on patients with early-onset Alzheimer's disease found that male sex, early-onset disease, concurrent physical illness, and low mini-mental state examination score were related to mortality risk. Conversely, Thomas et al.16 reported that increased age at presentation was significantly related to long-term mortality in early-onset Alzheimer's disease and vascular dementia patients. In our study, male gender, older age at diagnosis, and several comorbidities, such as diabetes, ischemic heart disease, and chronic kidney disease, were identified as independent risk factors for long-term mortality in patients with EOD, consistent with previous studies.
Some limitations of this study as follows. The NHIS database did not provide detailed clinical information such as educational level, degree of initial cognitive impairment, psycho-behavioral symptoms, and daily life performance. Therefore, we could not provide information to estimate the disease severity at the time of diagnosis of EOD. Similarly, the dataset could not accurately indicate the time of symptom onset. Therefore, our inability to specify the period from symptom onset to diagnosis was a limitation. Finally, we did not present the cause of death.
In conclusion, lower household income levels and rural residence are associated with long-term mortality risk in patients with EOD in South Korea. The authors suggest that these socio-environmental factors influence healthcare facility availability and health-seeking behavior, leading to these results. An imbalance in socio-environmental factors can be overcome to some extent via policymaking efforts, and our study results provide a rational basis for establishing a healthcare policy for patients with EOD. For the efficient management of patients with EOD, nationwide policy-based support as well as additional related research are needed.
 XML Download
XML Download